At a glance
- Prescription retatrutide has no cost because it does not exist: FDA-approved for zero indications in 2026.
- Grey-market research vials run roughly $200-500 monthly, unregulated and not the trial formulation.
- Compounded tirzepatide or semaglutide via telehealth starts near $129/mo, prescribed and supervised.
- Retatrutide hit 24.2% weight loss at 48 weeks; approved GLP-1s deliver 15-21% you can buy today.
Type "retatrutide cost" into Google and you are asking a question with no honest retail answer. There is no pharmacy shelf price, no insurance copay, no LillyDirect self-pay tier. Retatrutide is Eli Lilly's investigational triple agonist. As of July 2026 the FDA has approved it for nothing, no pharmacy can fill it, and no clinician can legally prescribe it.
So where do all the "cost" numbers people trade online come from? The grey market. When you see "$180 a vial" or "$12 a milligram" quoted in a forum, that is research-use-only powder sold under a lab-use disclaimer, not a medicine with a price. This guide separates the two: what retatrutide would theoretically cost if it existed as a drug, what the grey market actually charges, and what the supervised alternative you can buy this afternoon runs per month.
If you want the sourcing and vendor side instead of the pricing side, that lives in the retatrutide where-to-buy guide. This page is strictly about money.
Bottom line: You cannot legally buy prescription retatrutide at any price in 2026. The only real "retatrutide cost" is grey-market research material, which is unregulated. If your goal is supervised weight loss now, a prescribed compounded GLP-1 starts around $129/mo and is the honest answer to what you are actually trying to buy.
Why there is no legitimate retatrutide price
A drug gets a price when it gets an approval. Approval creates a manufacturer, a wholesale acquisition cost, pharmacy dispensing, and eventually insurance and cash-pay tiers. Retatrutide has none of that yet.
The data behind the hype is real. In the Phase 2 obesity trial, retatrutide produced 24.2% mean body weight reduction at 48 weeks on the 12 mg dose, the largest signal any incretin had posted in a peer-reviewed obesity trial to that point (Jastreboff et al. 2023). Lilly's TRIUMPH Phase 3 program read out across obesity and type 2 diabetes, and an FDA submission is widely expected on the back of it. A plausible label launch lands in 2027 at the earliest.
Until that happens, three things are true and worth saying plainly:
- No compounding pharmacy can legally compound retatrutide. There is no approved reference drug and it is not on the FDA 503A bulk substances list.
- No telehealth service can legally prescribe it. Any site quoting a "retatrutide prescription" is almost always routing you to compounded tirzepatide or semaglutide under a misleading label. Ask which pharmacy fills it; the answer tells you what you are really buying.
- Every legitimate vendor that ships retatrutide sells it as research material, not for human use.
That is the entire reason "retatrutide cost" searches bounce straight into the grey market.
The grey-market reality (described, not endorsed)
Research-peptide vendors sell lyophilized retatrutide in vials sized by milligram, commonly 10 mg and 30 mg. The pricing you see quoted online reflects those vials, and after typical research-vendor discount codes it tends to land in a rough band:
- A 10 mg vial: roughly $90-180 before discounts.
- A 30 mg vial: roughly $250-450 before discounts.
Translate that to a monthly figure and the math gets slippery, because the trial titrated from 2 mg per week up to 12 mg per week. At the top of that ramp you are using about 48 mg a month, so a "monthly cost" for research retatrutide realistically spans $200 to $500 or more depending on your dose and vendor. Codes like ENHANCED cut roughly half off some catalogs, which is why the quoted numbers swing so widely.
But price is the least important thing about this material.
Warning: Grey-market retatrutide is not the Lilly trial formulation. It is synthesized by third-party labs, sold research-use-only, and is not intended for human consumption. Purity, sterility, and actual peptide content vary by vendor and by lot. A cheap per-milligram price tells you nothing about what is in the vial. If you go this route, a per-lot HPLC certificate of analysis matching the vial lot number is the floor for trust, and even then you are dosing an unapproved drug with no clinician, no titration support, and no accountability if something goes wrong. Side effects are real: see the retatrutide side effects breakdown before you assume "cheap" means "low risk."
Cheap is not the same as safe, and unregulated is not the same as free of cost. The cost you cannot see on the invoice is the one that matters most.
The honest cost comparison
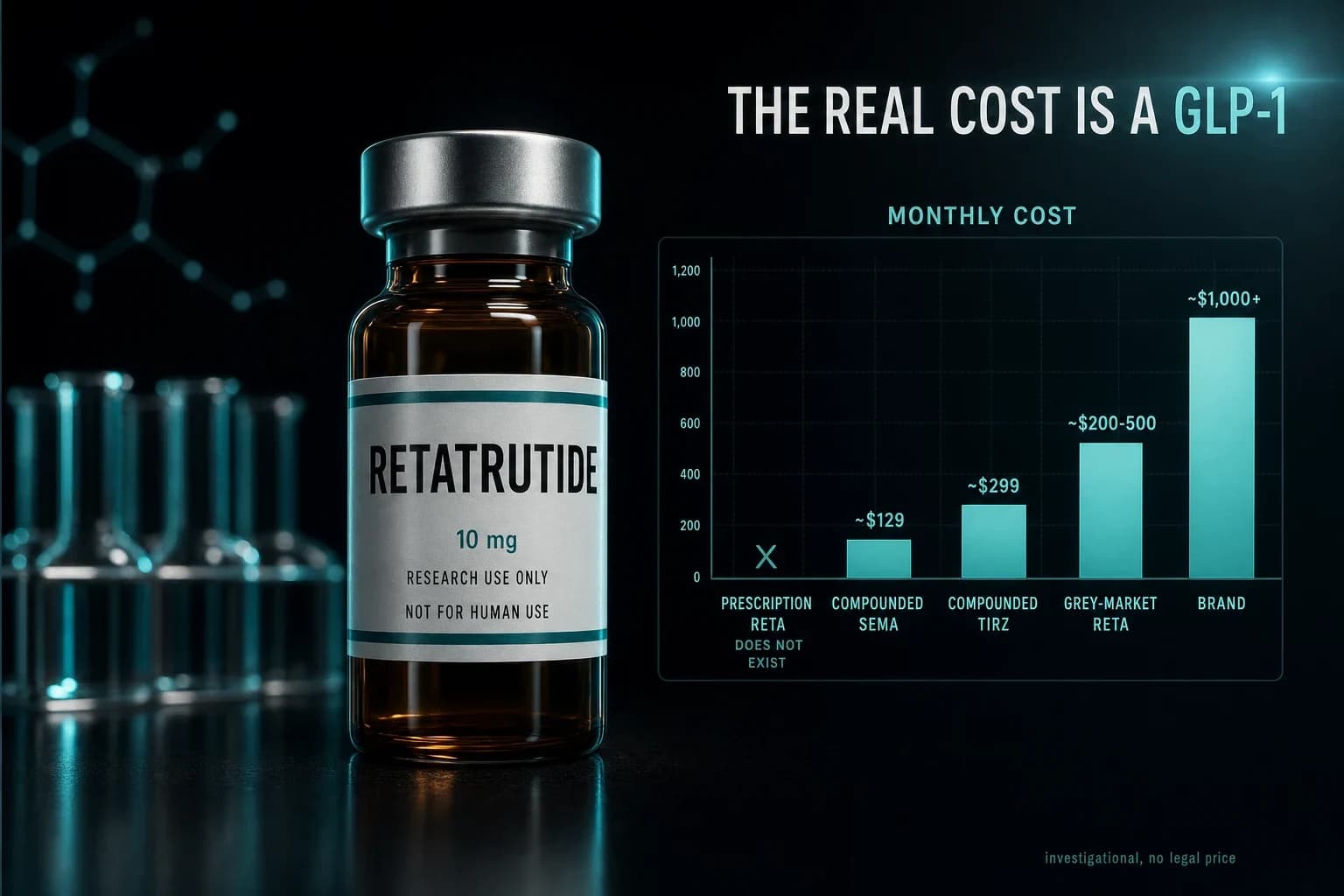
Here is every path someone Googling "retatrutide cost" is actually weighing, with a rough monthly figure and the one column most guides skip: whether it is legitimate.
| Option | What it is | Rough monthly cost | Legit? |
|---|---|---|---|
| Prescription retatrutide | FDA-approved retatrutide from a pharmacy | Does not exist in 2026 | No such product |
| Grey-market research retatrutide | Lab-use-only vials, not for human use | ~$200-500+ | Not for human use, unregulated |
| Compounded semaglutide (telehealth) | Prescribed GLP-1, US pharmacy-filled | From ~$129/mo | Yes, supervised |
| Compounded tirzepatide (telehealth) | Prescribed GIP/GLP-1 dual agonist | ~$199-349/mo | Yes, supervised |
| Brand Zepbound / Wegovy | FDA-approved GLP-1s, self-pay | ~$499-1,350/mo | Yes, but priciest |
The table makes the trade obvious. The only rows you can legally use as medicine are the approved GLP-1s. And the cheapest legitimate row starts well below what a full research-retatrutide protocol would cost you anyway.
The alternative most people are actually shopping for
Strip away the molecule name and what "retatrutide cost" shoppers usually want is simple: significant, supervised weight loss at a price that is not brand-name insane. That product exists today, it is just not retatrutide.
Retatrutide's headline was 24.2% at 48 weeks (Jastreboff et al. 2023). The approved incretins are not far behind and you can actually get them. Tirzepatide produced 20.9% body weight reduction at 72 weeks on the 15 mg dose in SURMOUNT-1 (Jastreboff et al. 2022). Semaglutide produced 14.9% at 68 weeks in STEP 1 (Wilding et al. 2021). Those are real numbers from real trials, and both drugs are prescribable now.
The route that lands closest to the "cheap and supervised" sweet spot is compounded GLP-1 through telehealth. You complete an online intake, a US-licensed clinician reviews your history and eligibility, and if it is appropriate a compounding pharmacy fills the prescription and ships it to your door. No in-person visit, no insurance required, and pricing that undercuts brand by a wide margin. Programs like Yucca Health run exactly this model, starting from around $129 a month, which is why it is the path we point most cost-conscious readers toward.
For the full ranking of legitimate low-cost options by real per-month price, see the cheapest GLP-1 guide. For the dual-agonist path specifically, which is the closest approved cousin to retatrutide's mechanism, compounded tirzepatide online covers what supervised access looks like and what it runs.
Frequently asked cost questions
How much does retatrutide cost per month?
There is no legitimate monthly price because retatrutide is not approved or prescribable in 2026. Grey-market research vials work out to roughly $200-500 a month at trial-level doses, but that is unregulated lab material sold research-use-only, not a medicine you can legally take. A prescribed, supervised compounded GLP-1 starts near $129 a month and is the real answer to the cost question most people are asking.
Why is retatrutide so much cheaper than Wegovy or Zepbound online?
Because the cheap "retatrutide" online is not a finished, FDA-regulated drug. It is research powder with no sterility guarantee, no clinician, and no manufacturer standing behind it. Brand GLP-1s cost more because they are approved, sterile, dose-verified pharmaceuticals. You are not comparing two prices for the same thing.
Can I get retatrutide covered by insurance?
No. Insurance covers approved drugs with a valid prescription. Retatrutide has neither. Even approved GLP-1s face heavy coverage restrictions, which is why most people use cash-pay compounded routes. See the cheapest GLP-1 breakdown for what actually clears without insurance.
Is grey-market retatrutide worth the price?
Price is the wrong lens. You are buying an unapproved drug with no medical oversight and lot-to-lot variability in purity and content. If you are set on retatrutide anyway, a per-lot HPLC certificate matching your vial is the minimum, and the where-to-buy guide covers verification. But for supervised weight loss at a lower all-in cost, a prescribed GLP-1 is the better value.
What is the cheapest legitimate way to lose weight on a GLP-1 right now?
Compounded semaglutide through telehealth is usually the lowest legitimate entry point, from around $129 a month, with compounded tirzepatide a step up for the stronger dual-agonist data. Both are prescribed and supervised. The cheapest GLP-1 guide ranks every option by real monthly cost.
Where to go from here
If you came for a retatrutide price and left understanding there is not one yet, that is the correct takeaway. The mechanism is genuinely ahead of the field, and the retatrutide research guide and retatrutide dosage chart cover it in full for when approval lands. Until then, the honest move is a supervised GLP-1 you can actually buy. Compare real monthly pricing on the cheapest GLP-1 guide, or start an intake with Yucca Health to see what a prescribed program costs for your situation.
This article is for educational purposes only and is not medical advice. Retatrutide is investigational, is not FDA-approved as of July 2026, is not available by prescription, and is not for human consumption. Weight-loss figures reflect published clinical trials of the compounds named; individual results vary. Consult a qualified clinician before starting any GLP-1 program.


