At a glance
- In the only head-to-head obesity trial, STEP 8 (PMID 35015037), semaglutide 2.4 mg cut body weight 15.8% vs 6.4% for liraglutide 3.0 mg at 68 weeks, a 9.4-point gap.
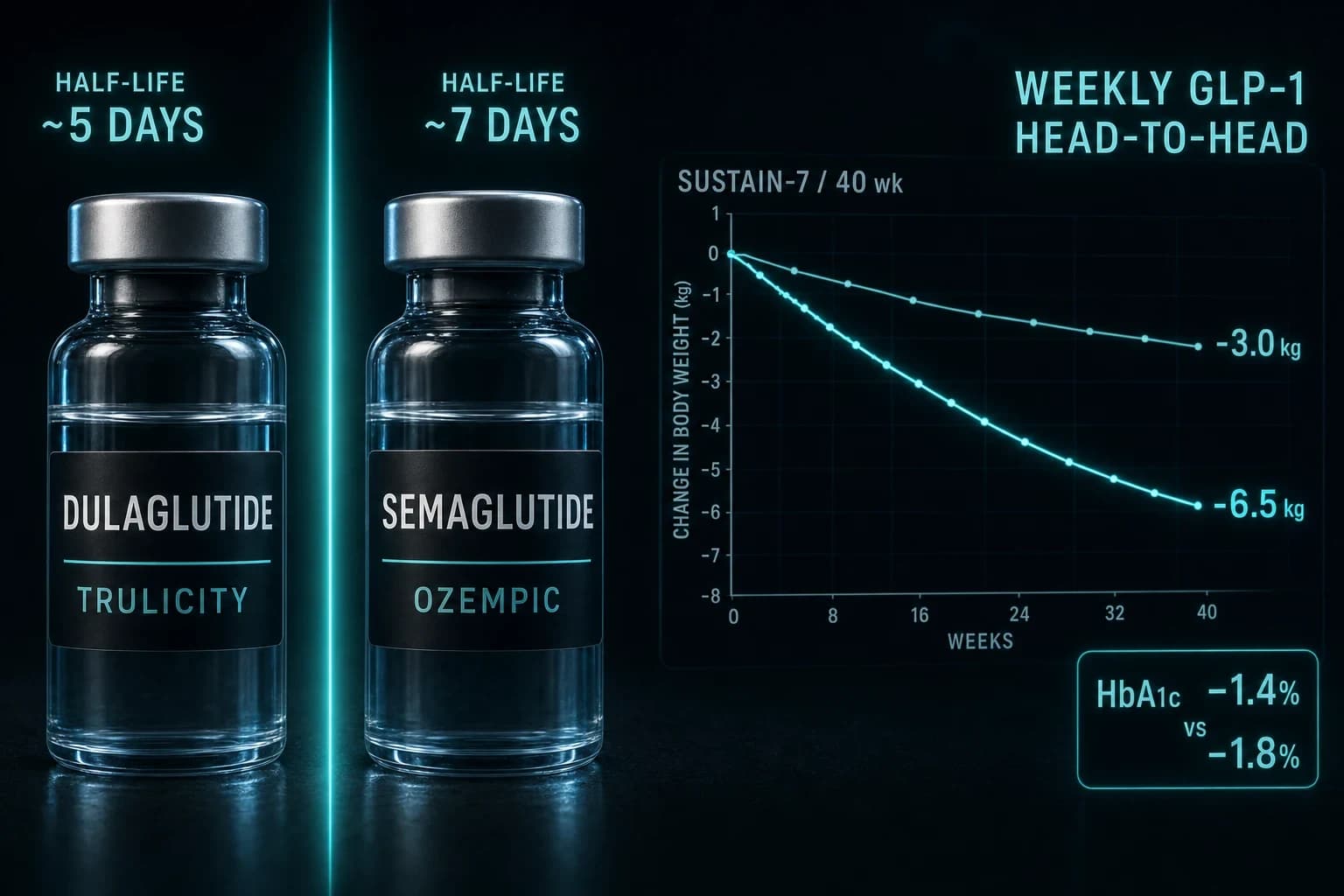
- Liraglutide clears with a ~13-hour half-life (once-daily injection); semaglutide's ~165-hour (~7-day) half-life allows once-weekly dosing.
- Both lower cardiovascular events in type 2 diabetes: LEADER put liraglutide MACE at HR 0.87, SUSTAIN-6 put semaglutide at HR 0.74.
- On its own, liraglutide 3.0 mg (SCALE, PMID 26132939) averaged about 8% weight loss vs semaglutide 2.4 mg's 14.9% in STEP 1.
- Even at diabetes doses, SUSTAIN 10 showed weekly semaglutide 1.0 mg beat daily liraglutide 1.2 mg: 5.8 kg lost vs 1.9 kg.
Put semaglutide 2.4 mg and liraglutide 3.0 mg into the same 68-week trial and the gap looks almost unfair. Semaglutide took 15.8 percent of body weight off. Liraglutide managed 6.4 percent. That is the headline from STEP 8, and it is why most clinicians treat these two drugs as different generations rather than close alternatives. They come from the same lab, hit the same receptor, and share a single design trick. The difference is what one small change to that trick did to potency and dosing.
This is the full comparison: mechanism, half-life, the head-to-head numbers, cardiovascular data, tolerability, and where each drug still makes sense.
Same receptor, two different molecules
Both liraglutide and semaglutide are GLP-1 receptor agonists. They copy the gut hormone glucagon-like peptide-1, which in its native form lasts about two minutes before the enzyme DPP-4 breaks it down. Both drugs dodge that fate by attaching a fatty acid chain that binds tightly to albumin, the most abundant protein in blood. Albumin acts as a slow-release reservoir, dripping the drug back into circulation over hours to days.
The size of that fatty acid chain is most of the story. Pi-Sunyer et al. (2015) describe liraglutide with a C16 palmitic acid link that produces roughly 97 to 99 percent albumin binding and a half-life near 13 hours. Semaglutide swaps in a longer C18 fatty diacid on a spacer and adds an amino acid substitution (Aib at position 8) that further shields it from DPP-4. The result is a half-life around 165 hours, close to seven days. That single engineering change is why one drug needs a daily needle and the other needs a weekly one.
Both slow gastric emptying, blunt appetite through receptors in the hypothalamus and brainstem, and improve insulin secretion in a glucose-dependent way, so neither causes low blood sugar on its own. You can read the full receptor and dosing profiles on our liraglutide and semaglutide pages.
Liraglutide vs semaglutide at a glance
| Feature | Liraglutide | Semaglutide |
|---|---|---|
| Brands (obesity / diabetes) | Saxenda / Victoza | Wegovy / Ozempic |
| Mechanism | GLP-1 receptor agonist | GLP-1 receptor agonist |
| Half-life | ~13 hours | ~165 hours (~7 days) |
| Dosing | Once daily, up to 3.0 mg | Once weekly, up to 2.4 mg |
| Avg weight loss (obesity dose) | ~6 to 8% | ~15% |
| CV outcome in T2D | MACE HR 0.87 (LEADER) | MACE HR 0.74 (SUSTAIN-6) |
| Best use | Dose flexibility, faster side-effect washout, longest CV record | Maximum weight loss, weekly convenience |
STEP 8: the only real head-to-head for weight
Most drug comparisons are indirect. You line up two separate trials and hope the populations matched. STEP 8 skipped that problem by randomizing the same population to both drugs. Rubino et al. (2022) enrolled 338 adults with overweight or obesity and no diabetes, assigning them to once-weekly semaglutide 2.4 mg or once-daily liraglutide 3.0 mg for 68 weeks, both alongside diet and activity counseling.
The mean weight change was 15.8 percent with semaglutide versus 6.4 percent with liraglutide, a difference of 9.4 percentage points. The milestone data made the gap concrete:
- 10 percent or more lost: 70.9 percent of the semaglutide group versus 25.6 percent on liraglutide
- 15 percent or more: 55.6 percent versus 12.0 percent
- 20 percent or more: 38.5 percent versus 6.0 percent
More than a third of semaglutide patients hit 20 percent weight loss. Fewer than one in fifteen liraglutide patients did. Gastrointestinal side effects, mostly nausea, were common with both and were the leading reason people stopped either drug.
Bottom line: For weight loss alone, this is not a close call. At their approved obesity doses, semaglutide 2.4 mg roughly doubled to tripled the result of liraglutide 3.0 mg in the same trial.
What each drug does on its own
STEP 8 lines up with the standalone approval trials. In SCALE Obesity and Prediabetes, Pi-Sunyer et al. (2015) randomized 3,731 adults to liraglutide 3.0 mg or placebo for 56 weeks. The liraglutide group lost a mean of 8.4 kg versus 2.8 kg on placebo, about 8 percent of starting weight, and 63 percent of them lost at least 5 percent. That trial is the basis for Saxenda's obesity approval, and it also showed more patients reverting from prediabetes to normal glucose.
Semaglutide's equivalent is STEP 1. Wilding et al. (2021) ran 1,961 adults on semaglutide 2.4 mg or placebo for 68 weeks and reported a mean loss of 14.9 percent versus 2.4 percent. Different trials, different lengths, but the pattern is the same one STEP 8 confirmed directly: liraglutide clusters near 6 to 8 percent, semaglutide near 15 percent.
Cardiovascular outcomes: closer than the weight data
Weight is where semaglutide dominates. Cardiovascular protection is where the two drugs look more alike, and where liraglutide holds the longer track record. Both were tested in large outcome trials in people with type 2 diabetes at high cardiovascular risk.
LEADER studied liraglutide. Marso et al. (2016) followed 9,340 patients and found major adverse cardiovascular events (cardiovascular death, nonfatal heart attack, nonfatal stroke) in 13.0 percent on liraglutide versus 14.9 percent on placebo, a hazard ratio of 0.87 and a statistically significant reduction. SUSTAIN-6 tested semaglutide at diabetes doses. A separate report from Marso et al. (2016) recorded events in 6.6 percent on semaglutide versus 8.9 percent on placebo, a hazard ratio of 0.74.
The point estimate favors semaglutide, but SUSTAIN-6 was smaller and designed to rule out harm rather than to prove benefit, so the two numbers are not cleanly comparable. What matters for a reader choosing a drug: both lower cardiovascular risk in diabetes, and liraglutide's benefit was confirmed in a larger, longer, dedicated outcomes trial.
Even at diabetes doses, weekly wins
STEP 8 used obesity doses. SUSTAIN 10 asked the same question at the doses people with type 2 diabetes actually take. Capehorn et al. (2020) randomized 577 patients to weekly semaglutide 1.0 mg or daily liraglutide 1.2 mg on top of oral drugs. HbA1c fell 1.7 percent with semaglutide versus 1.0 percent with liraglutide. Body weight dropped 5.8 kg versus 1.9 kg. Semaglutide won on glucose and on weight at every threshold tested, with a similar safety profile aside from slightly more gastrointestinal complaints. The efficiency gap holds whether you dose for diabetes or for obesity.
Tolerability: same side effects, different exit speed
The side effect that ends most GLP-1 courses is gastrointestinal: nausea, vomiting, diarrhea, constipation. Both drugs cause it, and in STEP 8 the rates were broadly similar, with gastrointestinal complaints the most common adverse event and the top reason for stopping either drug. Slow titration is the standard fix, which is why Wegovy takes four to five months to reach 2.4 mg and Saxenda ramps over five weeks.
The half-life changes how you manage a bad reaction. If liraglutide makes someone miserable, the roughly 13-hour clearance means the drug is largely gone within a day of the last dose. Semaglutide's seven-day half-life means a rough week stays rough, and a held dose still lingers. That is a genuine point in liraglutide's favor for anyone unusually sensitive to nausea or brand new to the class. Pancreatitis is a rare labeled risk for both, and both carry a thyroid C-cell tumor warning based on rodent data, so a personal or family history of medullary thyroid carcinoma rules out either drug.
Daily needle versus weekly needle
Potency is not the only variable that decides real-world results. A drug only works if people keep taking it, and here the schedules split sharply. Liraglutide, sold as Saxenda for obesity and Victoza for diabetes, is injected once daily and titrated up over five weeks from 0.6 mg to 3.0 mg. Semaglutide, sold as Wegovy for obesity and Ozempic for diabetes, is injected once weekly and titrated over 16 to 20 weeks to a maximum of 2.4 mg.
Daily dosing is not automatically worse. Some people prefer a fixed daily habit. But 365 injections a year versus 52 is a real difference in burden, and long-term persistence data tends to favor the weekly option. If you are reconstituting research-grade material rather than using a prefilled pen, our reconstitution calculator handles the dosing math for either half-life.
Cost, access, and the research-grade route
Brand pricing is the other reason people compare these two. Saxenda and Wegovy both carry list prices well over 1,000 dollars a month in the US without insurance, and coverage for obesity remains inconsistent.
For readers comparing costs, research-grade semaglutide from Ascension Peptides runs a small fraction of brand pricing, and code ENHANCED takes 50 percent off. It is sold for laboratory research use, not as a prescription product. If you want a legitimate prescription without paying full brand price, the telehealth and compounded options in our cheapest GLP-1 guide lay out what is currently available and roughly what each path costs.
Which one, and for whom
Bottom line: If the goal is maximum weight loss and you can get semaglutide, it is the stronger choice on every efficacy measure, and the weekly injection is easier to sustain. Liraglutide still earns its place when someone wants dose flexibility, values a shorter half-life for managing side effects, needs the longest-running cardiovascular outcomes data, or simply has access to it and not to semaglutide.
Neither is the ceiling anymore. Tirzepatide, the dual GIP and GLP-1 agonist, outperformed semaglutide in its own head-to-head, so read the tirzepatide profile before you commit to either older drug.
Research-only note: the information here is educational and describes clinical-trial data. Liraglutide and semaglutide are prescription drugs. Research-grade material sold by peptide vendors is intended for laboratory research only and is not for human use. Talk to a licensed clinician before starting, stopping, or changing any GLP-1 medication.