At a glance
- GLP-3 is not a real hormone or drug class. No such receptor exists.
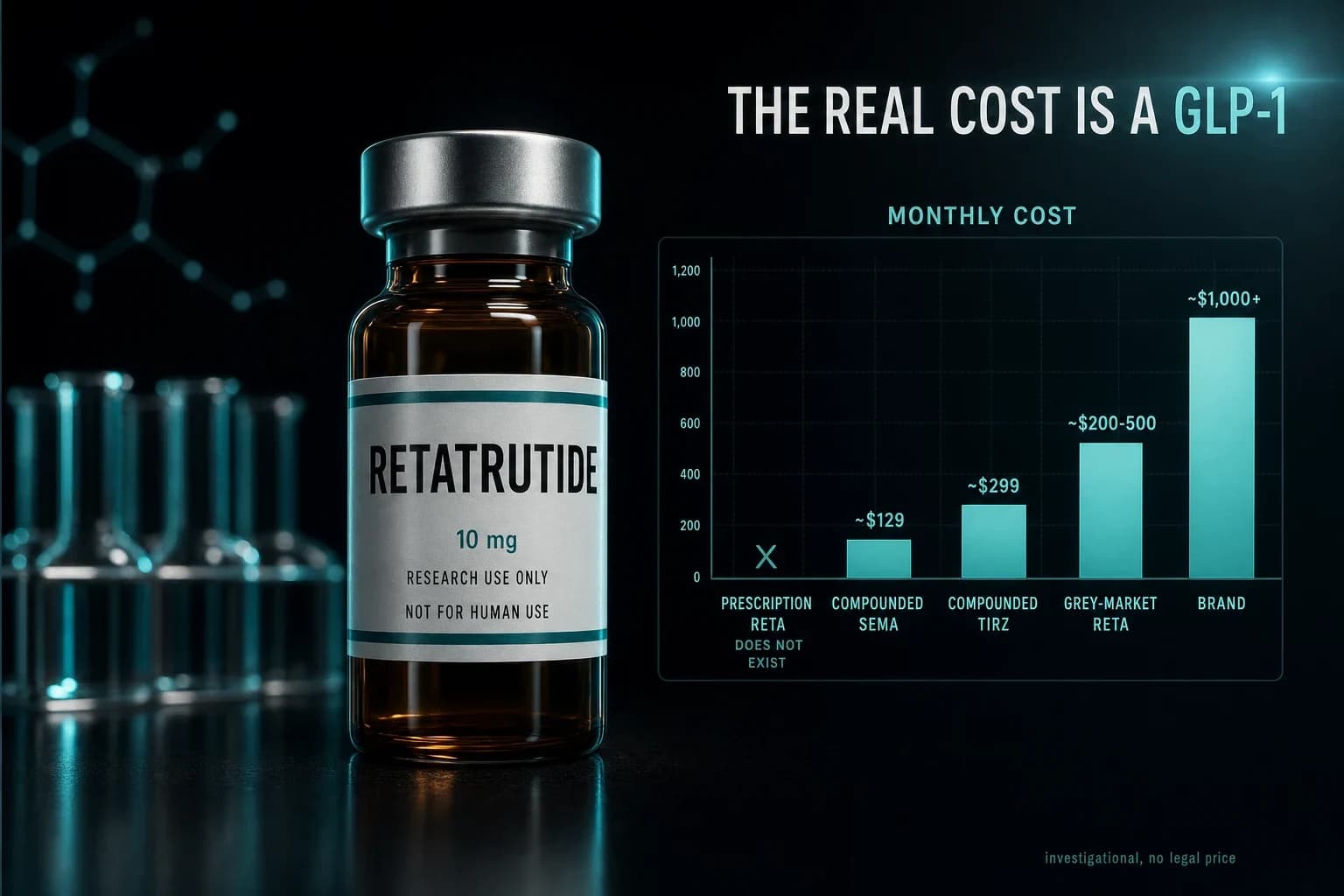
- The GLP-3 people mean is retatrutide (LY3437943), a triple agonist.
- Retatrutide hits three receptors: GLP-1, GIP, and glucagon.
- Phase 2 showed 24.2% body-weight loss at 48 weeks (Jastreboff 2023).
- Retatrutide is investigational. It is not FDA approved or prescribable yet.
There is no such thing as GLP-3. No hormone by that name exists, no receptor, no approved drug. If you typed "GLP-3" into a search bar expecting the next step up from Ozempic and Mounjaro, the instinct was right even though the term is wrong. What you are actually looking for is retatrutide, an investigational compound from Eli Lilly that the internet nicknamed "GLP-3" because it hits three receptors instead of one or two. This guide clears up the confusion and points you to the real compound.
The naming logic is easy to reverse-engineer. Semaglutide is a single agonist (GLP-1). Tirzepatide is a dual agonist (GLP-1 plus GIP). Retatrutide is a triple agonist, so people counted the receptors, saw "three," and coined "GLP-3." It is a misnomer, but a useful one, because it tells you exactly what makes this drug different: it recruits one more hormone pathway than anything currently on pharmacy shelves.
What people actually mean when they search "GLP-3"
Almost every "GLP-3" search traces back to one molecule. Its development code is LY3437943 and its generic name is retatrutide. In trials it has produced the largest weight-loss numbers ever reported for a drug of this type, which is why forum posts, TikToks, and news write-ups reach for a shorthand. "The triple" is accurate. "GLP-3" is catchier and wrong.
The confusion matters because it sends people looking for a class of drug that does not exist, and away from the actual research and the actual supervised routes available today. If you want the deep profile, the full mechanism and trial history lives on the retatrutide compound page and in our retatrutide triple-agonist explainer.
Bottom line: "GLP-3" is a nickname the internet invented for retatrutide, a triple agonist. There is no GLP-3 receptor and no drug officially called GLP-3.
The incretin receptor family, briefly
To understand why "GLP-3" is a misnomer, you need the actual cast of characters. These drugs work by mimicking gut and pancreatic hormones that regulate blood sugar, appetite, and energy use. The relevant three are GLP-1, GIP, and glucagon. There is no fourth incretin called GLP-3 waiting in line.
GLP-1 (glucagon-like peptide-1) is the one everyone knows. It slows stomach emptying, boosts insulin after meals, and dampens appetite in the brain. GIP (glucose-dependent insulinotropic polypeptide) is the second incretin, and it appears to improve how the body handles fat and amplifies GLP-1's effect on insulin. Glucagon is the odd one out: on its own it raises blood sugar, but it also increases energy expenditure and encourages the liver to burn fat. Pair it carefully with the other two and you get more calorie burn without losing glucose control.
Here is the family laid out.
| Receptor | Hormone it mimics | What activating it does | Drugs that hit it |
|---|---|---|---|
| GLP-1 | Glucagon-like peptide-1 | Slows gastric emptying, raises meal-time insulin, cuts appetite | Semaglutide, tirzepatide, retatrutide |
| GIP | Glucose-dependent insulinotropic polypeptide | Improves fat handling, amplifies the insulin response | Tirzepatide, retatrutide |
| Glucagon | Glucagon | Raises energy expenditure, drives hepatic fat burning | Retatrutide |
Read the table top to bottom and the progression is obvious. Semaglutide pulls one lever. Tirzepatide pulls two. Retatrutide pulls all three. That third lever, glucagon, is the piece no approved drug currently engages, and it is the reason retatrutide gets its own nickname.
The real name: retatrutide (LY3437943)
Retatrutide is a once-weekly injectable peptide engineered to activate the GLP-1, GIP, and glucagon receptors at once. Because glucagon normally raises blood sugar, the molecular design tunes the balance so the glucose-lowering effects of GLP-1 and GIP stay dominant while glucagon contributes its metabolic-rate and fat-burning benefits. That balancing act is the entire engineering challenge, and it is what separates a useful triple agonist from a dangerous one.
The compound belongs to the same broad family as tirzepatide and semaglutide, but adds the glucagon arm on top. If you want to see how the three stack up head to head, the retatrutide vs tirzepatide vs semaglutide comparison breaks down the trial numbers side by side.
Why the triple mechanism drives bigger weight loss
More receptors is not automatically better, but in this case the trial data backs up the theory. The standout is the Phase 2 obesity trial. Jastreboff et al. (2023) reported that adults on the highest 12 mg dose of retatrutide lost 24.2% of their body weight at 48 weeks, versus roughly 2% on placebo. Nearly a quarter of body weight, and the curve had not clearly flattened, which suggests the ceiling may be even higher over a longer trial.
Put that number next to the current leaders. In the SURMOUNT-1 trial of the dual GIP/GLP-1 agonist tirzepatide, Jastreboff et al. (2022) reported about 21% weight loss at the 15 mg dose over 72 weeks. For the single GLP-1 agonist semaglutide, the STEP 1 trial from Wilding et al. (2021) found a 14.9% mean reduction at 68 weeks. Retatrutide beat both, and did it in less time.
The pattern lines up with the mechanism: one receptor, roughly 15%; two receptors, roughly 21%; three receptors, roughly 24% and climbing. The glucagon arm is the leading explanation for the extra ground gained, because raising energy expenditure adds a lever that pure appetite suppression does not have.
The metabolic benefits are not limited to the scale. In people with type 2 diabetes, Rosenstock et al. (2023) found that retatrutide produced clinically meaningful improvements in glycemic control alongside robust weight loss, with a safety profile broadly comparable to existing GLP-1 drugs. Same triple mechanism, measured against blood sugar instead of body weight, same direction of effect.
The catch: retatrutide is investigational
Here is the part that gets lost in the hype. Retatrutide is not approved. As of now it has completed Phase 2 and is working through large Phase 3 trials, but no regulator has cleared it for sale, and no doctor can write you a legitimate prescription for it. You cannot get "GLP-3" at a pharmacy, because the drug it refers to is still in testing.
That also means the safety picture is incomplete. Phase 2 flagged the expected gastrointestinal effects common to this whole drug class (nausea, diarrhea, and similar), plus dose-dependent increases in heart rate that Phase 3 is designed to characterize further. We cover the current adverse-event data in the retatrutide side effects guide, and researched dosing schedules from the trials are collected in the retatrutide dosage chart. Treat all of it as investigational, because that is what it is.
Warning: Retatrutide is an investigational compound, not an approved medicine. There are no established human treatment doses outside clinical trials, no long-term safety record, and no legal prescription route. Anyone selling "GLP-3" as a finished drug is not offering something a regulator has cleared.
If you want a supervised GLP-1 route today
So the drug you searched for is real, promising, and not yet available. That leaves a practical question: what can you actually do now? The honest answer is that the approved GLP-1 and dual-agonist medications already deliver serious, clinically proven weight loss, and unlike retatrutide you can access them under medical supervision.
The right move is a prescribed telehealth route rather than a gray-market vial. A licensed provider like Yucca Health can evaluate whether a supervised GLP-1 program fits you, handle the prescription, and monitor you along the way. That is the difference between a drug with a doctor attached and a powder with a nickname attached. For a breakdown of the lowest-cost legitimate options, see our guide to the cheapest GLP-1 programs, and for the popular dual-agonist path specifically, compounded tirzepatide online covers what supervised access looks like and what it costs.
When retatrutide does clear Phase 3 and reach approval, it will almost certainly arrive through that same supervised, prescribed channel. Following the real compound now means you will recognize it when it lands, instead of chasing a name that was never on the label.
The short version
GLP-3 is not a hormone, not a receptor, and not a drug. It is a nickname for retatrutide (LY3437943), an investigational triple agonist that activates the GLP-1, GIP, and glucagon receptors. Its Phase 2 weight-loss numbers are the highest reported for the class, the glucagon arm is the likely reason, and it is not approved or prescribable yet. If you want results under medical supervision today, an approved GLP-1 program through a licensed telehealth provider is the real, available version of what "GLP-3" was pointing you toward.
This article is for research and educational purposes only. It is not medical advice. Retatrutide (LY3437943) is an investigational compound that has not been approved by the FDA or any regulator for the treatment of obesity, type 2 diabetes, or any other condition, and it is not available by prescription outside of clinical trials. Nothing here is a recommendation to use, purchase, or administer any substance. Consult a qualified healthcare professional before making any health decision.