At a glance
- TRIUMPH-4 (Phase 3, 68 wks): −28.7% at 12 mg vs −2.1% placebo (Lilly, Dec 11, 2025)
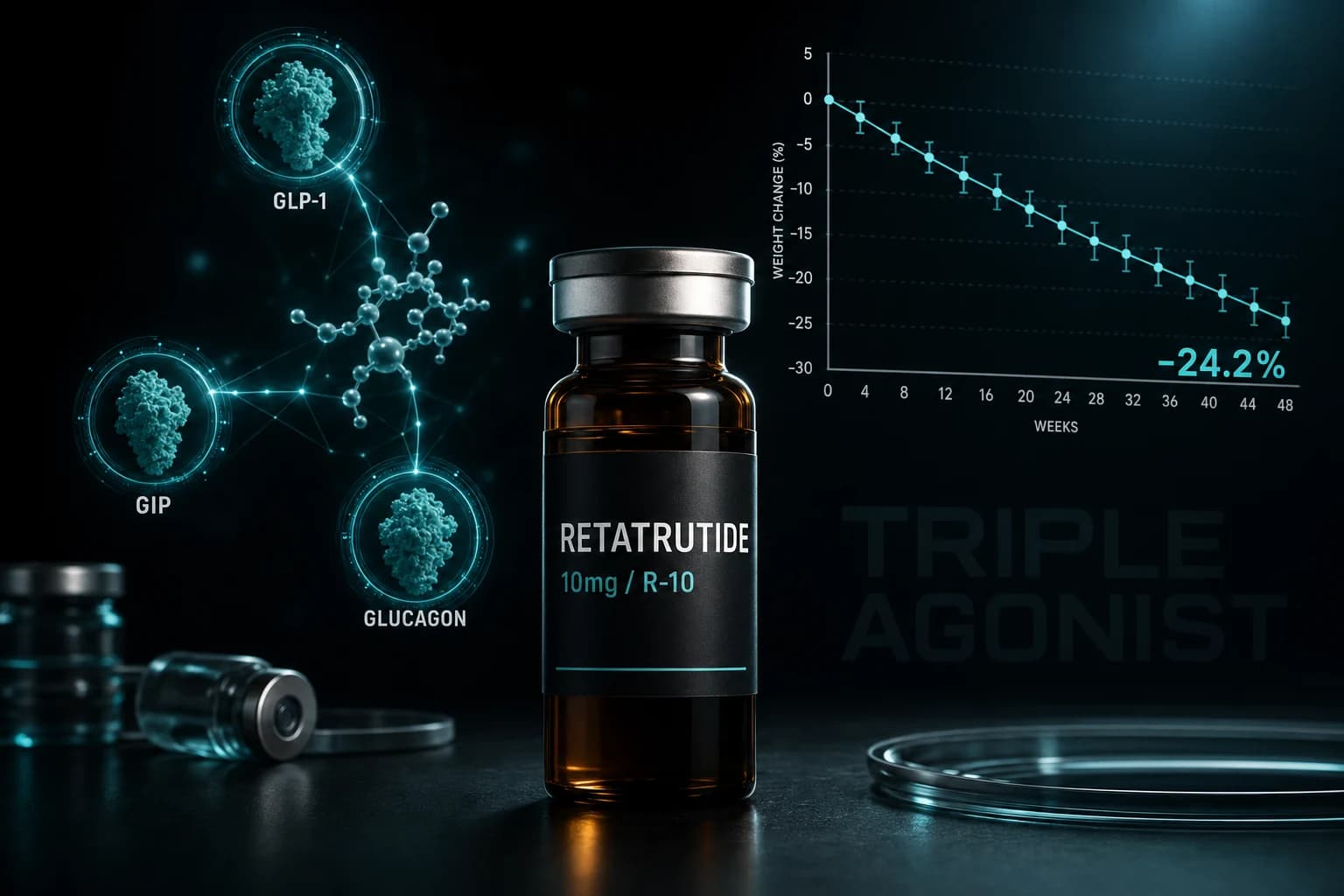
- Phase 2 NEJM 2023 baseline: −24.2% at 48 weeks, n=338 (Jastreboff et al)
- Triple agonist: GLP-1 (appetite) + GIP (metabolism) + glucagon (energy burn)
- TRIUMPH-4 enrolled obesity + knee osteoarthritis (T2D excluded)
- New safety signal: dysesthesia 20.9% at 12 mg vs 0.7% placebo
The Phase 3 number
On December 11, 2025, Eli Lilly reported topline results from TRIUMPH-4, the first successful Phase 3 trial of Retatrutide. At the 12 mg weekly dose, participants lost 28.7% of body weight at 68 weeks versus −2.1% on placebo. The 9 mg arm reached −26.4%. Trial size: n=445.
For context across compound classes:
- Retatrutide 12 mg, TRIUMPH-4 (68 wks): −28.7%
- Retatrutide 12 mg, Phase 2 (48 wks, Jastreboff et al., NEJM 2023): −24.2%
- Tirzepatide 15 mg (SURMOUNT-1, 72 wks): −20.9%
- Semaglutide 2.4 mg (STEP-1, 68 wks): −14.9%
- Lifestyle intervention alone: −2.4%
The Phase 3 number is the largest controlled-trial weight loss reported for a pharmaceutical compound to date. Two important caveats matter for how to read it:
- TRIUMPH-4 enrolled adults with obesity AND knee osteoarthritis (BMI ≥27, 84% had BMI ≥35). Type 2 diabetes was excluded. The co-primary endpoints were percent body weight change AND change in WOMAC pain at 68 weeks. So the headline 28.7% is from an obesity-plus-OA population, not generalized obesity.
- Press release only. As of April 2026, TRIUMPH-4 has not been published in a peer-reviewed journal. Detailed results are expected at a future medical meeting.
How it works: three receptors, not one or two
Most GLP-1 research compounds activate one receptor (Semaglutide) or two (Tirzepatide). Retatrutide activates three simultaneously:
1. GLP-1 receptor
The standard incretin pathway. Slows gastric emptying, reduces appetite, increases insulin secretion in response to meals. This is the "stop eating" signal.
2. GIP receptor
Another incretin, but primarily insulin-amplifying. Boosts the insulin response to GLP-1 activation and appears to modulate energy expenditure. This is the "process food better" signal.
3. Glucagon receptor
This is the unique addition. Glucagon receptor activation increases energy expenditure: the body burns more calories at rest. It's the "burn more" signal that Semaglutide and Tirzepatide don't have.
The combination produces both reduced caloric intake (GLP-1/GIP) and increased energy burn (glucagon). This dual mechanism is why the efficacy is so dramatically higher.
The glucagon concern
Glucagon is traditionally associated with raising blood sugar (it's the counter-regulatory hormone to insulin). You might reasonably ask: doesn't glucagon agonism work against the insulin-sensitizing effects of GLP-1 and GIP?
The answer from Phase 2 data: no, because GLP-1 and GIP dominate the glucose regulation while glucagon handles energy expenditure. HbA1c improvements in Retatrutide trials were comparable to Tirzepatide. The insulin-sensitizing pathways win.
Essentially, the compound is engineered such that each receptor contributes its beneficial effects without the downsides becoming dominant.
Current status: TRIUMPH-4 read out, more pending
As of April 2026, Retatrutide has its first successful Phase 3 result and a multi-trial program still running. Lilly stated additional Phase 3 readouts are expected through 2026.
- TRIUMPH-4 (read out Dec 11, 2025): Obesity + knee osteoarthritis, 68 weeks. Result above. Co-primary on body weight AND WOMAC pain. Not yet peer-reviewed.
- TRIUMPH-1: Obesity without diabetes, 72 weeks. Pending.
- TRIUMPH-2: Obesity with type 2 diabetes. Pending.
- TRIUMPH-3: Cardiovascular outcomes in obesity with CVD. Pending.
- TRIUMPH-Outcomes: MACE endpoint trial. Pending.
Lilly has not publicly committed to a specific FDA submission timeline as of the December 2025 release. Any "approval in 2026 or 2027" language elsewhere on the internet is speculation, not company guidance.
Dosing protocol
Phase 2 trials titrated Retatrutide over 12-20 weeks to minimize nausea:
- Weeks 1-4: 2 mg weekly
- Weeks 5-8: 4 mg weekly
- Weeks 9-12: 8 mg weekly
- Weeks 13+: 12 mg weekly (maximum)
Maximum efficacy was seen at 12 mg, with diminishing additional benefit at higher doses.
Half-life is approximately 6 days, consistent with once-weekly dosing.
Side effect profile
The Phase 3 TRIUMPH-4 dataset is now the most complete safety read for Retatrutide. Rates at 12 mg vs placebo:
- Nausea: 43.2% vs 10.7%
- Diarrhea: 33.1% vs 13.4%
- Constipation: 25.0% vs 8.7%
- Vomiting: 20.9% vs 0%
- Dysesthesia (abnormal sensation): 20.9% vs 0.7% (8.8% at 9 mg)
GI side effects are consistent with the GLP-1 class but at the high end. The dysesthesia signal is the new and notable finding that did not show up at this rate in earlier trials. It warrants attention as more Phase 3 data accumulates.
Treatment discontinuation due to adverse events: 18.2% at 12 mg, 12.2% at 9 mg, 4.0% on placebo. The drop-off rate at the top dose is meaningful and a data point for any researcher considering dose targeting.
When Retatrutide makes sense
For research in:
- Severe obesity (BMI > 40)
- Metabolic dysfunction where maximum efficacy matters
- Comparative studies vs first-generation GLP-1s
- MASLD and hepatic fat reduction research
Less useful for:
- Mild metabolic intervention (Semaglutide is sufficient)
- Cardiovascular outcomes research (Semaglutide has existing data)
- Cost-sensitive protocols (Retatrutide is premium-priced)
Research access
Retatrutide is available from our verified partner at research-grade purity with 50% off using code ENHANCED.


