At a glance
- Semaglutide 1.0 mg weekly reduced drinks per drinking day and weekly craving in a 48-person AUD RCT (Hendershot et al. 2025)
- Effect sizes on lab-task alcohol intake were medium to large (β around -0.46 to -0.48)
- A real-world cohort of 83,825 patients linked semaglutide to a 50-56% lower AUD incidence (Wang et al. 2024)
- Preclinical work shows GLP-1 agonists blunt alcohol-induced dopamine release in the nucleus accumbens
- Tirzepatide and retatrutide replicate the effect in rat interoception models (Windram et al. 2025)
- No GLP-1 agonist is approved for AUD; current data is hypothesis-generating, not clinical
Forty-eight people is a small trial. The signal is not small.
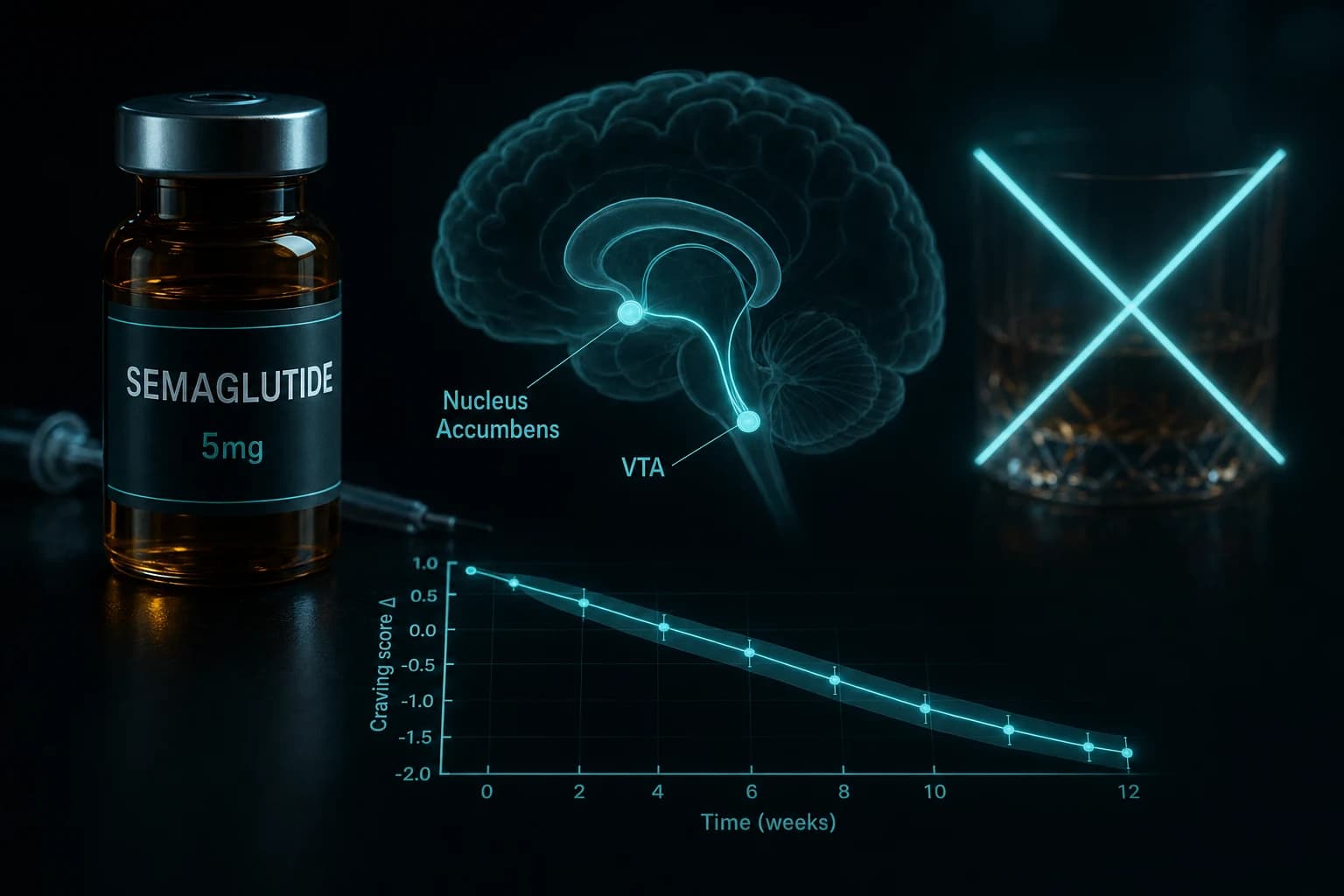
In February 2025, JAMA Psychiatry published the first randomized, double-blind, placebo-controlled trial of a GLP-1 receptor agonist in adults with alcohol use disorder. Forty-eight non-treatment-seeking participants, nine weeks of outpatient semaglutide titrated to 1.0 mg once weekly, and a prespecified lab alcohol self-administration task. The semaglutide group drank less during the task, with medium-to-large effect sizes for grams consumed (β, -0.48; 95% CI, -0.85 to -0.11) and peak breath alcohol concentration (β, -0.46; 95% CI, -0.87 to -0.06), and they reported less weekly craving (β, -0.39; 95% CI, -0.73 to -0.06) (Hendershot et al., JAMA Psychiatry 2025).
This is a phase 2 signal, not a phase 3 outcome. What makes it interesting is that it lands on top of three years of preclinical work, retrospective cohort data on tens of thousands of patients, and Reddit reports from people on semaglutide for weight loss who quietly stopped drinking. The research question has shifted from whether GLP-1 agonism touches the alcohol circuit to how large the effect is at real doses, whether it generalizes to tirzepatide and retatrutide, and what safe off-label research looks like for non-obese users.
If you are already running a GLP-1 protocol for body composition, you are likely also running an informal AUD trial on yourself. It is worth knowing what the data does and does not say.
Where the human evidence actually stands
Most of the media story is retrospective. Two signals matter most: the Hendershot RCT, and the Klausen exenatide trial that set the template three years earlier. A large real-world cohort study from Case Western sits next to them and gives the class-level effect a scale read.
| Study | Design | Compound | N | Key finding |
|---|---|---|---|---|
| Klausen et al., JCI Insight 2022 | 26-week RCT, placebo-controlled, with CBT | Exenatide 2 mg weekly | 127 AUD patients | No effect on heavy drinking days overall. BMI >30 subgroup saw significant reductions. fMRI showed blunted alcohol cue reactivity in ventral striatum. |
| Quddos et al., Scientific Reports 2023 | Reddit NLP + remote self-report survey | Semaglutide or tirzepatide | 153 (survey); 68,250 posts (NLP) | Self-reported AUDIT score, binge drinking odds, and drinks per episode all dropped on GLP-1 therapy vs controls. 71.7% of alcohol-related Reddit posts described reduced craving or drinking. |
| Wang et al., Nature Communications 2024 | Retrospective EHR cohort, propensity-matched | Semaglutide vs other anti-obesity drugs | 83,825 obese patients (plus 598,803 T2D replication) | 50-56% lower 12-month risk of incident and recurrent AUD. Effect held across age, sex, race, with and without diabetes. |
| Hendershot et al., JAMA Psychiatry 2025 | Phase 2 RCT, 9 weeks, double-blind | Semaglutide 0.25→0.5→1.0 mg weekly | 48 adults with AUD | Lab-task alcohol intake fell with medium-to-large effect sizes. Drinks per drinking day and weekly craving also fell. No effect on days drinking per se. |
Each of these tells part of the picture. The Klausen trial showed a null on the primary outcome but a clean mechanistic signal on fMRI and a real effect in the obese subgroup, which is the group where GLP-1 agonists are strongest. The Quddos analysis showed that real users were already self-reporting the phenomenon well before the formal trials read out. The Wang cohort put a number on the effect at population scale, though observational data cannot isolate drug effect from selection. The Hendershot trial is the first clean placebo-controlled RCT with a modern GLP-1 agonist.
Bottom line: The class-level signal is consistent. The best controlled human data is still a 48-person phase 2. Treat everything below as hypothesis-generating, not clinical practice.
Reading the Hendershot RCT carefully
The trial enrolled 48 adults with AUD but not seeking treatment, which is an unusual population. Participants averaged 39.9 years old and 71% were female. The titration matched the standard Ozempic weight-loss schedule: 0.25 mg for four weeks, 0.5 mg for four weeks, then 1.0 mg for one week. That last week ended with the lab self-administration task.
Two things about the primary outcome design are important. First, the "drinks per calendar day" and "drinking days" measures did not move, which is a fair knock on headline framing that implies semaglutide makes people stop drinking. What moved was the amount consumed when a person did drink, the lab-task intake, and the craving score. Second, this was a nine-week trial with a brief exposure to the full dose. Semaglutide pharmacokinetics reach steady state around five weeks at any given dose, so the 1.0 mg signal was captured in a single dosing window.
Effect sizes of β around -0.4 to -0.5 translate to a medium behavioral effect. Naltrexone, the closest FDA-approved AUD comparator, typically shows effect sizes of 0.1 to 0.2 for heavy drinking reduction in trial settings. That is not a direct head-to-head, and the AUD populations differ, but it frames why researchers are paying attention.
What the trial cannot tell you: whether the effect holds past nine weeks, whether it persists after semaglutide is stopped, and whether it translates to severe AUD with daily drinking patterns. The Windram animal work (Windram et al., Psychopharmacology 2025) hints at the last question. Repeated semaglutide maintained efficacy across a 15-day treatment period in rats, and alcohol discrimination returned to baseline three days after the drug was stopped. That is a plausible clinical picture, but it is a rat model.
The mechanism: mesolimbic dopamine and gastric emptying both contribute
Early coverage framed the alcohol effect as a side effect of slowed gastric emptying. That is a real phenomenon. GLP-1 agonists delay stomach emptying by roughly 30 to 70%, and alcohol is mostly absorbed in the small intestine. Slower gastric transit flattens the subjective reward curve. But the central mechanism is now well supported, and it is not reducible to gut kinetics.
Foundational mouse work showed that exendin-4, at a dose that did not affect locomotion on its own, blocked alcohol-induced dopamine release in the nucleus accumbens (Egecioglu et al., Psychoneuroendocrinology 2013). That accumbens dopamine surge is the core reward signal that trains repeated consumption. Subsequent work used direct injection of GLP-1 agonists into the VTA, nucleus accumbens, and lateral septum to confirm the central site of action. Optogenetic and chemogenetic studies in GLP-1 receptor-expressing neurons reinforced the point. The receptor is widely expressed in mesolimbic reward structures, and activation reduces drug-seeking.
The Klausen fMRI data is the cleanest human mechanism finding to date. Even though exenatide did not beat placebo on heavy drinking days, the exenatide arm showed reduced BOLD activation in the ventral and dorsal striatum in response to alcohol cue images. That is the same circuit alcohol taps into during craving, and the same circuit the preclinical work implicated.
Tip: If you are reading coverage that attributes GLP-1 alcohol effects entirely to nausea or gastric emptying, the mechanism story is five years out of date.
Does the effect generalize to tirzepatide and retatrutide?
The Quddos survey pooled semaglutide and tirzepatide users and found similar reductions in drinks per episode and AUDIT score. That is self-report in a non-randomized sample, so it cannot cleanly separate the two compounds. The animal side is further along.
Windram et al., Psychopharmacology 2025 trained male and female rats on alcohol drug discrimination, then tested acute doses of semaglutide, tirzepatide, and retatrutide. All three attenuated alcohol's interoceptive effects. This is the first published head-to-head of a GLP-1 mono-agonist, a GLP-1/GIP dual, and a GLP-1/GIP/glucagon triple on alcohol's subjective signal in a single experimental design. The effect was similar across compounds at equi-efficacious metabolic doses.
That matters because clinical populations are increasingly on tirzepatide (Mounjaro, Zepbound) or anticipating retatrutide approval. If the alcohol effect scales with GLP-1R occupancy rather than requiring broader receptor coverage, then tirzepatide and retatrutide should behave similarly in humans. If it requires something GIP or glucagon adds on top, the rat study would have shown a clear gradient. It did not. For a full primer on the triple agonist, see our retatrutide explainer and the triple GLP-1 comparison.
The 2024 real-world Wang cohort is strong but limited to semaglutide. A comparable Nature Communications analysis on tirzepatide has not yet been published. Most of the 2024 to 2025 coverage extrapolating a class effect is doing so from the Quddos self-report data plus the preclinical evidence. That is a reasonable scientific read, but it is not equivalent to a phase 2 trial.
What the Wang cohort actually found, and what it did not
The Wang cohort used TriNetX electronic health records and propensity-matched 83,825 obese patients started on semaglutide against obese patients started on other anti-obesity medications. The semaglutide group had a 50 to 56% lower 12-month risk of both incident AUD and AUD recurrence. A replication in 598,803 patients with T2D showed the same direction and magnitude.
That is a striking effect size, but retrospective EHR data is vulnerable to confounding by indication. Patients started on semaglutide versus other weight drugs are not identical on unmeasured variables like socioeconomic status, motivation, or baseline alcohol use. Propensity matching narrows the gap but cannot close it. The same study design applied to bupropion or naltrexone would also show lower AUD incidence, because the prescriber selected for a patient already engaged in behavior change.
The right read: the Wang cohort confirms there is a real population-level signal and rules out the possibility that the lab effect is a curiosity. It does not establish a causal effect size to within 50%.
What this does NOT mean
- It does not mean GLP-1 agonists are an AUD treatment. None is approved for that use. The Hendershot data is phase 2.
- It does not mean semaglutide is safe for someone with severe AUD who is actively drinking heavily. No trial has enrolled that population. Alcohol combined with GLP-1-induced gastroparesis raises aspiration risk, and semaglutide labels already flag a boxed concern around anesthesia and gastric retention.
- It does not mean "Ozempic cures alcoholism." The 48-person Hendershot RCT moved amount per drinking occasion and craving, not drinking days. The craving signal is the more interesting mechanistic finding, not a clinical endpoint.
- It does not mean a low semaglutide dose used for AUD is safer than the weight-loss dose. Hendershot titrated to 1.0 mg, the standard Ozempic dose. No dose-finding trial has been done for alcohol cravings specifically. Lower doses might or might not preserve the effect.
- It does not mean GLP-1 agonists work for other substance use disorders at the same magnitude. Preclinical data in cocaine, nicotine, and opioids exists, but human trials are smaller, more mixed, and mostly negative for opioids.
Warning: If you are researching GLP-1 agonists while actively drinking heavily, the gastric retention risk with the 1.0 mg and 2.4 mg weekly doses is non-trivial. The same delayed emptying that may blunt reward signals can trap alcohol in the stomach longer than expected.
How this intersects with a weight-loss research protocol
Most readers here are already running a GLP-1 protocol for body composition, not for alcohol reduction. The practical question is what happens when those goals stack. A few data points worth holding together:
- The Quddos self-report data and the Wang cohort both came from obese or overweight populations. The cleanest real-world effect of semaglutide on alcohol has been described in the weight-loss population, not in lean researchers at low doses. If you are running 0.25 mg weekly for aesthetic body composition, you may or may not hit the threshold where the central reward-pathway effect becomes detectable.
- Alcohol calories stack with your deficit. A sizable part of the weight-loss benefit attributed to GLP-1 therapy in the O'Farrell DOM cohort was mathematically consistent with reduced alcohol intake (alcohol drops from roughly 11.8 to 4.3 units per week would account for a meaningful caloric delta). The muscle-loss risk we covered in the GLP-1 muscle loss research read also scales with steeper deficits, so an unexpected alcohol drop on GLP-1 therapy can widen the caloric gap past the point where lean mass holds up.
- If your research protocol includes both a GLP-1 agonist and a cognitive or recovery peptide stack, the alcohol effect is worth noting in your self-report log. The effect shows up in craving scores before it shows up in drinking days, which means you can monitor it subjectively earlier than you would see it in weekly intake.
- The interaction with sleep and next-day training is underexamined. The same mechanism that reduces the perceived reward of the first drink may also reduce the compulsion to continue drinking, which in real-world use looks a lot like "I had two and didn't feel like a third." For people running performance-oriented stacks like the FIT Stack or Wolverine recovery protocol, that behavioral tail can move training adherence more than the scale can.
For the research-purposes context, high-quality injectable semaglutide is available from Ascension Peptides with 50% off using code ENHANCED. Their platform is geared toward the researcher population this article addresses.
Practical read for researchers following this field
- The best controlled human evidence is the 48-person Hendershot RCT. Treat it as a phase 2 signal. Phase 3 semaglutide AUD trials are in planning stages. Tirzepatide AUD trials are further behind.
- The mechanism is centrally mediated through the GLP-1 receptor's expression in the mesolimbic reward circuit. It is not simply a gastric emptying artifact, and it is not reducible to nausea.
- The 50 to 56% cohort effect from Wang et al. 2024 is real but confounded. The true causal effect is almost certainly smaller than the observational signal suggests.
- Expect the 2026 to 2027 literature to include: phase 3 semaglutide-AUD RCTs, tirzepatide-AUD phase 2 data, imaging studies linking dose to striatal activity, and probably a retatrutide signal given the animal data.
- If you track the GLP-1 class, you already have a hypothesis for why tirzepatide and retatrutide should behave similarly on alcohol. The rat head-to-head (Windram et al. 2025) supports that view.
Bottom line
The 2025 Hendershot RCT is the first clean randomized test of a GLP-1 agonist for alcohol use disorder, and it showed medium-to-large effects on lab-task alcohol intake and weekly craving at the standard 1.0 mg Ozempic dose. That result lines up with a 127-patient exenatide trial from 2022, a retrospective cohort of 83,825 semaglutide patients, multiple rat and mouse models, and Reddit self-report data. The mechanism runs through mesolimbic dopamine, not only through gastric emptying. None of this makes GLP-1 agonists approved for addiction research, and none of it resolves whether the effect persists beyond a few months. It does mean the question has moved from "is there a signal" to "how big, how durable, and in whom."
Related research on this site
- Tirzepatide vs Semaglutide: The 2026 Head-to-Head
- Retatrutide vs Tirzepatide vs Semaglutide: 2026 GLP-1 Comparison
- GLP-1 Muscle Loss: What the Research Shows in 2026
- Retatrutide Explained: Why It's the Most Effective Weight Peptide Yet
- 12-Week Retatrutide Titration Protocol
- Semaglutide research page
- Tirzepatide research page
- Retatrutide research page
- Reconstitution Calculator
This article is for educational and research purposes only. No GLP-1 receptor agonist is FDA-approved for alcohol use disorder. Semaglutide is FDA-approved for type 2 diabetes (Ozempic, Rybelsus) and chronic weight management (Wegovy). The data on alcohol-related outcomes reviewed here is hypothesis-generating and does not establish clinical efficacy or safety for AUD. Combining alcohol with high-dose GLP-1 agonist therapy carries gastric retention and aspiration risk. Consult a qualified healthcare professional before making any decisions about peptide research or AUD treatment.


