At a glance
- Retatrutide led every trial: 24.2% body-weight loss at 48 weeks (Jastreboff 2023).
- Tirzepatide hit 20.9% and semaglutide 14.9% in Phase 3 obesity trials.
- Only the GLP-1 class has large human weight-loss data. Most other peptides do not.
- Tesamorelin cuts visceral fat 15.2% but barely moves total body weight.
- AOD-9604 failed its Phase 2 trial. MOTS-c has zero human weight-loss data.
Retatrutide produced a 24.2% body-weight reduction at 48 weeks. That is roughly a quarter of a person's starting weight, from one weekly injection, in a placebo-controlled trial published in the New England Journal of Medicine. No peptide marketed as a "fat burner" on a research site comes within shouting distance of that number.
That gap is the whole story of this page. When people search for the best peptides for weight loss, they usually get a list that mixes genuine anti-obesity drugs with recycled growth-hormone fragments that failed their own clinical trials. We are going to separate them by evidence, not by which one sounds most exotic.
Here is the uncomfortable summary before the details: the peptides that actually strip fat in humans are almost all GLP-1 class incretin drugs. Everything else is either niche, indirect, or unproven. We will still cover the research-grade options, because researchers ask about them, but we are not going to pretend a mitochondrial peptide competes with tirzepatide.
How we ranked these peptides
Three questions decide the order:
- Is there a large, randomized, placebo-controlled human trial? Rodent data and open-label anecdotes do not count.
- How much total body weight did people actually lose, and over what timeline?
- Can you legally access it, and through which route?
Weight loss reported below is mean total body-weight reduction at the highest studied dose, versus placebo, from the registration or Phase 2 trial for each compound. Where a peptide only affects fat distribution rather than scale weight, we say so plainly.
The ranked list
| Peptide | Mechanism | Avg weight loss (top dose) | Evidence tier | Route |
|---|---|---|---|---|
| Retatrutide | GLP-1 / GIP / glucagon triple agonist | 24.2% at 48 wks | Phase 2, strong | Injectable, investigational |
| Tirzepatide | GLP-1 / GIP dual agonist | 20.9% at 72 wks | Phase 3, approved | Injectable, Rx |
| CagriSema | Amylin + GLP-1 combination | 20.4% at 68 wks | Phase 3 | Injectable, investigational |
| Semaglutide | GLP-1 receptor agonist | 14.9% at 68 wks | Phase 3, approved | Injectable, Rx |
| Cagrilintide | Long-acting amylin analog | 10.8% at 26 wks | Phase 2 | Injectable, investigational |
| Tesamorelin | GHRH analog | Visceral fat -15.2%, scale weight ~flat | Approved (HIV lipodystrophy) | Injectable |
| MOTS-c | Mitochondrial-derived peptide | No human weight-loss data | Preclinical / rodent | Injectable |
| AOD-9604 | Fragment of growth hormone (176-191) | No significant effect vs placebo | Failed Phase 2 | Injectable / oral |
The top four rows are drugs with real obesity trials. The bottom four are where most of the hype lives and most of the evidence does not.
Tier 1: the GLP-1 class, the only category that consistently works
Semaglutide, tirzepatide, and retatrutide are all peptides. That is not a technicality. They are engineered incretin analogs that happen to be the most effective weight-loss agents ever put through trials. If you want fat loss backed by data, this is the category, full stop.
Retatrutide: the current ceiling
Retatrutide hits three receptors at once: GLP-1, GIP, and glucagon. The glucagon arm is the interesting part, because it raises energy expenditure on top of the appetite suppression the other two provide.
In the Phase 2 trial, Jastreboff et al. (2023) reported that adults on the 12 mg dose lost 24.2% of body weight at 48 weeks, with the curve still trending down at the end. The primary endpoint at 24 weeks already showed a dose-dependent separation from placebo, and no plateau had appeared by week 48. That is the highest figure any obesity drug has posted in a controlled trial to date.
The catch: retatrutide is investigational. Phase 3 (TRIUMPH) is running, and there is no approved prescription product. Everything you read about it is trial data. The retatrutide research page covers the receptor pharmacology in more depth.
Tirzepatide: the best thing you can actually get prescribed
Tirzepatide is the dual GLP-1 / GIP agonist sold as Zepbound for weight loss and Mounjaro for diabetes. In SURMOUNT-1, Jastreboff et al. (2022) showed a 20.9% mean reduction at the 15 mg dose over 72 weeks, versus 3.1% on placebo. More than half of participants on the top dose lost at least a fifth of their body weight.
Unlike retatrutide, this one is FDA-approved and available today. That makes it the practical winner for most people: near-retatrutide efficacy, real regulatory oversight, and a prescribing pathway. See the tirzepatide compound page for dosing and titration specifics, or the guide to compounded tirzepatide online if you are weighing the telehealth route.
Semaglutide: the proven, widely available option
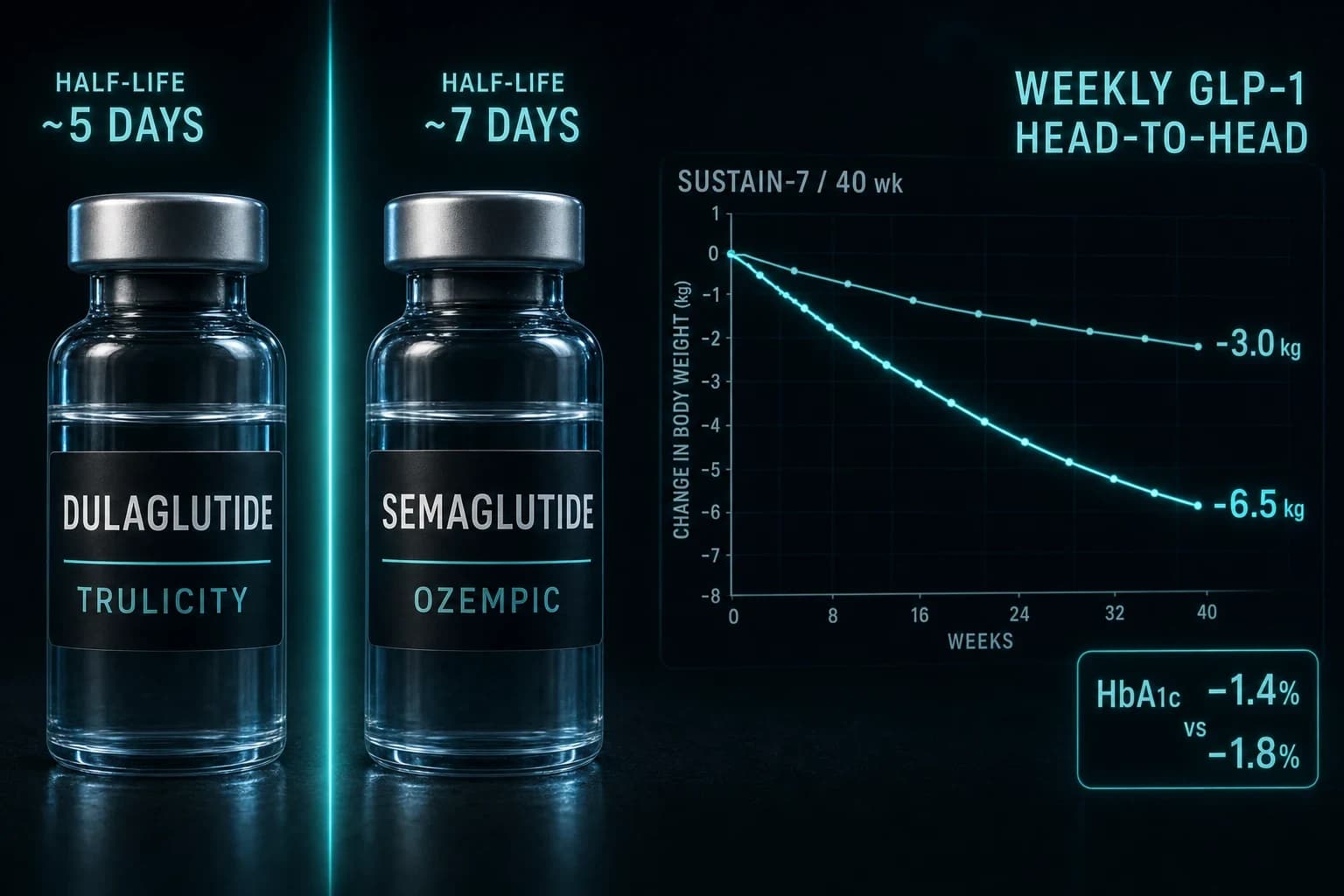
Semaglutide (Wegovy for obesity, Ozempic for diabetes) is the drug that made GLP-1 a household term. STEP 1, published by Wilding et al. (2021), found a 14.9% mean body-weight reduction at 68 weeks on 2.4 mg weekly, versus 2.4% on placebo.
That is a smaller number than tirzepatide's, and the head-to-head SURMOUNT-5 trial confirmed tirzepatide wins on magnitude. Semaglutide's advantages are availability, a longer real-world track record, and lower typical cost. For most people starting out, it is the sensible first move. The semaglutide page and the compounded semaglutide online guide walk through access.
CagriSema and cagrilintide: the amylin angle
Amylin is a different appetite hormone, and pairing a long-acting amylin analog with semaglutide is the idea behind CagriSema. In the REDEFINE 1 Phase 3 trial, Garvey et al. (2025) reported a 20.4% mean reduction, putting the combination in tirzepatide territory.
Cagrilintide on its own is weaker. Lau et al. (2021) found 10.8% at the 4.5 mg dose over 26 weeks in the Phase 2 dose-finding study, which is respectable but below the GLP-1 leaders. The value of amylin looks like it comes from combining it with a GLP-1, not from running it solo. The cagrilintide research page has the mechanism detail.
Bottom line: If the goal is maximum fat loss with real evidence behind it, the ranking is retatrutide (investigational) > tirzepatide (approved, get this) > CagriSema (investigational) > semaglutide (approved, widely available). Everything below this line is a meaningful step down.
Tier 2: a real drug aimed at the wrong target
Tesamorelin
Tesamorelin is a stabilized GHRH analog that raises your own growth-hormone pulses. It is FDA-approved, but for a specific job: reducing visceral fat in HIV-associated lipodystrophy.
The data are legitimate. Falutz et al. (2007) reported a 15.2% reduction in visceral adipose tissue versus a 5% increase on placebo over 26 weeks. That is a real effect on the dangerous fat around your organs.
Here is why it is not on the fat-loss podium: it barely moves the scale. Tesamorelin redistributes fat and trims visceral stores without producing the large total body-weight loss the GLP-1 drugs deliver. If your specific concern is stubborn visceral fat and metabolic markers, it earns a look. If you want to drop 40 pounds, it is the wrong tool. The tesamorelin page covers where it fits.
Tier 3: the peptides that mostly do not work for fat loss
This is where a lot of "best weight-loss peptide" lists lose the plot. Two names come up constantly and neither has earned it.
AOD-9604
AOD-9604 is a fragment of growth hormone (residues 176-191), marketed for years on the theory that it triggers fat breakdown without the blood-sugar side effects of full growth hormone. The theory sounded good. The trial did not cooperate.
Metabolic Pharmaceuticals ran a Phase 2b study in roughly 300 obese adults. The compound failed to produce clinically meaningful weight loss beyond placebo, and development as an obesity drug was discontinued. That result is not indexed in PubMed as a full publication, which itself tells you something about how the program ended. Rodent lipolysis data exist, but the human obesity trial is the one that counts, and it came up empty. Treat any site selling AOD-9604 as a "fat loss peptide" as selling you the hypothesis, not the outcome.
MOTS-c
MOTS-c is a mitochondrial-derived peptide that behaves like an exercise mimetic. The science is genuinely interesting: Reynolds et al. (2021) showed it is exercise-induced in human muscle and that injecting it improved metabolism and running capacity in aged mice.
Notice what that sentence does not contain: a human weight-loss trial. There isn't one. MOTS-c may improve metabolic flexibility and insulin sensitivity in models, but nobody has demonstrated meaningful fat loss from it in people. It is a promising research target, not a weight-loss protocol. The MOTS-c page keeps that distinction clear. The same caution applies to 5-Amino-1MQ and most "GH secretagogue for fat loss" pitches: indirect mechanism, no obesity trial.
Warning: There is a hard line between a prescribed medicine and a research chemical. Approved GLP-1 drugs are prescription medications that come with a clinician, a dose titration, and monitoring. Research-grade peptides sold in vials are labeled for laboratory use only, are not prescribed, and are not quality-controlled as medicines. Do not confuse the two, and do not treat a research vial as if a doctor signed off on it.
Two legitimate ways to access GLP-1s
Once you have decided the GLP-1 class is where the results are, there are two honest paths. They serve different people.
If you want medical supervision (most people should): a telehealth program is the cleanest route to a prescribed, compounded GLP-1. Yucca Health connects you with US-licensed clinicians who review your history, confirm eligibility, and, if appropriate, have the prescription filled by a compounding pharmacy and shipped to your door. That means real titration guidance and someone accountable for your care, which matters with a drug you inject weekly for months. Programs like this start well below brand-name pricing and skip the in-person visit.
If you are a researcher sourcing reference material: research-grade semaglutide and tirzepatide vials are available from Ascension Peptides with 50% off using code ENHANCED, shipped with per-batch certificates of analysis. This is laboratory-use-only material, not a prescription, and it is on you to verify purity and handle reconstitution correctly. The reconstitution calculator handles the unit math so a 5 mg vial actually gives you the dose you intend.
These are not interchangeable. One is a supervised medical program; the other is lab supply. Pick based on which describes you.
What it actually costs
Price is usually the real deciding factor, so be clear-eyed about it. Brand-name Wegovy and Zepbound carry list prices north of $1,000 a month before insurance. Compounded telehealth is dramatically cheaper and is the most affordable legitimate medical route for people paying cash. Research-grade vials are cheapest per milligram but come with none of the medical guardrails.
We broke the full comparison down in the cheapest GLP-1 guide, which ranks every access method by real per-month cost. If you are on Medicare or between plans, the Medicare GLP-1 bridge guide covers coverage gaps and workarounds. Cost-conscious readers should start there before committing to anything.
The honest bottom line
The best peptides for weight loss are, overwhelmingly, the GLP-1 class incretin drugs. Retatrutide leads on raw efficacy but is still investigational. Tirzepatide is the best option you can actually get prescribed today. Semaglutide is the proven, widely available workhorse. CagriSema is closing in from the amylin direction.
Everything below that tier is either narrow (tesamorelin for visceral fat), unproven in humans (MOTS-c), or a documented failure (AOD-9604). A good research peptide list should tell you that instead of padding the rankings.
If you want results, choose from the top of the table and pick your route: supervised telehealth through Yucca Health for a prescribed program, or research-grade vials from Ascension for lab work. Do not let a marketing page talk you into a growth-hormone fragment when the incretins have the trials.
Educational content only, not medical advice. GLP-1 medications such as semaglutide, tirzepatide, and their compounded forms are prescription drugs that require evaluation by a licensed clinician. Research-grade peptides referenced here are sold for laboratory and research use only, are not approved for human consumption, and are not quality-controlled as medicines. Consult a qualified healthcare provider before starting any weight-loss medication.