At a glance
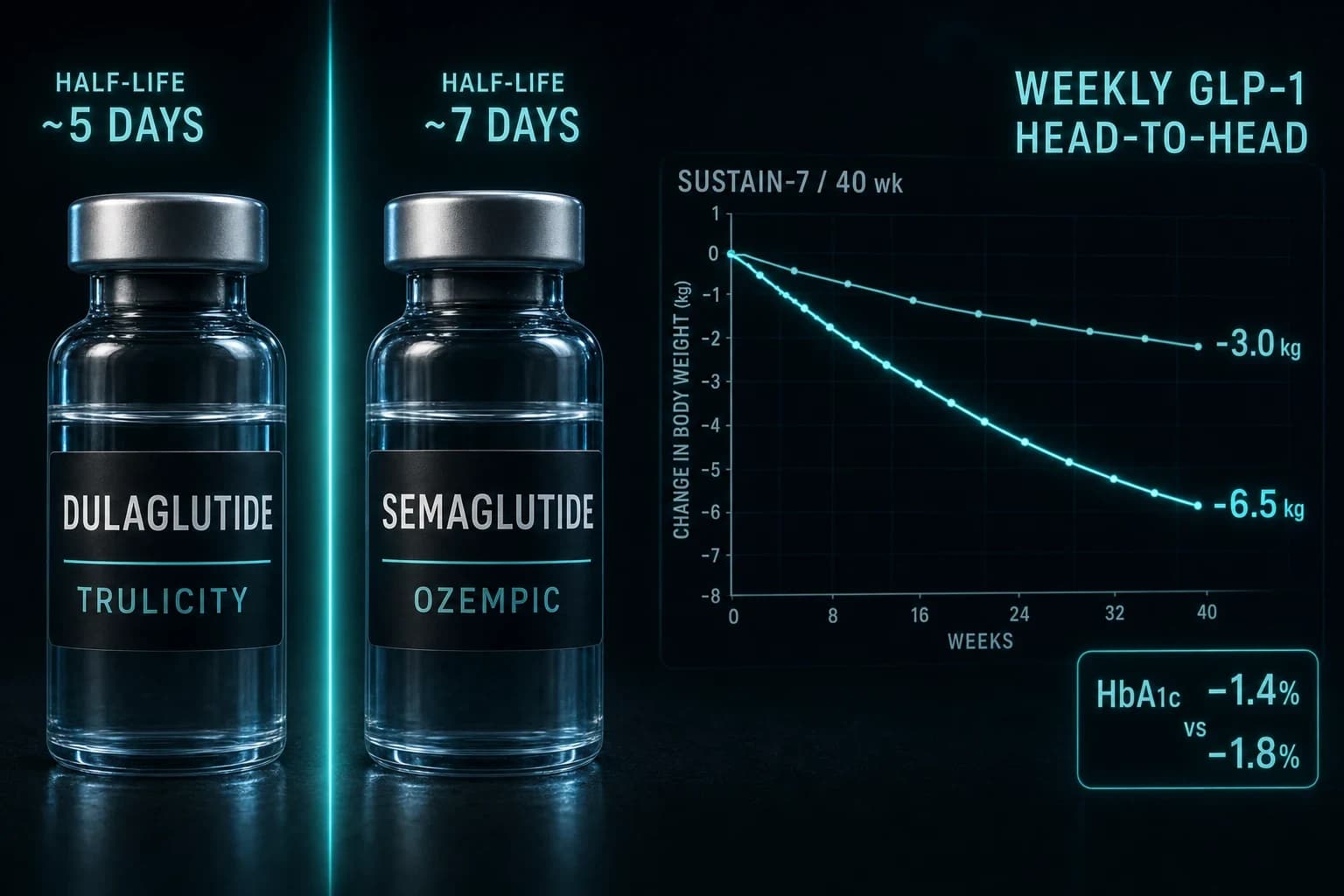
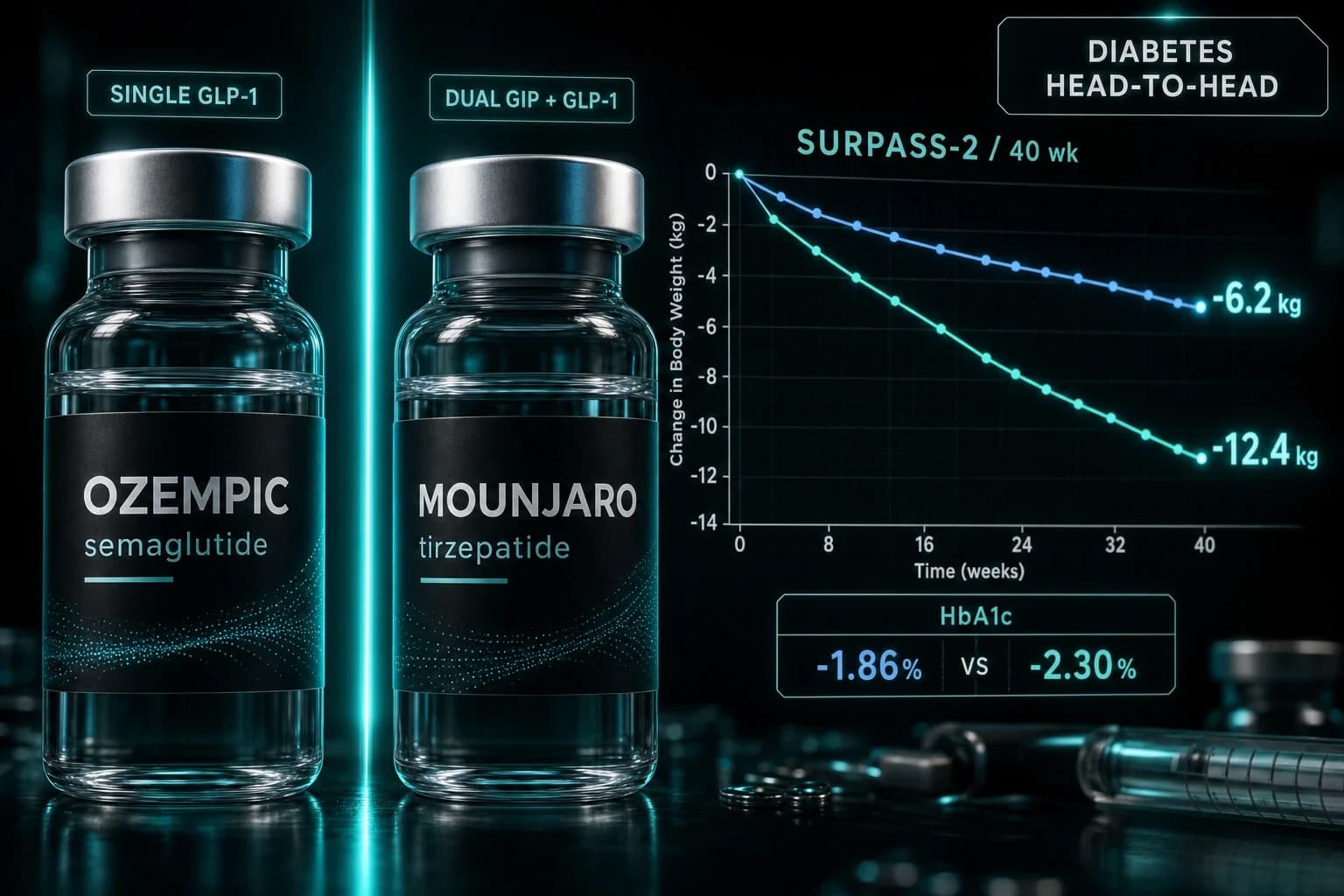
- In SURPASS-2, tirzepatide cut HbA1c 2.30% vs 1.86% for semaglutide over 40 weeks
- Tirzepatide lost 12.4 kg vs semaglutide's 6.2 kg head-to-head (Frías 2021)
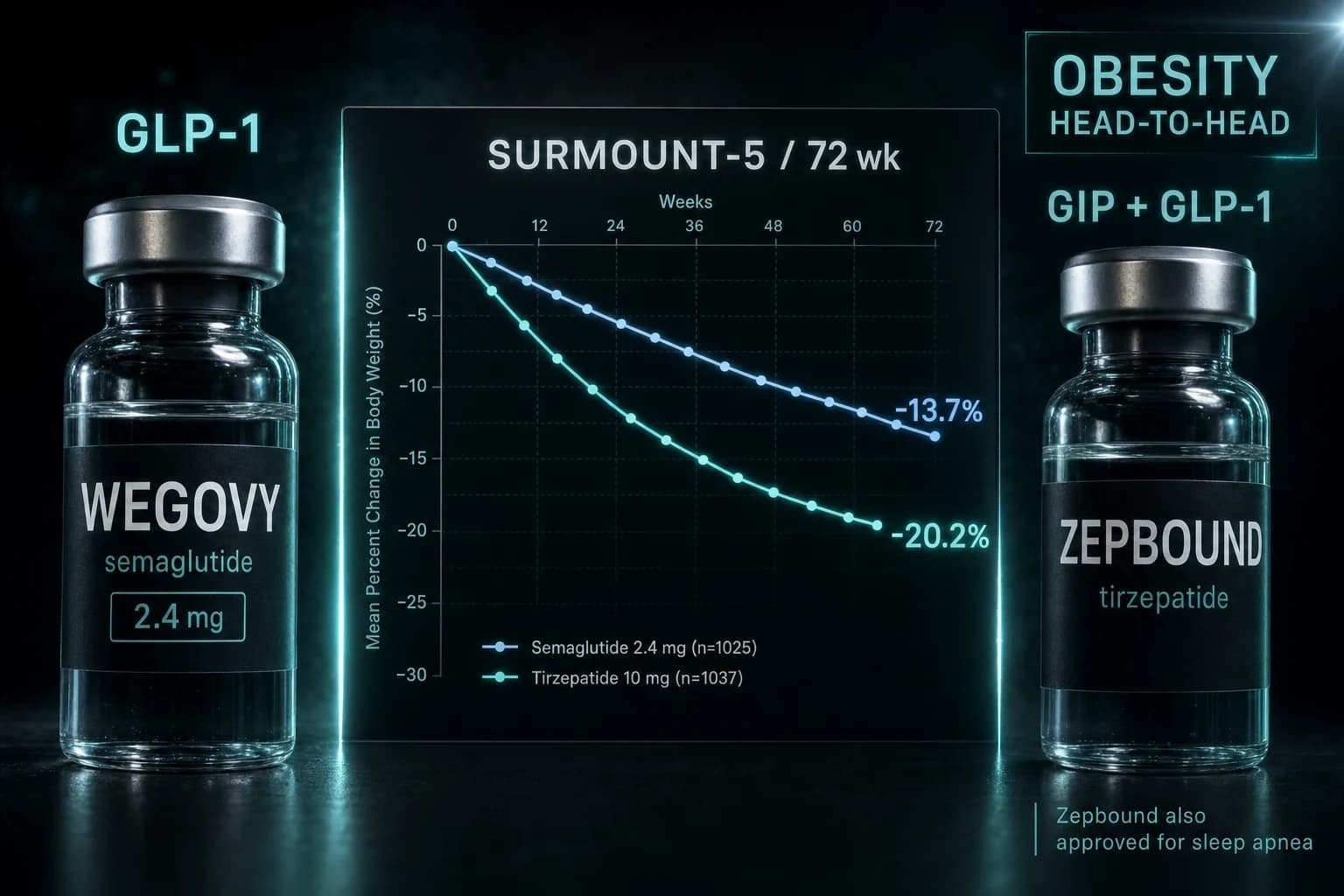
- Both are FDA-approved for type 2 diabetes, not obesity; Wegovy and Zepbound hold that
- Semaglutide has dedicated CV outcomes data: SUSTAIN-6 cut MACE 26% (HR 0.74)
- Mounjaro tops Ozempic for weight and glucose; Ozempic has the longer safety record
The one time Ozempic and Mounjaro were tested against each other, it was not close. In SURPASS-2, a 40-week head-to-head trial in 1,879 adults with type 2 diabetes, the top dose of tirzepatide (Mounjaro) dropped HbA1c by 2.30% and cut 12.4 kg of body weight. Semaglutide (Ozempic) at 1 mg managed 1.86% and 6.2 kg over the same weeks, in the same patients, on the same weekly schedule (Frías et al. 2021).
That result answers the question most people are typing into a search bar. But "which one is stronger" is not the only thing worth knowing before you ask a clinician for either drug, because these two were built for the same disease and carry very different track records.
Here is the full comparison, with the numbers that matter.
Two diabetes drugs everyone uses for weight
Start with the part the marketing buries. Ozempic and Mounjaro are both FDA-approved to lower blood sugar in type 2 diabetes. Neither one is approved to treat obesity. Novo Nordisk sells the exact same molecule as semaglutide under the Ozempic label for diabetes and the Wegovy label for weight. Eli Lilly does the identical thing with tirzepatide: Mounjaro for diabetes, Zepbound for obesity.
So when someone says they lost 40 pounds "on Ozempic," they are usually taking a diabetes drug off-label, or they are actually on Wegovy and calling it Ozempic because that is the name they recognize. The active ingredient is the same. The dose ceiling and the FDA label are not.
That distinction drives cost, insurance coverage, and dosing, which is why an honest comparison keeps the brands and the molecules straight. If your goal is purely weight, the cleaner brand-to-brand fight is Wegovy vs Zepbound. If you want the semaglutide-specific angle, Ozempic vs Wegovy explains why one molecule wears two names at two prices.
Ozempic vs Mounjaro at a glance
| Feature | Ozempic (semaglutide) | Mounjaro (tirzepatide) |
|---|---|---|
| Maker | Novo Nordisk | Eli Lilly |
| Molecule | Semaglutide, a GLP-1 analog | Tirzepatide, a GLP-1 analog with added GIP activity |
| Mechanism | Single GLP-1 receptor agonist | Dual GIP/GLP-1 receptor agonist |
| Max weekly dose | 2 mg | 15 mg |
| HbA1c drop (SURPASS-2) | -1.86% (1 mg arm) | -2.30% (15 mg arm) |
| Avg weight loss (SURPASS-2) | -6.2 kg | -12.4 kg |
| Cardiovascular data | SUSTAIN-6 (HR 0.74), SELECT (HR 0.80) | No dedicated MACE-superiority trial published |
| FDA-approved use | Type 2 diabetes (obesity = Wegovy) | Type 2 diabetes (obesity = Zepbound) |
One receptor versus two
Both drugs copy GLP-1, the gut hormone you release after eating. GLP-1 tells the pancreas to release insulin when glucose is high, tells the liver to stop dumping sugar, slows how fast the stomach empties, and turns down appetite signaling in the brain. Native GLP-1 gets broken down in about two minutes. Both semaglutide and tirzepatide are engineered to survive for roughly a week, so a single weekly injection keeps the signal running.
That is where Ozempic stops and Mounjaro keeps going. Semaglutide hits one target: the GLP-1 receptor. Tirzepatide is a dual agonist. It switches on GLP-1 and a second receptor, GIP (glucose-dependent insulinotropic polypeptide), another gut hormone tied to insulin release and fat metabolism. Two levers instead of one.
The theory was that adding GIP would deepen both glucose control and weight loss. SURPASS-2 is the evidence that it did.
SURPASS-2: the only true head-to-head
Most drug comparisons stitch together separate trials with different patients, so the numbers never quite line up. Ozempic and Mounjaro are one of the rare pairs tested directly against each other, which is why SURPASS-2 carries so much weight.
The design was clean. 1,879 adults with type 2 diabetes on metformin, randomized to tirzepatide 5, 10, or 15 mg or to semaglutide 1 mg, all once weekly for 40 weeks (Frías et al. 2021). Every tirzepatide dose beat semaglutide on both endpoints. At the top dose, tirzepatide reduced HbA1c by 2.30% versus 1.86%, and body weight by 12.4 kg versus 6.2 kg. The estimated treatment difference in weight reached 5.5 kg in tirzepatide's favor, all with p<0.001.
Note the asterisk: semaglutide was capped at 1 mg in that trial, below the 2 mg Ozempic ceiling now available. A higher semaglutide dose narrows the gap somewhat. It does not erase it. Tirzepatide's dual mechanism produced more glucose lowering and more weight loss when the two went head to head.
Bottom line: On raw glucose and weight numbers, Mounjaro (tirzepatide) beats Ozempic (semaglutide) in the only trial that put them in the same room. Ozempic's counterargument is not potency. It is track record.
Weight loss: the obesity trials tell the same story
Neither Ozempic nor Mounjaro was studied for weight at its diabetes label, so the cleanest weight data comes from the obesity-branded siblings dosed higher.
Semaglutide 2.4 mg (the Wegovy dose) produced a 14.9% mean body weight reduction over 68 weeks in STEP 1 (Wilding et al. 2021). Tirzepatide 15 mg (the Zepbound dose) produced a 20.9% reduction over 72 weeks in SURMOUNT-1, with 57% of participants losing more than a fifth of their starting weight (Jastreboff et al. 2022).
Those are separate trials with different populations, so the head-to-head caveat applies. Still, a roughly 6-point gap in average weight loss, pointing the same direction as SURPASS-2, is hard to hand-wave away. If maximum weight loss is the single thing you care about, tirzepatide is the stronger molecule. For a broader look at how both stack up against other options, see the best peptides for weight loss.
Cardiovascular data: Ozempic's real advantage
This is where the older drug pulls ahead. Semaglutide has two dedicated cardiovascular outcomes trials behind it.
In SUSTAIN-6, semaglutide cut the rate of major adverse cardiovascular events (cardiovascular death, nonfatal heart attack, or nonfatal stroke) by 26% in high-risk type 2 diabetes patients, a hazard ratio of 0.74 (Marso et al. 2016). SELECT then extended the finding to people with obesity and heart disease but no diabetes, cutting the same composite by 20%, a hazard ratio of 0.80 (Lincoff et al. 2023).
Tirzepatide does not yet have a comparable published cardiovascular-outcomes readout showing it prevents heart attacks and strokes. Its dual-agonist story is newer, and the long dedicated CV evidence base is still maturing. If you have established heart disease, that gap is not academic. It is the reason a cardiologist might reach for semaglutide even though tirzepatide moves the scale further.
Side effects: mostly a tie
Both drugs share the GLP-1 side effect profile, and it is driven by the same slowed gastric emptying that curbs appetite. Nausea, diarrhea, constipation, and vomiting lead the list, usually worst during dose escalation and fading as the body adjusts. Across SURPASS-2 and SURMOUNT-1, gastrointestinal effects were the most common reason people stopped, and rates were broadly similar between the two molecules.
Warning: Both carry a boxed warning for thyroid C-cell tumors based on rodent data and are contraindicated if you or your family have a history of medullary thyroid carcinoma or MEN 2. Pancreatitis, gallbladder disease, and low blood sugar (especially when combined with insulin or a sulfonylurea) are real risks. These are prescription drugs for a reason. Neither belongs in a self-directed protocol.
How to actually get either one
If you and a clinician decide semaglutide or tirzepatide is right for you, there are three realistic routes.
Brand-name Ozempic or Mounjaro through your own doctor and insurance is the gold standard, when it is covered. Coverage for the diabetes labels is common; coverage for weight is spotty, and Medicare has historically excluded anti-obesity drugs, which is the whole reason the Medicare GLP-1 bridge question keeps coming up.
The second route is prescribed telehealth with compounded GLP-1. You complete an online intake, a US-licensed clinician reviews your history and eligibility, and if it is appropriate a compounding pharmacy fills the prescription and ships it to your door. No insurance and no in-person visit required. Programs like Yucca Health run this model for both molecules, so it works whether you want the compounded semaglutide route or the compounded tirzepatide route. It is the same medical supervision, minus the waiting room.
The third factor is price. Brand pens without coverage can run four figures a month, while compounded and cash-pay options vary widely. If cost is the deciding vote, start with the current cheapest GLP-1 options before you commit to a brand.
Note: Research-grade semaglutide and tirzepatide vials also exist for laboratory use, available from Ascension Peptides with 50% off using code ENHANCED. That is not the same thing as a prescribed, pharmacy-compounded product, it is not quality-controlled for human use, and it is not a substitute for clinical supervision. For a drug you inject weekly, the prescribed telehealth route is the one that belongs in this comparison.
So which one wins
If you want the biggest drop in weight and blood sugar and have no specific cardiac concern, tirzepatide (Mounjaro) is the stronger molecule, and SURPASS-2 is the receipt. If you have established cardiovascular disease, or you simply want the drug with the longest and deepest outcomes record, semaglutide (Ozempic) earns its edge on data, not marketing.
Neither choice is one you make alone. Both are prescription drugs with real contraindications, and the right answer depends on your labs, your heart, your history, and what your coverage will actually pay for.
Disclaimer
This article is for educational purposes only and is not medical advice. Ozempic and Mounjaro are prescription drugs approved for type 2 diabetes; Wegovy and Zepbound are the obesity-approved siblings. Any decision to start, stop, or switch a GLP-1 medication should be made with a licensed clinician who knows your full medical history. Nothing here is a recommendation to obtain or use these drugs outside of proper medical supervision.