At a glance
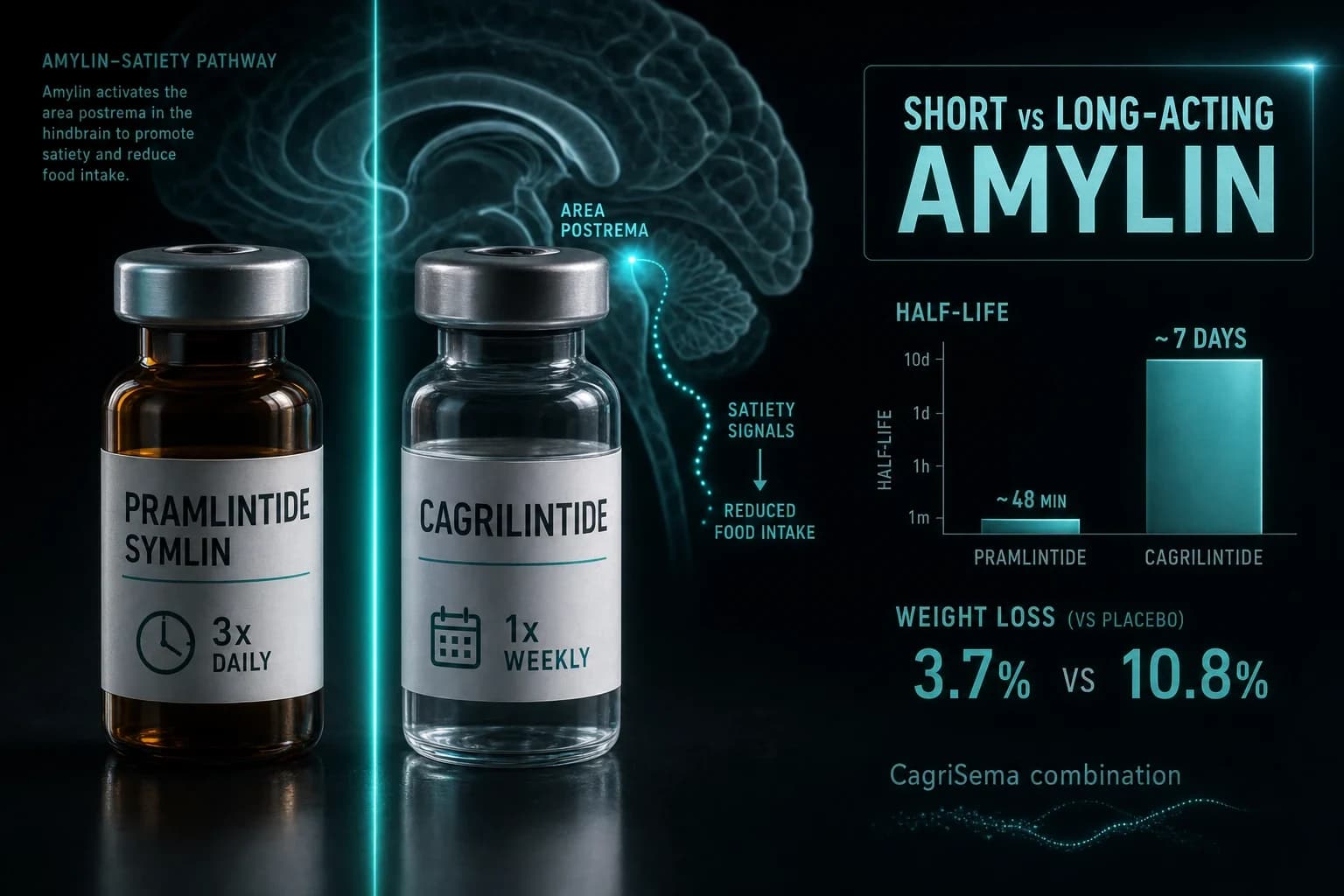
- Pramlintide has a ~48-minute half-life and needs dosing before every meal; cagrilintide lasts ~7 days and is dosed once weekly.
- Pramlintide (Symlin) is FDA-approved with a boxed warning for severe insulin-induced hypoglycemia; cagrilintide is investigational only.
- Cagrilintide 4.5 mg produced 10.8% weight loss at 26 weeks vs 3.0% placebo (Lau 2021); pramlintide managed ~3.7% placebo-corrected (Aronne 2007).
- Combined with semaglutide as CagriSema, cagrilintide drove 22.7% weight loss at 68 weeks in REDEFINE 1 (Garvey 2025).
- Same hormone, opposite clocks: half-life is the single variable that changes dosing, use case, and legal status.
Two drugs. Same hormone. Opposite clocks.
Pramlintide is gone from your bloodstream in under an hour. Cagrilintide is still working a week after you inject it. Both are synthetic versions of amylin, the pancreatic hormone that tells your brain you have eaten enough. But that single difference in half-life, roughly 48 minutes versus roughly 7 days, decides everything downstream: how often you dose, what the drug is actually good for, and whether it comes from a pharmacy shelf or a research vial.
If you are trying to figure out which amylin analog matters for your protocol, start with the clock. Everything else follows from it.
What amylin actually does
Amylin is co-secreted with insulin from the same pancreatic beta cells. When you eat, both hormones spike together. Insulin handles the glucose. Amylin handles the pacing.
It does three things at once. It slows how fast your stomach empties, so glucose enters the blood more gradually. It suppresses glucagon, the hormone that tells your liver to dump more sugar into circulation after a meal. And it acts on the area postrema in your hindbrain to increase satiety, the physical sense of fullness that ends a meal (Traina and Kane, 2011).
Native amylin is useless as a drug. It aggregates and clumps in solution, which is exactly why researchers had to engineer stable analogs. Pramlintide was the first. Cagrilintide is the modern rebuild. They target the same receptors and produce the same felt effect, reduced appetite, but they are built on completely different timelines.
Pramlintide: the short-acting original
Pramlintide has been around since 2005. It is the amylin analog with an actual FDA approval and decades of clinical data behind it, sold as Symlin.
The catch is the pharmacokinetics. Pramlintide has a half-life of about 48 minutes. That is not a typo. To match natural amylin's mealtime rhythm, you inject it separately from your insulin before every major meal, which in practice means three subcutaneous shots a day. It was designed as a mealtime adjunct for people with type 1 or type 2 diabetes who already use insulin, not as a standalone drug.
The diabetes data is solid. In a 52-week randomized controlled trial, Hollander et al. (2003) gave type 2 diabetics 120 mcg twice daily alongside insulin. HbA1c dropped 0.62% at one year, and body weight fell 1.4 kg while the placebo group gained 0.7 kg. Modest, but real, and notable because most diabetes drugs cause weight gain, not loss.
That weight signal is what pushed researchers to test pramlintide in obesity without diabetes. Aronne et al. (2007) ran a 16-week dose-escalation study in obese subjects, titrating up to 240 mcg three times daily. The result was a placebo-corrected weight reduction of 3.7%, with 31% of the pramlintide group losing at least 5% of body weight versus 2% on placebo. Proof of concept, clearly. But 3.7% over four months is not competitive with anything in the current GLP-1 era, and the three-shots-a-day schedule is a genuine adherence problem.
Warning: Pramlintide carries an FDA boxed warning for severe insulin-induced hypoglycemia. Used with mealtime insulin, it can cause a dangerous blood sugar crash, with the highest risk in the first 3 hours after injection. The label requires cutting mealtime insulin by 50% when starting and monitoring glucose closely. This is a genuine safety issue, not a formality.
Pramlintide's problem was never efficacy. It was the delivery. A drug that clears in 48 minutes will always demand frequent dosing, and frequent injections are where real-world compliance goes to die. You can read the full mechanism and dosing breakdown on our pramlintide guide.
Cagrilintide: the once-weekly successor
Cagrilintide is Novo Nordisk's answer to pramlintide's clock problem. Same hormone class, re-engineered for endurance.
Through acylation, attaching a fatty acid chain that binds albumin and slows clearance, cagrilintide's half-life stretches to roughly 180 hours, about 7 to 8 days (Mathiesen et al., 2022). That is a two-hundred-fold jump over pramlintide. It converts a three-times-daily mealtime drug into a once-weekly subcutaneous injection, the same cadence as semaglutide.
The efficacy scales with the exposure. In a 26-week phase 2 dose-finding trial, Lau et al. (2021) tested five cagrilintide doses in 706 adults with overweight or obesity. The top dose, 4.5 mg weekly, produced 10.8% weight loss versus 3.0% for placebo. It also edged out liraglutide 3.0 mg, which managed 9.0% in the same trial. As a monotherapy, that already roughly triples pramlintide's obesity result, and it does it on one shot a week instead of twenty-one.
The trade-off is the same one every gut-acting drug shares. Nausea was the dominant side effect, more frequent with cagrilintide than placebo, though mostly transient and dose-dependent. Our cagrilintide guide covers the titration schedule researchers use to blunt it.
But cagrilintide's monotherapy numbers, while good, are not the reason anyone is paying attention. The real story is what happens when you pair it with a GLP-1.
Pramlintide vs cagrilintide: the head-to-head
| Factor | Pramlintide (Symlin) | Cagrilintide |
|---|---|---|
| Half-life | ~48 minutes | ~7 days (180 hrs) |
| Dosing | Before each meal (3x daily) | Once weekly |
| Injections per week | ~21 | 1 |
| Approval status | FDA-approved (2005) | Investigational only |
| Primary use | Mealtime insulin adjunct for diabetes | Obesity (in development) |
| Peak weight loss (mono) | ~3.7% placebo-corrected, 16 wks | 10.8% vs 3.0% placebo, 26 wks |
| Boxed warning | Yes (severe insulin hypoglycemia) | None (not approved) |
| Combination play | None | CagriSema (with semaglutide) |
The table makes the split obvious. Pramlintide is the approved, well-characterized, but logistically painful mealtime tool. Cagrilintide is the once-weekly, higher-ceiling, but still-investigational contender whose future is tied to a combination.
CagriSema: why cagrilintide's real story is a combination
Amylin and GLP-1 hit fullness through different pathways. Stacking them is additive, and that is the entire premise behind CagriSema, a co-formulation of cagrilintide 2.4 mg and semaglutide 2.4 mg in a single once-weekly injection.
The phase 3 REDEFINE 1 trial put it to the test. Garvey et al. (2025) randomized 3,417 adults with obesity to CagriSema, semaglutide alone, cagrilintide alone, or placebo over 68 weeks. CagriSema delivered 22.7% mean weight loss (20.4% under the more conservative treatment-policy estimand) versus 3.0% for placebo. The individual components landed lower: cagrilintide 2.4 mg alone produced 11.8%, and semaglutide 2.4 mg alone produced 16.1%. The combination beat both, which is the whole point. Sixty percent of participants on CagriSema lost at least 20% of their body weight, and 23% lost 30% or more.
REDEFINE 2 ran the same combination in adults with type 2 diabetes, historically a harder population to move the scale in. Davies et al. (2025) reported 13.7% weight loss versus 3.4% on placebo at 68 weeks, and 73.5% of the CagriSema group reached an HbA1c of 6.5% or lower, compared with 15.9% on placebo.
Bottom line: Cagrilintide's monotherapy weight loss (10.8%) is respectable. Its combination weight loss inside CagriSema (22.7%) is what puts it in direct conversation with tirzepatide. Amylin's future in obesity is almost certainly as a partner to GLP-1, not a solo act.
That framing matters when you compare it to the current standard. Semaglutide alone tops out around 15 to 16% in this exact trial, and tirzepatide, the dual GIP/GLP-1 agonist, sits in the low-to-mid 20s. CagriSema's 22.7% pulls amylin-plus-GLP-1 into that same top tier. Pramlintide, for all its history, was never going to get there on a three-shot-a-day schedule.
How to think about half-life for your protocol
Half-life is not trivia. It is the design constraint that dictates the entire protocol.
A 48-minute half-life means pramlintide must be timed to meals and can never be a set-and-forget drug. It also means the effect is over quickly, which is precisely why the hypoglycemia risk concentrates in a narrow window right after injection. Short action cuts both ways: less accumulation, but relentless dosing.
A 7-day half-life means cagrilintide reaches steady state gradually over several weeks, which is why researchers titrate the dose up slowly rather than starting high. The long tail is what makes once-weekly dosing work, and it is also why nausea tends to fade as the body acclimates to a stable exposure. If you are reconstituting research-grade cagrilintide, that slow titration is where accuracy counts. Our reconstitution calculator handles the mcg-per-unit math so your weekly dose is actually the dose you intended.
Sourcing and legal status
This is where the two compounds fully diverge.
Pramlintide is a prescription drug. As Symlin, it is FDA-approved and dispensed through a pharmacy for insulin-using diabetics, complete with the boxed warning and the required insulin-dose adjustments. It is not something you source as a research chemical, and given the hypoglycemia risk, it should not be used outside medical supervision.
Cagrilintide has no approval yet. It exists in clinical trials and, for research purposes, as a research-grade peptide. Researchers studying amylin signaling can source cagrilintide from Ascension Peptides with 50% off using code ENHANCED. Pair it with their semaglutide if you are modeling the CagriSema combination that REDEFINE validated.
Bottom line: Choose by clock and by legal status. Pramlintide is the approved short-acting mealtime tool with a real hypoglycemia warning. Cagrilintide is the investigational once-weekly compound with the higher ceiling, especially alongside a GLP-1. They are the same hormone solving the same problem on two different timescales.
This article is for research and educational purposes only. It is not medical advice. Cagrilintide is an investigational compound not approved for human use outside of clinical trials. Pramlintide (Symlin) is a prescription medication that should only be used under the supervision of a licensed healthcare provider. Nothing here should be interpreted as a recommendation to purchase or use any compound outside of a properly authorized research setting.