At a glance
- No controlled trial has tested semaglutide or tirzepatide below the FDA-approved starting doses of 0.25 mg and 2.5 mg weekly.
- STEP 1 semaglutide 2.4 mg produced 14.9% weight loss at 68 weeks; the 0.25 mg starting dose is a tolerability step, not a therapeutic dose (Wilding 2021, PMID 33567185).
- SURMOUNT-1 tirzepatide showed a clean dose-response: 15.0% at 5 mg, 19.5% at 10 mg, 20.9% at 15 mg (Jastreboff 2022, PMID 35658024).
- STEP 4 showed the 2.4 mg maintenance dose held the loss; switching to placebo drove roughly 6.9% regain within 48 weeks (Rubino 2021, PMID 33755728).
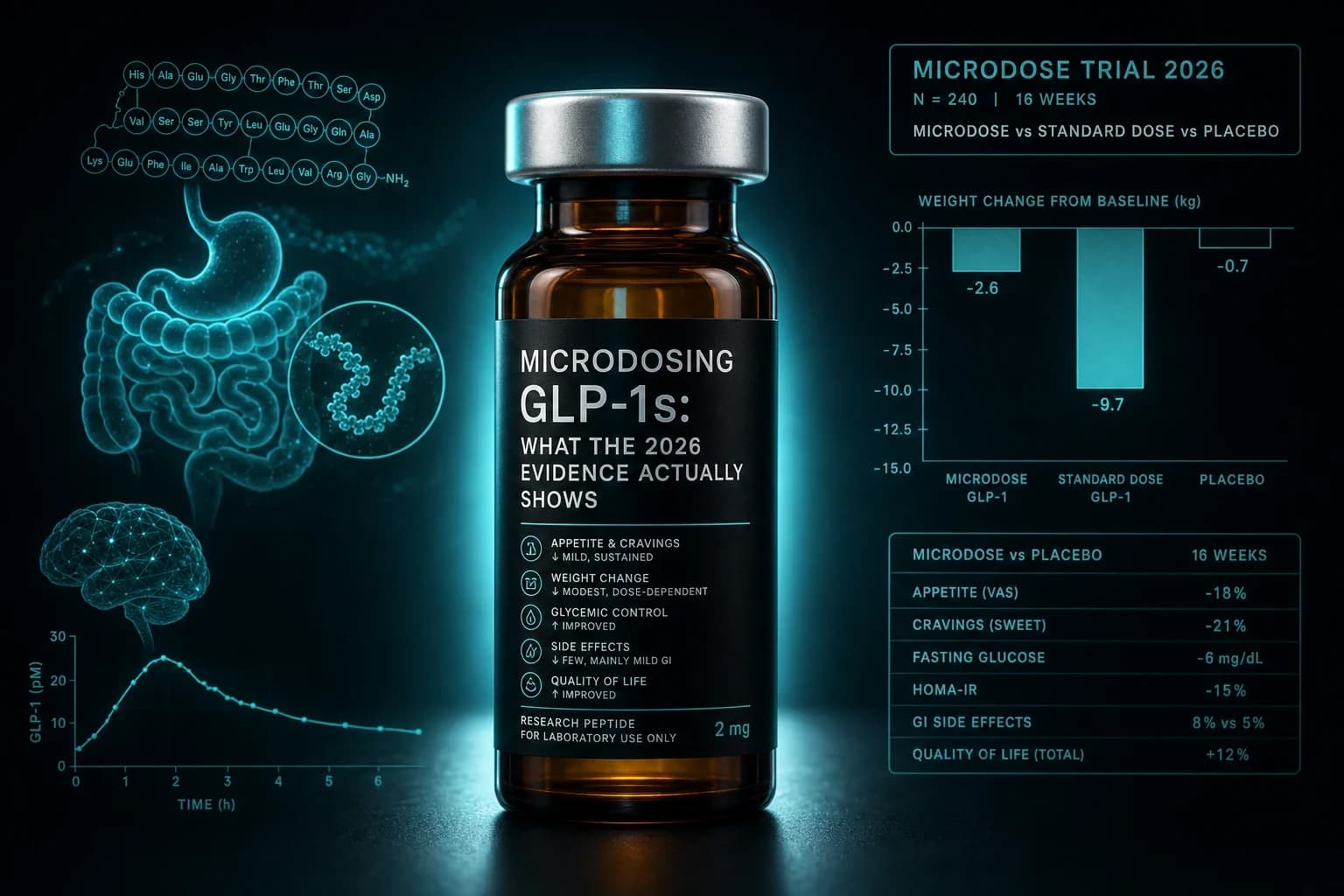
- A 2026 Evidation Health survey found ~15% of injectable GLP-1 users microdose, mostly to manage side effects or stretch cost.
Someone in your gym locker room says they are microdosing Ozempic. A telehealth ad promises "gentle" tirzepatide at half the price. A Reddit thread swears that 0.1 mg weekly kept the weight off with none of the nausea. The pitch is always the same. All of the benefit. None of the cost. None of the side effects. None of the muscle loss.
Here is the problem. No controlled trial has ever tested semaglutide or tirzepatide below the FDA-approved starting doses. The 0.25 mg semaglutide dose you see quoted is not a therapeutic dose in the labels. It is a tolerability step that people escalate off in four weeks. The 2.5 mg tirzepatide starting dose is the same. The pharmacology argument for microdosing is real. The clinical trial argument is essentially empty. Both things can be true, and this article treats them as such.
What people mean by "microdosing" a GLP-1
Search results and forum threads use "microdose" loosely. Working definitions we see most often:
- Semaglutide: 0.05 to 0.25 mg weekly, held indefinitely instead of titrated up.
- Tirzepatide: 0.5 to 2.5 mg weekly, held indefinitely instead of titrated up.
- Retatrutide: 0.5 to 2 mg weekly, well below the 4 to 12 mg trial arms.
The other flavor of "microdosing" is what pharmacologists would call maintenance dosing: someone who titrated up to a therapeutic dose, lost weight, and then dropped back to a small fraction to preserve the loss without side effects. That is closer to a real question the trials touch, and we will treat it separately from the "start low, stay low" pattern that dominates the marketing.
A 2026 Evidation Health member survey reported roughly 15% of injectable GLP-1 users described their regimen as a microdose, with side effect avoidance and cost cited as the top two reasons. Nothing about that survey validates the practice on efficacy. It documents that people are doing it.
Bottom line: "Microdose" is a marketing word. There is no FDA-recognized subclinical dosing tier for semaglutide or tirzepatide, and no controlled human data at the doses being sold as microdoses.
What the pivotal trials actually tested
The whole microdose conversation gets easier once you look at what got measured and at what dose. Here are the trial arms that anchor the label for each drug.
| Trial | Compound | Dose(s) tested | Duration | Mean weight loss | Reference |
|---|---|---|---|---|---|
| STEP 1 | Semaglutide | 2.4 mg weekly | 68 weeks | 14.9% | Wilding et al. NEJM 2021, PMID 33567185 |
| STEP 2 | Semaglutide | 2.4 mg vs 1.0 mg vs placebo (T2D) | 68 weeks | 9.6% (2.4) vs 7.0% (1.0) vs 3.4% | Davies et al. Lancet 2021, PMID 33667417 |
| STEP 4 | Semaglutide | 2.4 mg continued vs placebo switch | 48 weeks post-randomization | -7.9% continued vs +6.9% placebo | Rubino et al. JAMA 2021, PMID 33755728 |
| STEP UP | Semaglutide | 7.2 mg vs 2.4 mg vs placebo | 72 weeks | 18.7% (7.2) vs 15.6% (2.4) vs 3.9% | Aronne et al. Lancet Diab Endo 2025, PMID 40961952 |
| SURMOUNT-1 | Tirzepatide | 5, 10, 15 mg weekly | 72 weeks | 15.0%, 19.5%, 20.9% | Jastreboff et al. NEJM 2022, PMID 35658024 |
| Phase 2 | Retatrutide | 4, 8, 12 mg weekly | 48 weeks | 8.7%, 22.8%, 24.2% | Jastreboff et al. NEJM 2023, PMID 37366315 |
Two patterns fall out of that table.
First, dose matters. STEP 2 is the cleanest apples-to-apples semaglutide dose comparison inside a single trial. At 68 weeks, 2.4 mg produced 9.6% weight loss in adults with type 2 diabetes; 1.0 mg produced 7.0%; placebo produced 3.4%. That is a real gap between 1.0 and 2.4, and the 1.0 mg arm is the highest dose FDA-approved for diabetes glycemic control, not for weight loss. STEP UP extended the ladder upward and again the higher dose won, with 7.2 mg producing 18.7% loss versus 15.6% for the standard 2.4 mg arm at 72 weeks.
Second, no arm in any of these trials tested doses under the starting titration step. Semaglutide 0.25 mg is not a Phase 3 arm anywhere. Tirzepatide 2.5 mg is a titration step that everyone escalated off after four weeks. The lowest published human dose-response data for tirzepatide sits at 5 mg, and even that is only tested for 20 weeks in the SURMOUNT-1 dose escalation before people moved up.
If you want to see the full weekly ladder in plain reference form, our semaglutide dosage chart and tirzepatide dosage chart show the FDA-approved steps side by side with what the pivotal trials actually studied.
What "microdose" doses would look like on that ladder
Slotting the common microdose ranges into the pivotal trial framework makes the extrapolation gap obvious.
| Microdose regimen | Weekly dose | Ratio vs. trial target | Human RCT data at this dose |
|---|---|---|---|
| Semaglutide "gentle" | 0.10 mg | ~1/24 of STEP 1 target | None |
| Semaglutide "starter hold" | 0.25 mg | ~1/10 of STEP 1 target | None as a maintained dose; only as a 4-week titration step |
| Semaglutide half-diabetes | 0.5 mg | ~1/5 of STEP 1 target | Approved for T2D glycemic control; not tested as obesity monotherapy |
| Tirzepatide "gentle" | 1.0 mg | ~1/15 of SURMOUNT-1 top dose | None |
| Tirzepatide "starter hold" | 2.5 mg | ~1/6 of SURMOUNT-1 top dose | None as a maintained dose; titration step only |
| Retatrutide "starter" | 1.0 mg | ~1/12 of Phase 2 top dose | None as a therapeutic dose |
None of the rows in that table are supported by a Phase 3 endpoint. That is the crux of the microdose problem. The pharmacology tells you these compounds still hit the receptor at those doses. The clinical trial tells you nothing about what percent of body weight anyone actually loses, how the loss curve levels off, how long people stick with it, or what the side effect profile looks like at that receptor occupancy.
Absence of evidence is not evidence of absence. That is true here. It is also true that "we do not know" is not the same as "it works but no one has bothered to prove it," which is how the practice is often marketed.
Warning: Extrapolating linearly down from Phase 3 dose-response is dangerous. GLP-1 receptor agonism produces effects at very low occupancy, but non-linear relationships between plasma exposure and appetite/satiety response are the norm, not the exception. Expect surprises in either direction.
Why anyone microdoses in the first place
Three reasons show up in surveys and forum threads more than any others. Each has a real pharmacologic hook, and each has a specific failure mode.
Reason 1: Side effects. The GI tolerability of full-dose semaglutide and tirzepatide is not a rumor. STEP 1 reported nausea in 44%, diarrhea in 32%, and vomiting in 25% of the semaglutide 2.4 mg arm (Wilding et al. NEJM 2021, PMID 33567185). STEP 2 confirmed the same pattern at 2.4 mg in adults with type 2 diabetes and showed a lower rate in the 1.0 mg arm (Davies et al. Lancet 2021, PMID 33667417). The intuition that a smaller dose means fewer GI events is directionally correct within the tested ranges.
Failure mode: side effects follow a dose-response, but so does efficacy. If your goal is meaningful weight loss and metabolic improvement, dropping below the studied doses drops you into a zone where nobody has measured what you get back for the tolerability gain. The right lever if GI events are the blocker is a slower titration or an anti-nausea rescue, not permanent subclinical dosing.
Reason 2: Cost. Compounded semaglutide and tirzepatide from a 503A pharmacy or a legitimate telehealth partner can run $150 to $400 per month. Buying research-grade compound and dosing yourself puts the monthly cost near $80 to $150. Microdosing stretches the same vial across three to six times as many weeks. This is real math, and it is the reason cost sits second in every survey.
Failure mode: cost pressure pushes people to grey-market suppliers whose product may not be what the label claims. A certificate of analysis matters more than the dose you inject when the compound came from an unverified source. If money is the constraint, a legitimate compounded partner at a standard dose usually beats an unverified compound at a microdose. Vetted compounded routes are covered in our compounded semaglutide access guide and compounded tirzepatide access guide.
Reason 3: Weight-loss maintenance. This is the one case where the pharmacology and the trials point in the same direction. People who lose 15 to 20 percent of body weight on a therapeutic dose face a specific question: what dose keeps the loss? The rebound biology is now well-characterized. STEP 1 extension showed that stopping semaglutide 2.4 mg entirely triggered regain of 11.6 percentage points of weight over 68 weeks (Wilding et al. Diabetes Obes Metab 2022, PMID 35441470). STEP 4 showed that continuing the 2.4 mg dose held the loss and produced further reduction, while switching to placebo triggered a 6.9 percent regain in 48 weeks (Rubino et al. JAMA 2021, PMID 33755728).
Failure mode: STEP 4 tested "keep the maintenance dose" versus "stop entirely." It did not test "drop to a subclinical dose." The 15% to 20% loss required 2.4 mg, and STEP UP suggests that even more loss came from pushing to 7.2 mg (Aronne et al. Lancet Diab Endo 2025, PMID 40961952). Whether 0.5 mg or 1.0 mg holds the loss is a serious question with no controlled answer. Real-world evidence is starting to appear, but the systematic review of GLP-1 discontinuation trajectories is what practitioners should be watching, not testimonials.
For the deeper look at what discontinuation actually does, see the site's dedicated guide to stopping GLP-1s and weight regain.
The receptor pharmacology, explained honestly
The best pro-microdose argument leans on receptor occupancy. Semaglutide is a highly potent GLP-1 receptor agonist with a plasma half-life around 165 hours, meaning weekly dosing produces smooth exposure with a peak-to-trough ratio close to 1.4. Even sub-milligram doses produce meaningful receptor engagement in the pancreatic beta cell, the enteric neurons, and the hindbrain. Tirzepatide adds GIP agonism on top of GLP-1 and shows similar sustained exposure.
Two things follow from that.
First, low doses do something. Nobody serious argues that 0.25 mg of semaglutide is pharmacologically inert. It measurably slows gastric emptying, blunts postprandial glucose excursions, and reduces reported hunger scores in acute pharmacology studies. The mechanism exists at low doses.
Second, "does something" is not the same as "produces STEP 1-scale weight loss." Every controlled outcome we care about, appetite suppression that translates into 500 to 700 kcal per day of intake reduction, sustained loss curves, and preserved metabolic rate through the loss, was measured at 2.4 mg semaglutide and 10 to 15 mg tirzepatide. Extrapolating from receptor occupancy to that outcome without a trial is a leap the marketing routinely makes and the literature does not support.
The Lancet's February 2025 editorial on microdosing landed on this point plainly: the practice of microdosing drugs is not new, but there is no evidence that it works for obesity. That framing survived the STAT News May 2026 review and remains the honest one-line summary of the state of the field.
Safety at unstudied doses
Efficacy is the first question. Safety is the second, and the two do not track linearly. Here is what we know and do not know at microdose exposure.
- Pancreatitis: SURMOUNT-1 and the STEP program reported low rates of pancreatitis across the tested doses (Jastreboff et al. NEJM 2022, PMID 35658024). The site's pancreatitis risk deep dive covers the full data. Whether microdoses attenuate this risk is unknown; the mechanism is receptor-mediated, not just dose-mediated.
- Muscle loss: Lean mass loss during GLP-1 treatment is a real signal in DXA substudies. Whether reducing dose preserves lean mass without reducing fat loss proportionally has not been tested. See our muscle loss and lean mass preservation guide for the primary evidence base.
- Cardiovascular signal: SELECT established a 20% MACE reduction with semaglutide 2.4 mg. That signal has not been demonstrated at any microdose. Anyone using GLP-1s for cardiovascular protection should not assume subclinical doses inherit the benefit.
- Thyroid, gallbladder, gastroparesis: All three have documented associations at the tested doses. Whether they attenuate proportionally at microdoses is unknown.
- Rebound biology: Even at full doses, weight regain begins within weeks of discontinuation. It is possible that a subclinical maintenance dose partially blunts regain. It is also possible it does not blunt it enough to matter. Nobody has tested this in a controlled setting.
Note: The comparators worth reading here are the site's side effects deep dive on semaglutide and tirzepatide and the Reddit-adjacent evidence review. Every serious risk conversation starts with those.
A decision framework, honestly
The right question is not "should I microdose." The right question is "what am I actually trying to do." Different goals point to different regimens, and the evidence supports some of those regimens more than others.
| Your goal | Best evidence-supported route | What to avoid |
|---|---|---|
| Maximum weight loss | Titrate to 2.4 mg semaglutide or 10 to 15 mg tirzepatide over 12 to 20 weeks. Consider 7.2 mg semaglutide if approved and available in your region. | Holding at 0.25 mg or 2.5 mg to spare side effects. You are trading measured outcomes for unmeasured ones. |
| Modest weight loss with minimum GI events | Slow titration (extra 4 weeks per step), 1.0 mg semaglutide as a documented lower-efficacy but real-loss regimen. | Sub-1.0 mg semaglutide as a maintained dose with an efficacy expectation. |
| Maintenance after reaching goal | Continue the maintenance dose that produced the loss. If cost is prohibitive, discuss step-down protocols with a clinician. | Assuming a self-selected microdose preserves the loss. STEP 4 is the closest data and it did not test that. |
| Diabetes glycemic control | 1.0 mg semaglutide is the approved diabetes dose and produces measurable A1C reduction. | Sub-1.0 mg semaglutide for glycemic control. Not approved, not studied, not enough exposure to trust the effect. |
| Metabolic tune-up with no obesity | No trial supports this indication at any dose. Talk to a physician, not a compounding pharmacy. | Any regimen. This is not a documented use case at any dose. |
If your goal falls anywhere in the first three rows, the honest guidance is to run the trial-supported protocol first, then adjust based on measured tolerability. If the first three rows do not match your reason for asking, no dose of these drugs is an evidence-based fit for what you want.
For the practical protocol side, the 12-week titration ladder from the pivotal trials is captured in the retatrutide titration protocol reference, and the equivalent semaglutide and tirzepatide unit conversions live in the semaglutide reconstitution chart and tirzepatide reconstitution chart. Anyone measuring their own doses should also run the reconstitution calculator before mixing a vial.
What the microdose crowd gets right
The critique is not that these compounds behave like binary switches. They do not. Real dose-response data from STEP 2 and SURMOUNT-1 shows that lower doses produce measurable but proportionally smaller weight loss and better GI tolerability. Anyone who claims that only the top dose does anything is misreading the trial data as badly as anyone who claims sub-clinical doses replicate top-dose outcomes.
A reasonable version of the microdose argument does exist: for a person with modest weight loss goals, mild metabolic dysfunction, high side-effect sensitivity, and no urgency, a lower dose within the studied ranges may be a fair trade. The unreasonable version is anyone chasing STEP 1-scale weight loss without STEP 1-scale side effects and cost.
What the microdose crowd gets wrong
Three claims recur in the marketing that the literature does not support.
"You get most of the benefit with none of the side effects." No dose-response curve in the semaglutide or tirzepatide programs supports this. Efficacy and tolerability both scale with dose, in the same direction, within the studied ranges.
"Long-term microdosing preserves your metabolic set point." No trial has measured metabolic rate or set-point outcomes at microdoses. This claim is currently vibes-based.
"Compounded microdoses are just as good as the pen." Compounded semaglutide from a legitimate 503A pharmacy delivers the active molecule, but the FDA's March 2026 warning-letter cluster to telehealth companies flagged multiple misleading claims about efficacy at unstudied doses. Legitimate compounded routes exist; the "microdose is equivalent" framing is not one of them. If you are sourcing, verify the compounding pharmacy the same way you would verify a peptide vendor's certificate of analysis.
Cost and sourcing without the marketing gloss
If cost is the reason to consider microdosing, the more productive move is to make the full dose cheaper rather than the dose smaller. Two paths worth understanding side by side:
- Compounded 503A pharmacy access via telehealth. Standard weekly doses of compounded semaglutide or tirzepatide run several times cheaper than branded Ozempic, Wegovy, Mounjaro, or Zepbound. The cheapest GLP-1 access routes and the site's Yucca Health review for 2026 walk through the vetted paths and what to check before signing up. This is the honest cost-lever for people who need the drug at a therapeutic dose.
- Research-grade injectable peptides for lab use. Ascension Peptides carries research-grade semaglutide, tirzepatide, and retatrutide for laboratory use. Available with 50% off using code ENHANCED. That is not a clinical prescription, and it is not a substitute for medical supervision, but for research protocols the pricing usually beats compounded telehealth. Read the Ascension Peptides review for the sourcing and COA discussion before ordering.
Either route sits inside a documented dose. Neither route becomes a "microdose" just because it is cheaper.
The bottom line
There is a version of low-dose GLP-1 use that the literature supports: the 1.0 mg semaglutide diabetes dose, the 5 mg tirzepatide bottom rung of the SURMOUNT-1 ladder, and slow titrations that spend extra weeks at each step to smooth the tolerability curve. Those are real, measured, defensible regimens.
The version that the literature does not support is holding at 0.1 mg or 0.25 mg semaglutide as a therapeutic dose and expecting a chunk of the STEP 1 outcome. That is an extrapolation, not a protocol. Anyone selling it as science is confusing pharmacology with efficacy, and the difference matters when the reason you are chasing weight loss is health, appearance, or metabolic risk that you were told these drugs solve at their studied doses.
For research protocols, use the studied doses. For a maintenance regimen after real weight loss, ask a clinician who will actually track the outcome and adjust. For a cheaper option, use the compounded route at a real dose. The microdose story is neither a scam nor a solution. It is a gap in the evidence, and the honest answer is that gap has not been closed yet.
Bottom line: Zero controlled trials have tested semaglutide or tirzepatide below the FDA-approved starting doses. Every published outcome we care about happened at 2.4 mg semaglutide or 5 to 15 mg tirzepatide. Sub-clinical dosing may be reasonable in narrow cases; it is not a replacement for the trial-supported protocol.
Further reading on this site
- Tirzepatide vs semaglutide 2026 head-to-head
- Retatrutide, tirzepatide, and semaglutide compared
- GLP-1 dosing comparison across the class
- Stopping GLP-1s and the weight-regain literature
- Retatrutide side effects deep dive
Disclaimer
This article is for research and educational purposes only. It is not medical advice, not a treatment protocol, and not a substitute for consultation with a qualified physician. Semaglutide, tirzepatide, and retatrutide are prescription medications in most jurisdictions and carry documented risks that require medical supervision. Any decision about dosing, discontinuation, or off-label use should be made with a clinician who can monitor outcomes and adjust accordingly. Nothing here endorses the practice of microdosing or self-managing these compounds outside the regulatory framework in your country.