At a glance
- Mounjaro is diabetes tirzepatide; Wegovy is obesity semaglutide, so the brands are not a fair match
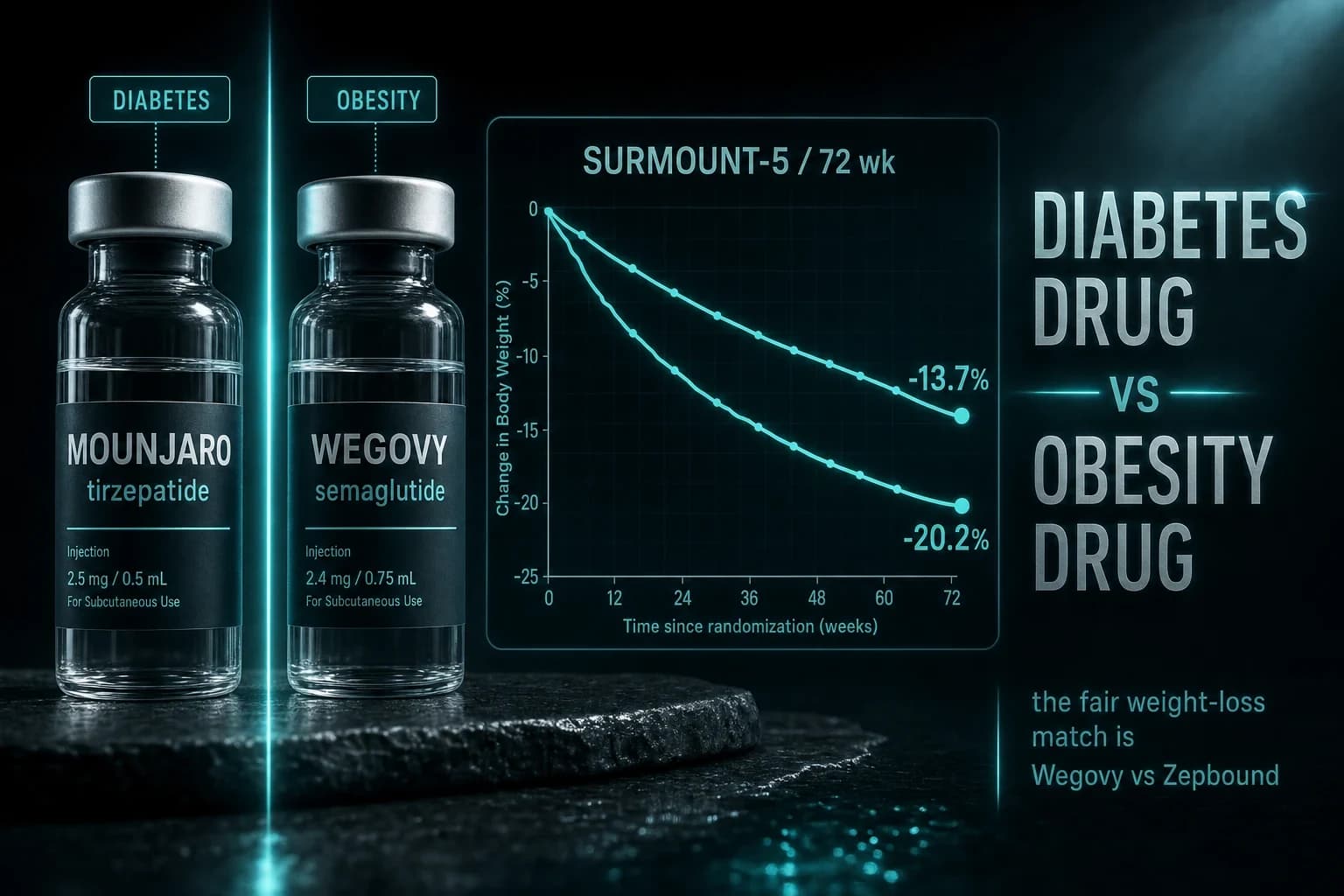
- In SURMOUNT-5, tirzepatide beat semaglutide 20.2% vs 13.7% body-weight loss head to head
- SURPASS-2 gave tirzepatide 15 mg a 12.4 kg drop vs 6.2 kg for semaglutide 1 mg in diabetes
- Semaglutide owns the cardiovascular pedigree: SELECT cut major events 20% (HR 0.80)
- Max doses differ: Mounjaro tops out at 15 mg weekly, Wegovy at 2.4 mg weekly
Here is the catch nobody tells you before you type "Mounjaro vs Wegovy" into a search bar: you are comparing a diabetes drug to a weight-loss drug. Mounjaro is approved to treat type 2 diabetes. Wegovy is approved to treat obesity. They are not the same class competing for the same job, and lining them up as if they were is how people end up asking their doctor for the wrong prescription.
The molecule question underneath, though, is the one you actually care about: tirzepatide or semaglutide, which takes off more weight? That one has a clean answer now. In the first trial to test them directly against each other for obesity, tirzepatide cut 20.2% of body weight versus 13.7% for semaglutide at 72 weeks (Aronne et al. 2025). Same trial, same patients, same timeline. Tirzepatide won by roughly six and a half percentage points.
So the short version is: the brands are mismatched, but the molecule verdict is real. Let me untangle both, because the branding confusion is genuinely the thing tripping most people up.
The brand trap: four names, two molecules
There are only two drugs here. There are four brand names because each manufacturer sells the same molecule twice, once for diabetes and once for weight.
- Mounjaro = tirzepatide, made by Eli Lilly, FDA-approved for type 2 diabetes.
- Zepbound = the exact same tirzepatide, same molecule, FDA-approved for obesity and weight management.
- Ozempic = semaglutide, made by Novo Nordisk, FDA-approved for type 2 diabetes.
- Wegovy = the exact same semaglutide, FDA-approved for obesity and weight management.
Read that again and the "Mounjaro vs Wegovy" matchup falls apart. You are pitting Lilly's diabetes drug against Novo's obesity drug. The apples-to-apples pairs are different: for diabetes it is Ozempic vs Mounjaro, and for weight loss it is Wegovy vs Zepbound. If you want weight loss, the honest comparison is Wegovy against Zepbound, not against Mounjaro.
Why does the molecule get two names? Regulatory and pricing reasons, mostly. A drug approved for diabetes and a drug approved for obesity go through separate FDA indications, separate labels, separate insurance codes, and often separate pricing. Selling tirzepatide as "Mounjaro" to endocrinologists and "Zepbound" to obesity clinics keeps those lanes clean. The chemistry in the pen is identical.
None of that changes the pharmacology. So for the rest of this, when the branding stops mattering, we will talk about tirzepatide (the Mounjaro/Zepbound molecule) and semaglutide (the Ozempic/Wegovy molecule).
Mounjaro vs Wegovy at a glance
| Feature | Mounjaro (tirzepatide) | Wegovy (semaglutide) |
|---|---|---|
| Molecule | Tirzepatide | Semaglutide |
| Maker | Eli Lilly | Novo Nordisk |
| FDA-approved use | Type 2 diabetes | Obesity / weight management |
| Obesity-branded twin | Zepbound | (Wegovy is the obesity brand) |
| Diabetes-branded twin | (Mounjaro is the diabetes brand) | Ozempic |
| Mechanism | Dual GIP + GLP-1 receptor agonist | GLP-1 receptor agonist only |
| Max dose | 15 mg once weekly | 2.4 mg once weekly |
| Avg weight loss (pivotal) | 20.9% at 72 wk (SURMOUNT-1) | 14.9% at 68 wk (STEP 1) |
| Head-to-head weight (obesity) | 20.2% (SURMOUNT-5) | 13.7% (SURMOUNT-5) |
| Cardiovascular outcomes | Trial ongoing (SURPASS-CVOT) | 20% MACE reduction (SELECT) |
| Dosing | Weekly, titrate 2.5 to 15 mg | Weekly, titrate 0.25 to 2.4 mg |
One receptor versus two
This is the mechanistic difference that drives everything downstream.
Semaglutide is a GLP-1 receptor agonist. It mimics one gut hormone, GLP-1, which prompts glucose-dependent insulin release, suppresses glucagon, slows stomach emptying, and quiets appetite in the brain. It does that job very well, which is why it reset the field when Wegovy launched.
Tirzepatide hits two receptors. It agonizes GLP-1 and GIP (glucose-dependent insulinotropic polypeptide), a second incretin hormone. GIP appears to add its own effects on insulin sensitivity and fat metabolism, and the two signals together seem to do more than GLP-1 alone. That is the leading explanation for why tirzepatide tends to out-lose semaglutide on the scale. It is a dual agonist against a single agonist.
Whether the second receptor is the whole story is still debated. What is not debated is the outcome data, so let us go to the trials.
The weight-loss verdict: tirzepatide wins
For years the comparison was indirect. Tirzepatide's SURMOUNT-1 put up 20.9% mean body-weight loss on the 15 mg dose at 72 weeks in adults with obesity and no diabetes (Jastreboff et al. 2022). Semaglutide's STEP 1 put up 14.9% at 68 weeks on the 2.4 mg dose in a comparable population (Wilding et al. 2021). Different trials, different timelines, so purists could argue the gap was an artifact.
SURMOUNT-5 closed that argument. It randomized adults with obesity (without diabetes) directly to tirzepatide or semaglutide, both titrated to their maximum tolerated dose, and ran for 72 weeks. Tirzepatide produced 20.2% mean body-weight reduction versus 13.7% for semaglutide (Aronne et al. 2025). That is a 6.5 percentage-point advantage, head to head, and it lines up almost exactly with what the separate trials predicted.
Bottom line: If maximum weight loss is the goal, tirzepatide beats semaglutide. This is not extrapolation across trials anymore. SURMOUNT-5 tested the two molecules against each other and tirzepatide won by roughly six and a half points of body weight.
The diabetes data tells the same story from a different angle. SURPASS-2 pitted tirzepatide against semaglutide 1 mg in adults with type 2 diabetes. Tirzepatide 15 mg dropped HbA1c 2.30% and body weight 12.4 kg; semaglutide 1 mg dropped HbA1c 1.86% and weight 6.2 kg (Frias et al. 2021). Note the caveat: that trial used semaglutide 1 mg, the diabetes dose, not the 2.4 mg obesity dose, so the weight gap looks wider than it would against Wegovy-strength semaglutide. Still, on blood sugar and weight in diabetes, tirzepatide came out ahead.
Where semaglutide still wins: the heart
If tirzepatide takes the weight crown, semaglutide holds the one credential that matters most to a cardiologist: proven cardiovascular outcomes.
The SELECT trial enrolled more than 17,000 adults who had established cardiovascular disease and were overweight or obese, but did not have diabetes. Semaglutide 2.4 mg cut major adverse cardiovascular events (cardiovascular death, non-fatal heart attack, non-fatal stroke) by 20% versus placebo (HR 0.80, 95% CI 0.72 to 0.90) over a mean 33 months (Lincoff et al. 2023). That was the first time a weight-management drug demonstrated it prevents heart attacks and strokes, and it is why semaglutide carries an FDA indication to reduce cardiovascular risk that tirzepatide does not yet have.
Tirzepatide's cardiovascular outcomes trial, SURPASS-CVOT, is still running. Its metabolic profile is excellent and the expectation is favorable, but as of now the hard-outcomes evidence belongs to semaglutide. If your primary concern is documented protection against cardiovascular events, that pedigree is real and it belongs to the Wegovy molecule.
Warning: More weight loss is not automatically more heart protection. Tirzepatide takes off more pounds, but only semaglutide has finished a cardiovascular outcomes trial and proven it lowers heart-attack and stroke risk. Those are two different questions. Answer the one that matches your health, not the one with the bigger headline number.
So which one, actually?
Strip out the branding and it comes down to what you are treating.
If the priority is weight loss, tirzepatide is the stronger molecule. SURMOUNT-5 settled that head to head. In brand terms, that means Zepbound (obesity tirzepatide), not Mounjaro, is the fair comparison against Wegovy, and it wins on the scale.
If the priority is type 2 diabetes with cardiovascular disease, semaglutide's SELECT outcomes and its established heart-risk indication carry real weight. Tirzepatide controls glucose beautifully, but the finished CV-outcomes evidence sits with semaglutide today.
If you are weighing this seriously, our tirzepatide vs semaglutide 2026 breakdown goes deeper on dosing, side effects, and cost per pound lost. Both molecules share the same gastrointestinal side-effect profile (nausea, diarrhea, constipation), both titrate slowly to blunt it, and both are once-weekly injections.
The cost and access reality
Both drugs are expensive at brand pricing. Mounjaro, Zepbound, Ozempic, and Wegovy all carry list prices around 1,000 dollars or more per month, and what you actually pay hinges on insurance, whether you qualify under the diabetes or the obesity indication, and manufacturer coupons. That indication split is exactly why the brand confusion has teeth: an insurer may cover Mounjaro for diagnosed diabetes but deny Wegovy for weight, or the reverse.
The route most cost-conscious readers land on is supervised telehealth with compounded GLP-1. You complete an online intake, a US-licensed clinician reviews your history and eligibility, and if it is appropriate a compounding pharmacy fills the prescription and ships it to your door. Yucca Health runs this model for both molecules, so it works whether you want the compounded tirzepatide route or compounded semaglutide, with real titration guidance instead of a marketplace checkout. We rank every legitimate access method by real per-month cost in the cheapest GLP-1 guide.
The smart first move is a conversation with a clinician who can screen you, confirm which molecule fits your actual diagnosis, and titrate you safely. Whether that ends in tirzepatide or semaglutide, supervised care beats guessing which brand your search engine served you.
Disclaimer
This article is for research and educational purposes only and is not medical advice. Mounjaro, Zepbound, Ozempic, and Wegovy are prescription medications; tirzepatide and semaglutide are prescription drugs. Decisions about starting, switching, or dosing any of them, including which indication applies to you, should be made with a licensed clinician. Nothing here is a recommendation to self-prescribe or self-administer any compound.


