At a glance
- ASA's 2023 guidance: hold weekly GLP-1s for one week, daily forms the day of surgery
- Sherwin 2023 found 70% of semaglutide users had retained gastric solids vs 10% of controls
- Hiramoto 2024 meta-analysis pinned the average gastric-emptying delay at about 36 minutes
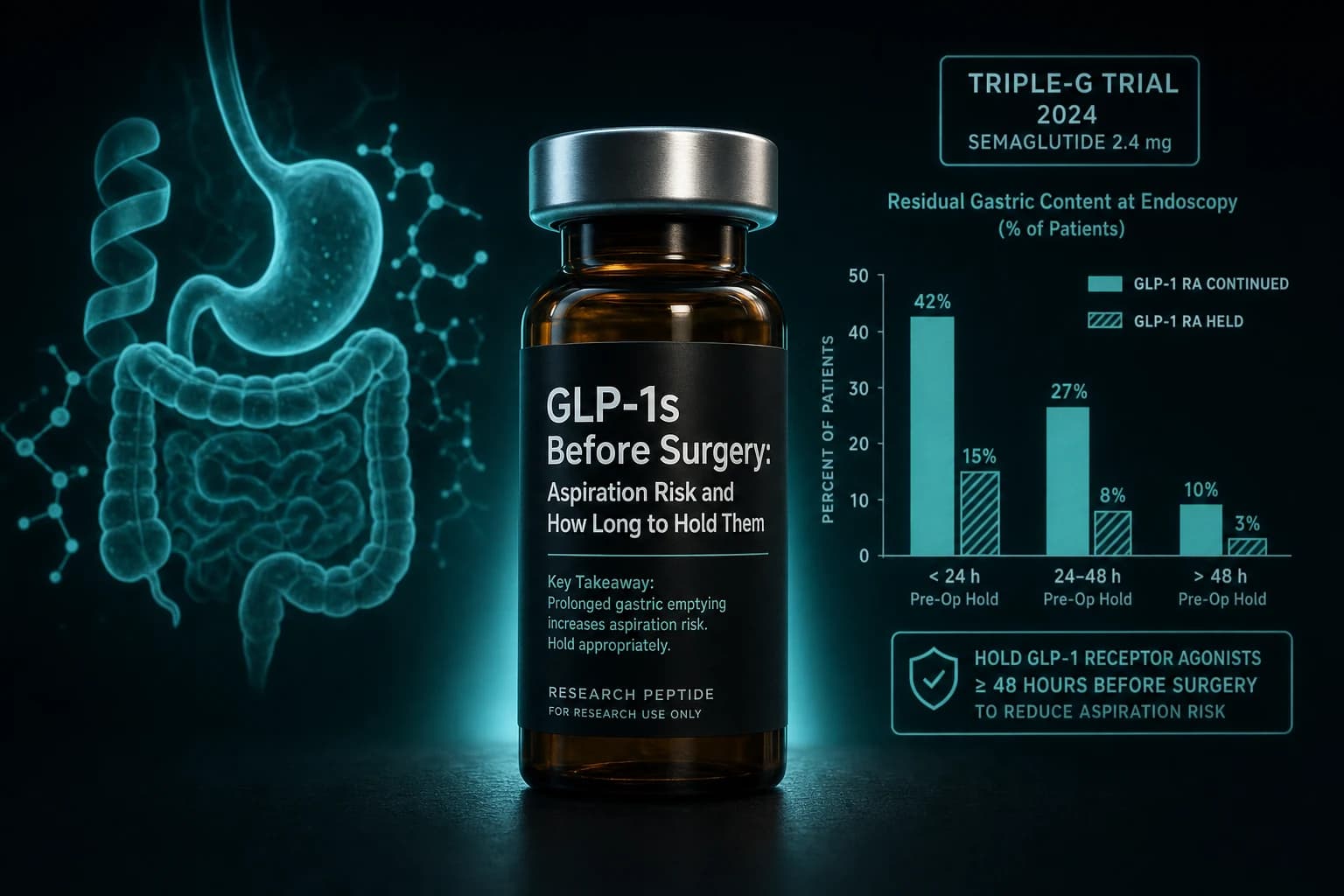
- Nersessian 2024 found residual gastric content in 40% of recent semaglutide users vs 3%
- 2024 multisociety guidance shifted toward shared decisions and a clear-liquid day before
You booked the colonoscopy, fasted overnight, and showed up with an empty stomach. Then the anesthesiologist asks one question that can push the procedure to another day: are you taking Ozempic? GLP-1 receptor agonists slow how fast the stomach empties, and a stomach that still holds food after a proper fast can be aspirated under sedation.
Delayed gastric emptying sits behind every perioperative GLP-1 headline since 2023. The awkward part is that the studies disagree with each other. Some find retained food in the stomach of most semaglutide users after an overnight fast. A large meta-analysis puts the average emptying delay at roughly half an hour, small enough to question the alarm. Both numbers come from real data, and the official guidance has already been rewritten twice trying to reconcile them.
What follows is the part most search results skip: what the studies actually measured, how long the major guidelines suggest holding each GLP-1 before surgery, and why a flat one-week pause does not settle the question.
Why a slow stomach becomes an anesthesia problem
Anesthesia care is built on a simple assumption. Follow the fasting rules (broadly, no solids for six hours and no clear liquids for two before sedation), and the stomach will be close to empty when the airway reflexes that normally protect the lungs are switched off. An empty stomach has little to regurgitate. A full one can send gastric contents up the esophagus and into the lungs, a complication called pulmonary aspiration that ranges from a chemical pneumonitis to a life-threatening event.
GLP-1 receptor agonists complicate that assumption. The same mechanism that curbs appetite, slowed gastric emptying driven by vagal and central signaling, also keeps solid food in the stomach longer than the fasting window assumes. Pulmonary aspiration during anesthesia is rare to begin with, so the practical question is not whether these drugs are dangerous in surgery. It is whether they leave enough retained food, often enough, to matter for an individual patient.
What the studies actually found
The evidence falls into two groups: imaging studies that look directly at stomach contents after a fast, and physiology studies that measure how quickly a test meal leaves the stomach. They point in different directions.
| Study | Design | Population | Key finding |
|---|---|---|---|
| Sherwin et al. 2023 (Can J Anesth) | Prospective, gastric ultrasound | ~20 volunteers, semaglutide vs control | 70% vs 10% had retained solids supine; 90% vs 20% lateral |
| Nersessian et al. 2024 (Anaesthesia) | Prospective observational | 220 surgical patients | Residual gastric content in 40% of recent semaglutide users vs 3% |
| Retrospective EGD analysis 2025 (Endosc Int Open) | Retrospective case-control | Upper-endoscopy patients | Retained contents in 12.5% on GLP-1 vs 1.3% of controls |
| Hiramoto et al. 2024 (Am J Gastroenterol) | Meta-analysis, 15 studies | Mixed | Scintigraphy delay ~36 min; acetaminophen-test studies showed none |
| Dixit et al. 2024 (JAMA) | Retrospective cohort | Surgical patients with diabetes | Postoperative respiratory complications 3.5% vs 4.0% (not significant) |
Imaging tells a consistent story. In a small prospective ultrasound study, Sherwin et al. (2023) found that 70% of volunteers on semaglutide still had solid gastric content while supine after fasting, against 10% of controls. Nersessian et al. (2024) scanned 220 surgical patients and saw residual gastric content in 40% of those who had taken semaglutide within the prior 10 days, compared with 3% of non-users. A 2025 retrospective of upper-endoscopy patients reported retained contents in 12.5% of GLP-1 users versus 1.3% of controls (retrospective EGD analysis, 2025). Different methods, same direction: more food, more often, in people on these drugs.
Physiology pushes back. The meta-analysis by Hiramoto et al. (2024) pooled 15 studies and found that the average gastric-emptying delay measured by scintigraphy was about 36 minutes (95% CI 17 to 55), while studies using the acetaminophen-absorption test found no significant delay at all. Set against a six-to-eight-hour solid fast, 36 minutes is modest. The authors argued that the routine recommendation to hold these drugs rested on thin evidence.
Outcome data complicate it further. The largest relevant cohort, Dixit et al. (2024) in JAMA, looked at postoperative respiratory complications in surgical patients with diabetes and found 3.5% among GLP-1 users versus 4.0% among non-users (odds ratio 0.85, 95% CI 0.70 to 1.04), a difference that was not statistically significant. Retained food on a scan is a surrogate. Whether it converts into actual aspiration in the operating room is the question the outcome data have not answered with confidence.
Bottom line: Imaging studies agree that GLP-1 users are more likely to have food in the stomach after fasting. Physiology and early outcome data suggest the average emptying delay is small and have not yet shown more respiratory complications. The risk is real but probably smaller and more variable than the scariest headlines imply.
How long to hold each GLP-1 before a procedure
The suggested pause tracks two things: how often the drug is dosed and how long it lingers in the body. Weekly injectables with long half-lives get a longer hold than daily forms that clear quickly. The table below reflects the 2023 consensus framework from the American Society of Anesthesiologists. Read it as a starting point for a conversation with your care team, not a self-service instruction.
| Drug (brand) | Dosing | Typical hold (2023 ASA framework) | Notes |
|---|---|---|---|
| Semaglutide (Ozempic, Wegovy) | Weekly injection | About one week before | Half-life near 7 days; symptomatic patients may need longer |
| Oral semaglutide (Rybelsus) | Daily | Day of the procedure | Daily dosing despite a long half-life |
| Tirzepatide (Mounjaro, Zepbound) | Weekly injection | About one week before | Half-life near 5 days; less direct aspiration data than semaglutide |
| Dulaglutide (Trulicity) | Weekly injection | About one week before | Long-acting weekly agent |
| Liraglutide (Victoza, Saxenda) | Daily injection | Day of the procedure | Short half-life near 13 hours |
| Retatrutide (investigational) | Weekly injection | No procedural data | Not approved; any pause is extrapolated from class behavior |
Newer GLP-1 and dual or triple agonists share the same gastric-emptying mechanism, so their hold windows are estimated from pharmacokinetics rather than proven by surgery studies. If you are tracking how these compounds differ in dosing and duration, the GLP-1 dosing comparison for 2026 lays out the schedules side by side, and the semaglutide and tirzepatide compound guides cover their pharmacology.
Why "hold it for a week" is not a clean rule
A single week sounds tidy. The data are messier. A retrospective single-center analysis of various semaglutide interruption intervals (2024) found that pausing for less than 14 days was still associated with increased residual gastric content, and only intervals beyond roughly three weeks brought users in line with non-users. Patients with ongoing digestive symptoms needed the longest pause.
Two practical points follow. The effect on emptying tends to fade with chronic use, so someone stable on a maintenance dose for months may retain less than someone recently started or escalated. And because the delay hits solids far harder than liquids, a clear-liquid diet the day before a procedure can lower residual content even when the drug itself is continued. That second point is why the guidance moved away from reflexive cancellation.
Warning: Do not stop a prescribed GLP-1 on your own before a procedure. For type 2 diabetes the drug is managing blood sugar, and skipping doses carries its own risk. Tell your prescriber and your anesthesia or endoscopy team, and let them decide together based on your dose, symptoms, and the procedure.
The guidance has been rewritten twice
In June 2023 the American Society of Anesthesiologists issued consensus guidance recommending that daily-dosed GLP-1s be held on the day of a procedure and weekly agents held for a week, alongside standard fasting. It was cautious by design, and it triggered a wave of canceled and delayed cases.
By late 2024 the picture had widened. A multisociety clinical practice guidance (Kindel et al., 2024), developed across gastroenterology, bariatric surgery, and anesthesiology groups, recommended shared decision-making rather than blanket holding. Its themes: stratify by risk (GI symptoms, recent dose escalation), favor a clear-liquid diet the day before, use point-of-care gastric ultrasound when feasible to check the stomach directly, and weigh the metabolic cost of stopping against a small and uncertain aspiration risk. Into 2025, international groups echoed the same individualized approach.
Note: Almost all of this evidence sits in semaglutide. Tirzepatide and retatrutide work through the same delayed-emptying mechanism, but direct perioperative studies on them are sparse, so their hold windows lean on pharmacokinetics rather than procedure data.
What this means if you are on a GLP-1
The reflexive advice ("just stop it for a week") and the dismissive take ("the delay is only 36 minutes") both miss the point. Risk here is individual, and the people best placed to judge it have access to your dose history, your symptoms, and the type of anesthesia planned. A few things are worth doing regardless.
Tell every part of the care team that you take a GLP-1, including the scheduler, the surgeon or endoscopist, and the anesthesia provider. Ask directly whether to hold the drug and for how long given your situation, rather than assuming the front-desk default is right for you. Expect a possible clear-liquid day before the procedure even if you are told to continue the medication. And if you take it for type 2 diabetes, ask how to manage glucose during any pause, because stopping is not free.
If you are researching these compounds outside the clinic, the semaglutide and tirzepatide guides cover pharmacology and sourcing, and vials for protocol work are available through Ascension Peptides with code ENHANCED for 50% off injectables. None of that changes the rule above: a perioperative decision belongs with your clinical team, not a checkout page.
Further reading
- Semaglutide compound guide
- Tirzepatide compound guide
- GLP-1 dosing comparison 2026
- Stopping GLP-1s: weight regain and maintenance research
- Semaglutide reconstitution chart
- Reconstitution calculator
This article is for educational and research purposes only. It is not medical advice and does not replace guidance from your prescriber, surgeon, or anesthesia provider. Semaglutide and tirzepatide are FDA approved for type 2 diabetes and chronic weight management; retatrutide is investigational and not approved. Do not start, stop, or change any prescribed medication before a procedure without talking to your clinical team.