At a glance
- Hurtado 2024 Menopause journal (PMID 38446869): 106 postmenopausal women on semaglutide, hormone therapy users lost 16% at 12 months vs 12% without HT
- Castaneda 2026 Mayo Clinic cohort (Lancet OG&WH): 120 postmenopausal women on tirzepatide, HT users lost 19.2% vs 14.0% at last follow-up (p=0.0023)
- Tchang 2025 SURMOUNT post-hoc (PMID 40074721): tirzepatide worked 23 to 26% vs 2 to 3% placebo across pre-, peri-, and postmenopause, so menopause itself does not blunt response
- Both HT-combo studies were retrospective and non-randomized; healthy-user bias and unmeasured lifestyle differences are the main confounders to weigh
- Bone loss and fragility fracture risk are the two safety questions that remain open in the 55 to 75 age band on GLP-1 weight loss doses
Weight loss on semaglutide or tirzepatide runs at 15 to 21 percent of body weight across the pivotal obesity trials. What the pivotal trials do not answer well is a question that comes up in every women's health clinic: does the same drug work the same way in a 58-year-old on hormone replacement as it does in a 38-year-old who is not?
Three publications from the last 18 months finally have real numbers on this. A retrospective cohort by Mayo Clinic's Maria Hurtado published in Menopause in April 2024 (PMID 38446869) tracked postmenopausal women on semaglutide, split by hormone therapy use. A follow-up cohort from the same Mayo group led by Regina Castaneda ran the same design on tirzepatide, published in The Lancet Obstetrics, Gynaecology, & Women's Health in January 2026. And a post hoc analysis of the SURMOUNT program by Beverly Tchang and colleagues in Obesity in 2025 (PMID 40074721) categorized SURMOUNT women by reproductive stage and asked a different question: does the response even depend on menopause status.
This article walks through what each of those studies actually measured, how big the effect sizes are, where the confounders sit, what the mechanism story looks like, and where the evidence is still thin. Treat it as a reference for reading the emerging HRT-plus-GLP-1 numbers before making a joint decision with a prescriber. Nothing here is a treatment guide or a substitute for individualized clinical advice.
Why menopause changes the weight-loss calculation
The metabolic shift at menopause is not a small effect. Resting metabolic rate drops, fat distribution moves from gluteofemoral to visceral, and lean body mass declines even without a change in weight. The perimenopausal transition itself is associated with roughly 1.5 kg of average weight gain independent of aging, and abdominal fat mass increases by about 20 percent across the transition on top of that. Estrogen loss is the single largest lever.
Estrogen also does something else that matters here. It amplifies GLP-1 receptor signaling in animal models and appears to potentiate the anorectic effect of GLP-1 in the hypothalamus. The preclinical work is consistent with a modest mechanistic interaction: when estrogen is present, GLP-1 agonism produces a slightly stronger downstream effect on food intake and body weight. When estrogen is absent, that potentiation is lost.
That is the biological reason to ask whether adding hormone therapy back to a postmenopausal woman on semaglutide or tirzepatide restores some of the response. The clinical evidence is where the retrospective cohorts come in.
The Hurtado 2024 semaglutide + HT cohort
The Hurtado et al. 2024 study in Menopause is the anchor paper for the semaglutide question. Design: retrospective cohort of 106 postmenopausal women treated with semaglutide for overweight or obesity for at least three months at Mayo Clinic between January 2021 and March 2023. Mean age 58.4 years. Mean baseline BMI 38.5. Comparison: current menopause hormone therapy users versus non-users, adjusted for age, baseline BMI, and comorbidities.
Total body weight loss percentage (TBWL%) diverged consistently in favor of the HT-plus-semaglutide arm:
| Timepoint | HT + semaglutide TBWL% | Semaglutide alone TBWL% |
|---|---|---|
| 3 months | 7 ± 3 | 5 ± 4 |
| 6 months | 13 ± 6 | 9 ± 5 |
| 9 months | 15 ± 6 | 10 ± 6 |
| 12 months | 16 ± 6 | 12 ± 8 |
The 12-month difference of 4 percentage points sounds small in the abstract. In context, it is not. Four extra percentage points of body weight in an average 100 kg starting weight is 4 kg of additional fat mass loss over a year. The association held after adjustment for confounders in the paper's multivariable model.
Where the study has limits. It is retrospective, not randomized. Women choosing HT differ systematically from women not choosing HT: they are more likely to have vasomotor symptoms severe enough to seek treatment, more likely to be engaged with a menopause-specialty clinic, and more likely to be engaged in other lifestyle interventions. The paper controlled for measured confounders. It could not control for the unmeasured ones. The cohort is also drawn from a single tertiary center, which biases the population toward higher motivation and better follow-up than the general population.
The takeaway is not that HT causes the additional weight loss. The takeaway is that in a real-world clinical cohort, the two treatments together tracked with more weight loss than semaglutide alone, and the effect size is consistent with the preclinical estrogen-plus-GLP-1 potentiation story.
The Castaneda 2026 tirzepatide + HT cohort
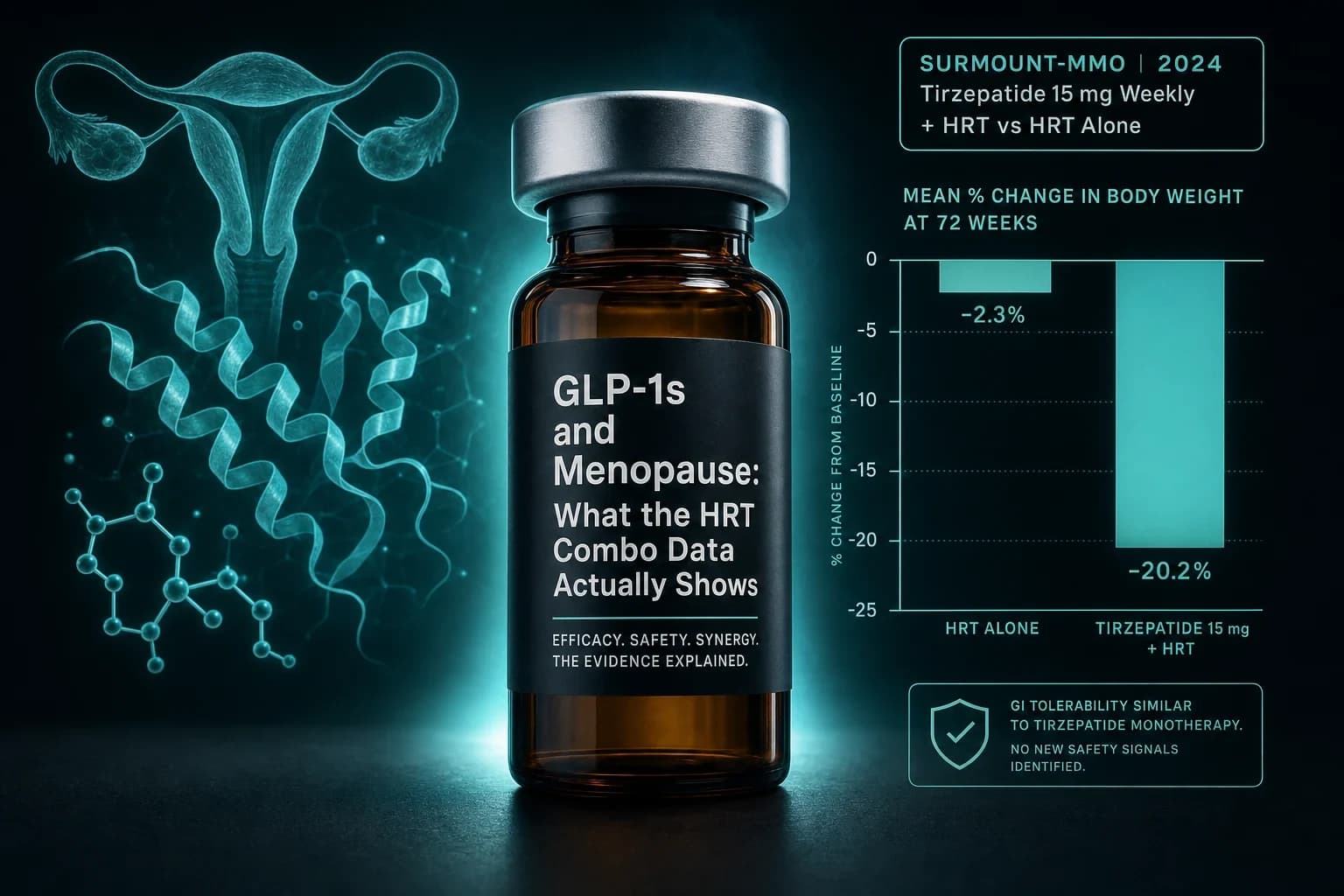
Two years after the Hurtado paper, the same Mayo Clinic obesity group ran the analogous study on tirzepatide. Castaneda et al., published in The Lancet Obstetrics, Gynaecology, & Women's Health on January 22, 2026 (DOI 10.1016/S3050-5038(25)00145-1). Design: retrospective cohort of 120 postmenopausal women prescribed tirzepatide for weight management and followed for a median of 18 months. 40 women were on concurrent menopause hormone therapy, matched 1:2 to 80 women on tirzepatide alone.
Primary outcome: percentage change in total body weight at last follow-up.
| Endpoint | HT + tirzepatide | Tirzepatide alone | p-value |
|---|---|---|---|
| Total body weight loss at last follow-up | −19.2% | −14.0% | 0.0023 |
| Proportion achieving ≥20% weight loss | 45% | 18% | reported significant |
| Direction on cardiometabolic parameters | Improved further | Baseline improvement | favorable |
The 5.2 percentage-point delta on tirzepatide is larger than the 4-point delta on semaglutide from Hurtado. That is directionally consistent with tirzepatide producing larger absolute weight loss overall, so a proportional interaction with hormone therapy would be expected to be larger in the arm that is producing more mechanistic effect to modulate.
The 45 percent versus 18 percent split on the ≥20 percent threshold is the number that translates most clearly to clinical decision-making. Twenty percent body weight loss is roughly the boundary where NAFLD reversal, remission of obstructive sleep apnea, and durable diabetes improvement start to become likely rather than possible. Nearly half of the HT-plus-tirzepatide group crossed that line. Fewer than one in five of the tirzepatide-alone group did.
Same limitations as the semaglutide cohort. Retrospective, single center, matched but not randomized. Women on HT were more likely to be engaged with menopause specialty care and less likely to have poorly managed comorbid conditions at baseline. The Castaneda paper's authors flag this explicitly and note that the direction is consistent with a real biological interaction but cannot prove causation without a randomized trial.
The Tchang SURMOUNT reproductive-stage analysis
Where the retrospective cohorts asked "does HT augment the response," the Tchang et al. 2025 Obesity post hoc analysis of the SURMOUNT program asked a prior question: does reproductive stage itself alter how well tirzepatide works. If menopause blunts the response, the Hurtado and Castaneda observations would take on a different interpretation, because the "HT" arm would partly be recovering ground the menopause lost.
Design: women participants from SURMOUNT-1, -3, and -4 were retrospectively classified by reproductive stage (premenopause, perimenopause, postmenopause) and body weight change on tirzepatide 15 mg or maximum tolerated dose was compared against placebo.
Body weight reduction from baseline at week 72:
| Reproductive stage | Tirzepatide TBWL% | Placebo TBWL% |
|---|---|---|
| Premenopause | −26% | −2% |
| Perimenopause | −23% | −3% |
| Postmenopause | −23% | −3% |
The proportion achieving ≥5 percent weight loss ranged from 97 to 98 percent on tirzepatide versus 29 to 33 percent on placebo across all three stages. Waist circumference reductions were 22, 20, and 20 cm respectively.
Menopause status does not appear to blunt tirzepatide's efficacy in the randomized SURMOUNT population. The absolute effect sizes are 2 to 3 percentage points smaller in peri- and postmenopause than in premenopause, which is a small enough gap to plausibly reflect confounding by age, BMI, or comorbidities within the SURMOUNT enrollment. The direction is not "tirzepatide works dramatically less well after menopause." The direction is "tirzepatide works similarly well across the reproductive spectrum, with a modest attenuation in the postmenopausal window."
This matters for interpretation. If the Castaneda +5.2 percentage point HT effect is real, it is likely additive potentiation on top of a response that is already close to maximal, not recovery of a lost response.
Study comparison at a glance
The three anchor studies map cleanly onto a comparison table.
| Study | Drug | Design | n | Median follow-up | HT + drug outcome | Drug alone outcome | Delta |
|---|---|---|---|---|---|---|---|
| Hurtado 2024 (PMID 38446869) | Semaglutide | Retrospective cohort | 106 | 12 months | −16% | −12% | +4 pp |
| Castaneda 2026 | Tirzepatide | Retrospective cohort, matched | 120 | 18 months | −19.2% | −14.0% | +5.2 pp |
| Tchang 2025 (PMID 40074721) | Tirzepatide | Post hoc RCT (SURMOUNT) | Women only from SURMOUNT-1/-3/-4 | 72 weeks | n/a (not stratified by HT) | Post: −23%, Peri: −23%, Pre: −26% vs placebo −2 to −3% | Menopause status: 2 to 3 pp attenuation |
Two things fall out. First, both retrospective cohorts report an additive benefit of HT plus GLP-1 in the 4 to 5 percentage point range. Second, the underlying tirzepatide response holds up well across reproductive stages, so the HT signal is on top of a still-strong response, not a rescue effect.
The 2026 Cureus scoping review by Graczyk and Bisschops is the most recent synthesis across these and related studies. Their conclusion: GLP-1 receptor agonists are associated with more weight loss and reduced central adiposity in postmenopausal women, with a smaller and less consistent signal on vasomotor symptoms and cardiovascular biomarkers. The review flags the same limits: retrospective evidence, small cohorts, no head-to-head RCT of HT plus GLP-1 versus GLP-1 alone.
Mechanism: why estrogen and GLP-1 might reinforce each other
The mechanistic story sits at two levels.
At the receptor level, estrogen appears to sensitize hypothalamic GLP-1 signaling. Rodent studies show that ovariectomized animals blunt the anorectic response to peripheral GLP-1 agonism and that estradiol replacement restores the response. Human trials cannot directly measure this, but the direction of the retrospective cohorts is consistent with the animal work.
Whole-body composition changes matter too. Hormone therapy alters the fat distribution that a GLP-1 acts on. Estrogen preserves gluteofemoral fat storage and mitigates the shift toward visceral adiposity that accompanies menopause. That means the fat mass being lost on GLP-1 therapy in an HT user is coming out of a distribution that is closer to premenopausal patterns, with a smaller subcutaneous cushion at the hip and thigh and proportionally more visceral fat to give up. Losing weight from the visceral compartment translates to bigger changes on the scale per unit of body composition change.
Estrogen also modulates energy expenditure directly, both via basal metabolic rate and via activity thermogenesis. HT users tend to sit slightly higher on resting metabolic rate than non-users of the same age and body composition, which produces a small tailwind on the calorie deficit that GLP-1 therapy is driving.
None of these mechanisms is a strong effect on its own. Stacked together, in the same direction, they plausibly produce the 4 to 5 percentage point delta the retrospective cohorts observe.
Bottom line: The additive benefit is biologically plausible, replicated in two retrospective cohorts on two different GLP-1 compounds, and consistent with the SURMOUNT reproductive-stage data. It is not proven by a randomized trial. Anyone comparing HT-plus-GLP-1 to GLP-1 alone should treat the 4 to 5 percentage point delta as a real but confounded estimate, not as a fixed prescription target.
Vasomotor symptoms and quality of life: the softer signal
The retrospective cohorts were designed around weight loss, not around symptom relief. That leaves a real question: does GLP-1 therapy itself do anything for hot flashes, night sweats, or sleep disturbance beyond what any weight loss achieves.
The Graczyk and Bisschops scoping review synthesizes what evidence exists. A small number of studies report reductions in vasomotor symptom frequency and severity on GLP-1 therapy, but the signal is inconsistent and sample sizes are small. Sleep quality improvements are more consistently reported, and are plausibly mediated by weight loss reducing airway obstruction and improving sleep architecture. There is no well-powered randomized trial testing GLP-1 therapy against placebo for vasomotor symptoms specifically.
For anyone reading the popular coverage of this topic, this is the section to bookmark. The headlines that describe GLP-1s as "menopause drugs" or "hot flash relief" are outrunning the evidence. Weight loss helps sleep. Weight loss modestly reduces vasomotor symptom severity across many interventions. GLP-1s produce weight loss. The chain is real. The direct receptor-level effect on menopause symptoms is not established.
The bone density and fragility fracture question
Postmenopausal women are the population where the GLP-1 bone-loss question matters most. The Hansen et al. 2024 phase 2 RCT in eClinicalMedicine enrolled 64 adults at increased fracture risk, mean age 63, mostly postmenopausal women. 52 weeks of semaglutide 1.0 mg produced a 2.6 percent reduction in total hip bone mineral density and a 2.1 percent reduction in lumbar spine BMD compared to placebo. Bone resorption markers (P-CTX) rose. Weight loss was approximately 6.8 kg greater in the semaglutide arm.
The Hansen trial is the cleanest available signal on semaglutide-associated bone changes in the age band that matters. Two important caveats. First, the dose is 1.0 mg (T2D dosing), not the 2.4 mg used for obesity, so the true obesity-dose signal is likely larger. Second, the mechanism appears to be weight-loss-mediated: the amount of BMD change tracks with the amount of weight lost, and no comparable signal is seen with weight loss that preserves lean mass better.
Real-world fracture outcomes on GLP-1s in older adults are still developing. A 2026 retrospective analysis in a large administrative cohort estimated a hazard ratio of approximately 1.26 for fragility fracture in adults aged 65 to 75 initiating GLP-1s versus comparator drugs, with no signal in adults 75 and older. For a deeper dive on the fracture-risk numbers across trials and cohorts, see the GLP-1 bone density and fracture risk research review.
For a postmenopausal woman weighing HT plus GLP-1, the bone density question is where hormone therapy contributes its own trajectory. Estrogen is well established to preserve BMD in the postmenopausal window, and standard HT approximately halves fracture risk over a decade of use. That is the exact opposite direction of the GLP-1 signal. In principle, HT plus a GLP-1 could partly cancel out the bone-loss cost of the weight loss. There is no clean prospective trial testing this. The direction is plausible; the magnitude is not measured.
What this means for a 55-year-old deciding on Wegovy or Zepbound
The practical decision that this evidence informs is not "should I start a GLP-1." That decision belongs upstream, with the standard obesity indication criteria, cardiovascular risk profile, and comorbidity picture. The question this evidence informs is "if I am already on hormone therapy, or considering it, does the joint decision change."
A short framework, without a prescription:
- If you are already on stable HT and considering a GLP-1, the cohort evidence is directionally favorable. Expect the same overall response profile as any other user, with a modest tailwind from the estrogen-GLP-1 interaction. The bone density trajectory looks less concerning than the same drug at the same dose without HT.
- If you are on a GLP-1 already and considering starting HT for menopausal symptoms, the decision belongs primarily on the menopause side (vasomotor symptom burden, individual risk profile, contraindications). The weight-loss augmentation is a small favorable secondary effect, not a primary indication for HT.
- If you are considering both simultaneously, the retrospective cohorts do not answer whether starting them together produces different outcomes than staggered starts. The straightforward path is to stabilize on the treatment addressing the more disruptive symptom first, then add the second.
- If you are postmenopausal and not on HT and not planning to start it, the Tchang SURMOUNT reproductive-stage data says tirzepatide still works well in your subgroup. The absence of HT does not predict a weak response; the practical consequence is to be more attentive to lean mass, bone density, and protein intake during weight loss.
For anyone selecting a specific compound within this decision, the tirzepatide vs semaglutide 2026 head-to-head covers the choice at the compound level, and the Wegovy dosage chart and Zepbound dosage chart walk through the titration schedules. The reconstitution calculator handles the arithmetic for research-use vials.
Warning: Menopause hormone therapy is not indication-approved as a weight loss adjunct. The additive benefit shown in the retrospective cohorts does not by itself justify starting HT. The primary indication for HT is menopausal symptom management in appropriately selected women, and that decision belongs with a menopause-specialty clinician who can weigh individual cardiovascular, thromboembolic, and breast cancer risk.
Where the evidence is still thin
Five gaps deserve to be named out loud rather than glossed.
No randomized trial of HT plus GLP-1 versus GLP-1 alone. The Hurtado and Castaneda cohorts are the best available evidence and they are both retrospective. A properly powered randomized comparison would take three to five years to run and does not exist yet. Every effect size reported here should be treated as a directional estimate, not a fixed prescription target.
No head-to-head across HT modalities. Oral estrogen, transdermal estradiol, combined estrogen-progestin regimens, and vaginal estrogen may not interact identically with GLP-1 signaling. The cohort studies do not stratify by HT modality. Whether transdermal HT augments GLP-1 response more or less than oral is unknown.
No data on GLP-1 pipeline compounds in this population. Retatrutide, cagrilintide-semaglutide (CagriSema), maridebart cafraglutide (MariTide), and orforglipron have no comparable subgroup analyses by menopause status or HT use. The mechanism story that supports the semaglutide-plus-HT effect should generalize, but that is a hypothesis, not a measurement.
No prospective bone density data on the combination. The intuition that HT counteracts GLP-1-mediated BMD loss is biologically supported. It is not measured in a prospective trial.
Sparse data on non-white postmenopausal populations. Both Mayo Clinic cohorts are drawn from a majority-white referral population. Menopausal weight distribution, HT response, and GLP-1 metabolism all have documented ethnic variation. The magnitude of the HT-plus-GLP-1 effect in Black, Hispanic, and Asian postmenopausal populations is not measured.
For readers wanting more on the underlying compounds, the semaglutide peptide page covers pharmacology and label indications, and the tirzepatide peptide page does the same for the dual GLP-1/GIP agonist. Beyond the menopause window, the broader women's health angle is covered in Best peptides for women and GLP-1 PCOS evidence.
Anyone sourcing research-use semaglutide or tirzepatide should note that Ascension Peptides carries both formats with 50% off using code ENHANCED. The Ascension Peptides review covers the COA and third-party testing methodology used on the injectable side.
Bottom line
Two retrospective Mayo Clinic cohorts, one on semaglutide and one on tirzepatide, both report a 4 to 5 percentage point additional total body weight loss in postmenopausal women on hormone therapy versus those not on hormone therapy. A separate SURMOUNT post hoc analysis shows tirzepatide's underlying efficacy holds up across pre-, peri-, and postmenopause, with a modest 2 to 3 percentage point attenuation in the postmenopausal window. Preclinical work on estrogen sensitization of hypothalamic GLP-1 signaling supports a direction of effect. No randomized trial has tested the combination head-to-head against GLP-1 alone.
For a 55-year-old deciding on Wegovy or Zepbound, the practical implication is narrow. If HT is otherwise indicated, the combination looks favorable across weight loss and probably across bone density trajectory. If HT is not otherwise indicated, the retrospective cohort evidence is not by itself a reason to start it. And if HT is contraindicated, the SURMOUNT data still support a strong expected response to tirzepatide in the postmenopausal subgroup, with lean mass and bone density as the two variables to actively manage rather than passively observe.
The larger point is that GLP-1 responses in women are not uniform across the reproductive spectrum, but the direction of variation is smaller than the popular menopause-and-Ozempic coverage sometimes implies. Menopause changes the metabolic starting point. It does not appear to substantially blunt the drug's efficacy. Adding hormone therapy on top, when otherwise indicated, tracks with a small additional benefit that is biologically plausible and consistent across two independent cohorts.
This article is for research and educational purposes only. Menopause hormone therapy and GLP-1 receptor agonists are prescription medications with individualized risk profiles. Decisions about starting, stopping, or combining these therapies belong with a qualified prescriber familiar with your medical history. Statistics cited come from the peer-reviewed publications linked inline. Nothing here constitutes medical advice, and the retrospective cohort evidence discussed is not a substitute for a randomized trial.