At a glance
- SURMOUNT-1 recorded tirzepatide constipation at 16.8, 17.1, and 11.7 percent for 5, 10, and 15 mg (placebo 5.8 percent)
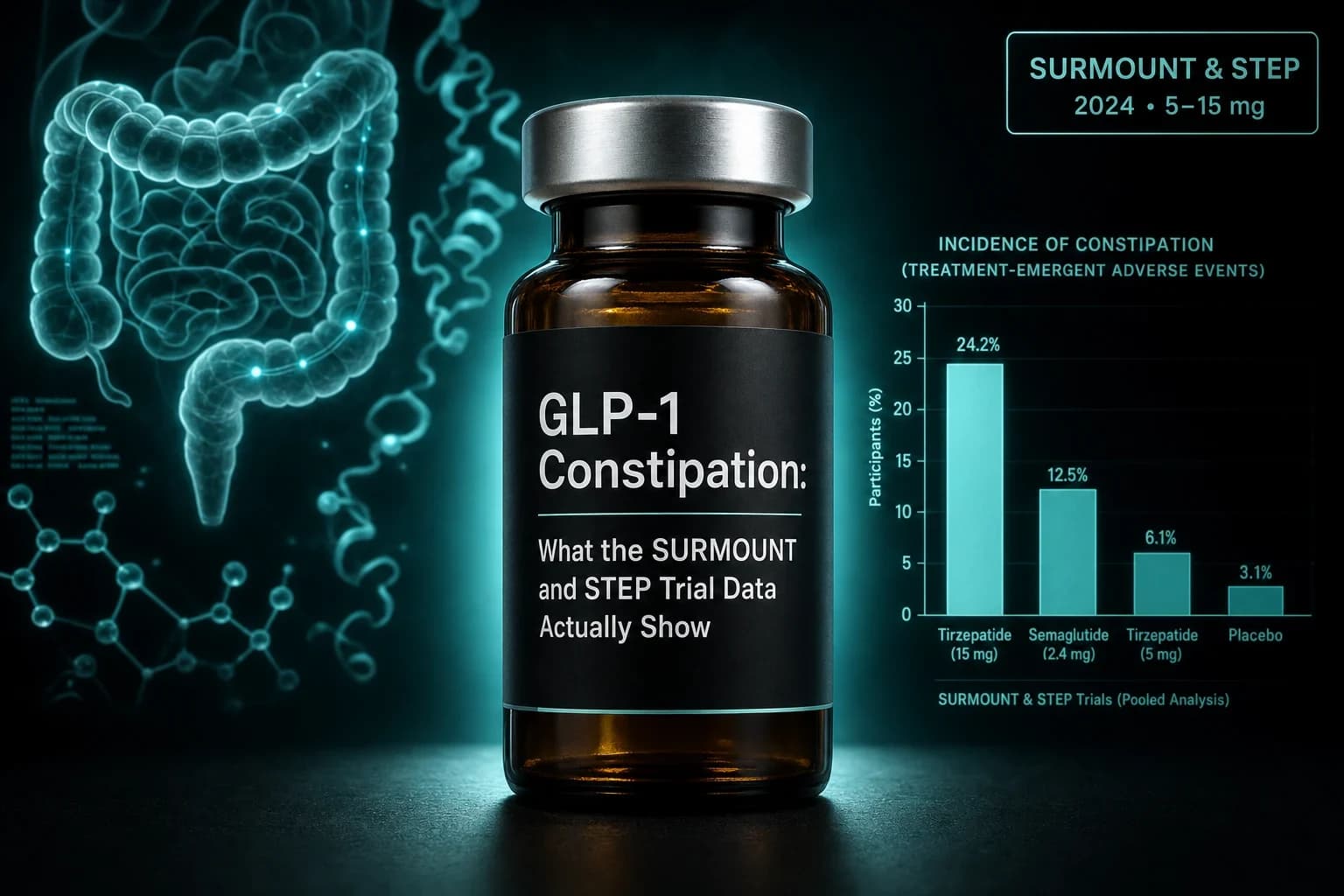
- STEP-1 semaglutide 2.4 mg produced constipation in 24.2 percent versus 11.5 percent on placebo across 68 weeks
- GI events cluster in the first 12 to 20 weeks of titration and taper as the maintenance dose stabilizes (Rubino et al. 2025)
- Mechanism is mechanical: slowed gastric emptying plus longer colon transit means more water reabsorption and harder stool
- Fluid, fiber, and osmotic laxatives are the first line; stimulant laxatives short-term; investigate obstruction if pain plus vomiting appears
Constipation is the second-most-searched GLP-1 side effect after nausea, and it is the one people underestimate the most. Nausea gets a warning label and a titration schedule. Constipation gets a shrug from the prescriber and a link to a fiber supplement. The trial data tell a different story: across the pivotal STEP and SURMOUNT programs, 11 to 24 percent of participants reported constipation, and a smaller but non-trivial subset ended up on chronic laxatives or, in isolated case reports, in the emergency department with obstruction.
This is a research-focused breakdown of what the actual trial data show, why the mechanism produces the symptom, when in a course of therapy it tends to hit, and what the evidence supports for management. It is not medical advice. It is a reference for people who want to know the numbers before they either start a GLP-1 or reason about a symptom they already have.
The rates you should actually expect
Trial-reported constipation rates depend on the compound, the dose, the population, and the definition. The definition matters more than most articles admit. In the STEP and SURMOUNT trials, "constipation" is a spontaneously reported adverse event, not a standardized Rome IV diagnosis. That means the true rate of harder stools, fewer bowel movements, and straining is almost certainly higher than the AE tables suggest, because subclinical constipation gets under-reported when the participant is losing weight and feels the overall trade is worth it.
Here are the pooled trial numbers.
| Drug | Trial | Dose | Constipation, active | Constipation, placebo | Citation |
|---|---|---|---|---|---|
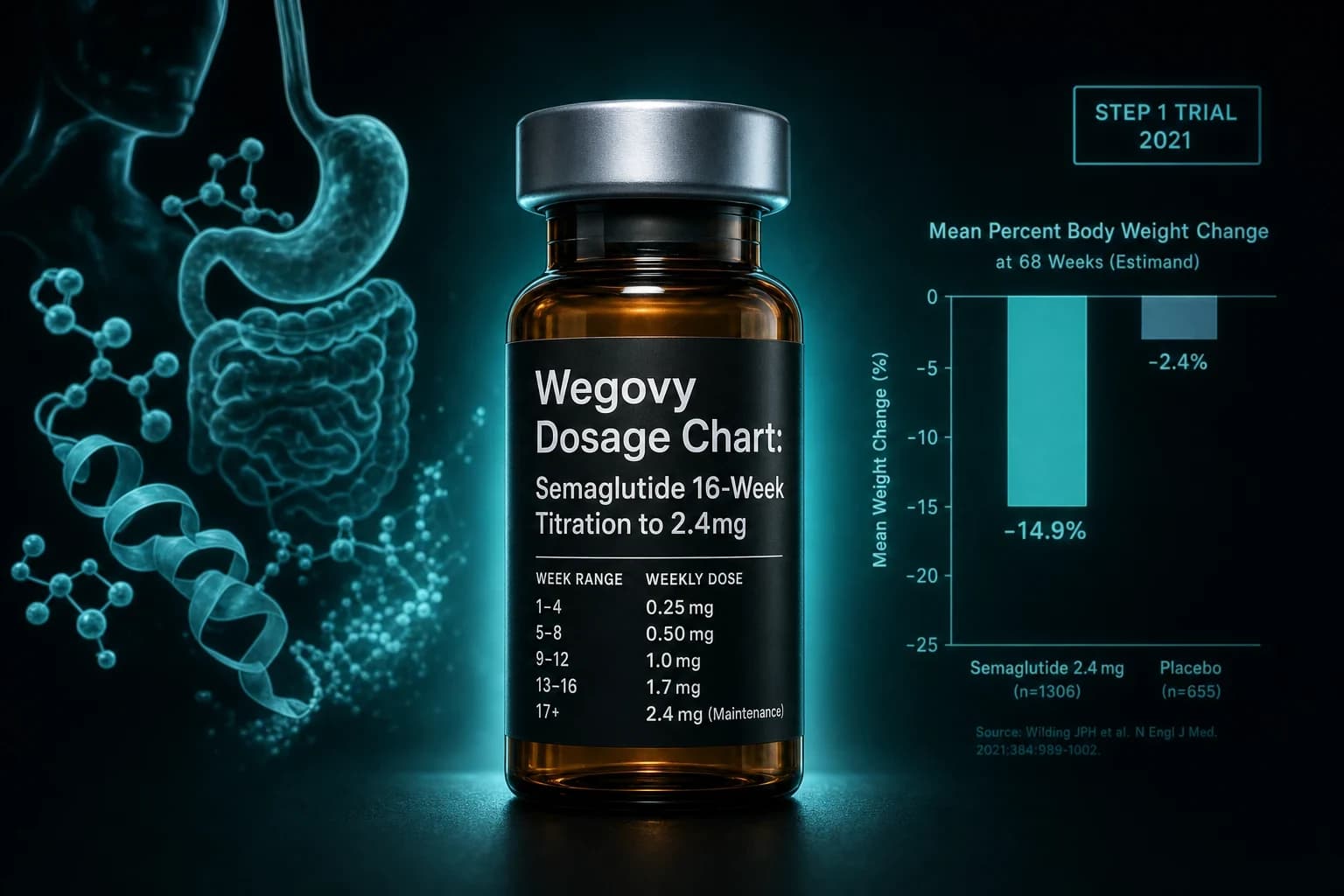
| Semaglutide 2.4 mg | STEP-1, 68 wk, obesity | 2.4 mg weekly | 24.2% | 11.5% | Wilding et al. NEJM 2021 |
| Tirzepatide | SURMOUNT-1, 72 wk, obesity | 5 mg weekly | 16.8% | 5.8% | Jastreboff et al. NEJM 2022 |
| Tirzepatide | SURMOUNT-1, 72 wk, obesity | 10 mg weekly | 17.1% | 5.8% | Jastreboff et al. NEJM 2022 |
| Tirzepatide | SURMOUNT-1, 72 wk, obesity | 15 mg weekly | 11.7% | 5.8% | Jastreboff et al. NEJM 2022 |
| Tirzepatide | SURPASS-2, 40 wk, T2D | 5 to 15 mg weekly | 6.8 to 11.4% | 6.6% (semaglutide 1 mg comparator) | Frías et al. NEJM 2021 |
| Tirzepatide, pooled | SURMOUNT-1 to -4 post hoc | 5 to 15 mg | ~12 to 17% across doses | ~6% | Rubino et al. DOM 2025 |
Three patterns fall out of this table.
First, the obesity trials show more constipation than the diabetes trials. SURMOUNT-1 hit 17 percent at 10 mg; SURPASS-2 hit about 8 percent at 10 mg. Same drug, same dose, different denominator. The most likely explanation is that obesity trials titrate to higher steady-state doses and enroll participants without the pre-existing dysglycemia-related motility issues that can blunt a small additional slowing.
Second, the tirzepatide constipation rate is not linearly dose-dependent. SURMOUNT-1 shows 16.8, 17.1, and 11.7 percent across 5, 10, and 15 mg. The 15 mg arm reports less constipation than the 5 mg arm. The likely reason is early discontinuation: participants who develop severe GI issues at low doses drop out before they ever escalate, so the 15 mg denominator is enriched for GI-tolerant participants. This is survivorship bias, and it applies to every long-term GLP-1 adverse event table.
Third, the placebo arms are not zero. Weight loss itself, dietary change, and the psychology of being in a trial all move bowel habits. The delta over placebo, not the absolute rate, is the number that reflects drug effect. For STEP-1 semaglutide 2.4 mg, that delta is 12.7 percentage points. For SURMOUNT-1 tirzepatide 10 mg, it is 11.3.
The mechanism is mechanical, not neural
Every serious review of GLP-1 gastrointestinal effects lands in the same place: the drug slows gut motility from the stomach through the colon, and the further downstream you go, the harder the stool gets. The Jalleh et al. 2024 review in Lancet Gastroenterology & Hepatology synthesizes this well, and a case series with wireless motility capsule testing found delayed gastric emptying in 80 percent of GLP-1 users, small bowel transit delay in 33 percent, and colon transit delay in 33 percent.
There are two mechanistic layers.
Layer one is direct GLP-1 receptor activation on smooth muscle and enteric neurons. GLP-1 receptors are present throughout the gut wall, and activating them reduces peristalsis and alters the migrating motor complex that clears the small bowel during fasting.
On top of that sits vagal afferent signaling from the gut back to the brainstem. Kanoski et al. Endocrinology 2011 showed that surgical deafferentation of the subdiaphragmatic vagus attenuates the anorectic and motility effects of peripherally administered liraglutide and exendin-4 at low doses. Higher doses bypass the vagal route by hitting brainstem GLP-1 receptors directly. That is why the constipation profile does not fully resolve with a dose reduction: some of the signal is central.
Downstream, the consequence is straightforward. Slower stomach emptying delays how quickly a meal reaches the colon. Once it reaches the colon, transit slows further. The colon reabsorbs water from stool as a normal function; the longer stool sits, the more water it loses. Harder, drier stool, less frequent bowel movements, more straining. That is the entire pathophysiology.
Bottom line: GLP-1 constipation is not central. It is the same drug effect that produces the appetite suppression and satiety, just measured at the other end of the GI tract. You cannot separate the therapeutic effect from the constipation risk mechanistically. You can only manage the downstream water loss.
When constipation starts and when it fades
The Rubino et al. 2025 post hoc analysis of SURMOUNT-1 to -4 is the cleanest source on timing. GI adverse events on tirzepatide were mostly mild to moderate, clustered during dose escalation, diminished over time, and rarely led to treatment discontinuation. Symptomatic medication was used by fewer than one-third of participants across the four trials.
For most people, the practical timeline looks like this.
| Week | What tends to happen | What to do |
|---|---|---|
| 1 to 4 | First dose steps, mild delay in bowel frequency, harder stool possible | Front-load fluid and soluble fiber; osmotic if no bowel movement in 3 days |
| 4 to 12 | Titration continues; symptoms peak for many users; higher chance of needing a laxative regimen | Add osmotic (PEG 3350) daily; recheck fluid; add gentle exercise |
| 12 to 20 | Steady state on maintenance dose; symptom intensity typically trending down | Continue osmotic as needed; reassess fiber tolerance |
| 20+ | For the majority, GI symptoms have settled into a manageable baseline | Titrate laxative down; keep hydration habit |
Two caveats. First, symptoms do not fade for everyone. A subset carries chronic mild constipation for the duration of therapy. Second, every dose escalation can restart the clock. Moving from 5 mg to 10 mg tirzepatide is a new titration event mechanistically, even if the previous dose was well tolerated. Plan for a temporary re-emergence when you step up.
For dose specifics, the Zepbound dosage chart and Wegovy dosage chart walk through the standard titration schedules and give a reference point for where each escalation lands.
Evidence-informed management, in order
There is no randomized trial of laxative regimens specifically in GLP-1 users. The recommendations below are the standard chronic constipation ladder applied to a mechanistic profile of slowed transit with normal colonic anatomy. Start at the top and step down only after the mechanism is addressed at the level above.
1. Fluid, first and non-negotiable
Slower transit means more water reabsorbed from stool. Increasing water in reduces the amount of water the colon is able to reclaim. Aim for enough that urine stays pale straw-colored throughout the day. Coffee, tea, and other caffeinated fluids count. Alcohol is a net diuretic and does not.
The reason this matters more on a GLP-1 than off one: appetite suppression frequently reduces spontaneous fluid intake by 20 to 40 percent, because a large fraction of daily water comes attached to food. If someone eats meaningfully less, they also drink meaningfully less by default. This has to be replaced consciously.
2. Soluble fiber, titrated slowly
Psyllium husk (Metamucil) is the best-studied soluble fiber for chronic constipation. Start at half a normal serving to see how it interacts with the delayed gastric emptying. If the drug is already producing a full, slow-emptying stomach, adding bulk-forming fiber too quickly can worsen bloating and fullness without helping the downstream problem.
Insoluble fiber (wheat bran, raw vegetables in high volume) is worth being more cautious with. It adds bulk that has to move through a slowed system, and it is a common cause of "I added fiber and got worse."
3. Osmotic laxative
Polyethylene glycol 3350 (Miralax, generic PEG 3350) is the first-line osmotic. It pulls water into the colon and stays there rather than being absorbed. It is not a stimulant, has no cramping to speak of, is well tolerated for months to years, and works directly on the mechanistic problem. A standard starting dose is 17 g once daily; titrate down or up based on stool consistency. Magnesium-based osmotics (magnesium citrate, milk of magnesia) also work but need monitoring in anyone with reduced kidney function.
4. Stimulant laxative, short-term
Senna or bisacodyl. These trigger the enteric nervous system to increase peristalsis. They are appropriate as a rescue when the osmotic route has not moved things in 48 to 72 hours, and they are appropriate as short-term adjuncts during a titration event. They are not appropriate as an indefinite daily habit for most users, because the tolerance and dependency profile is real over months.
5. Prescription secretagogues
Linaclotide, plecanatide, lubiprostone. These are prescription options for chronic idiopathic constipation that persists despite osmotic laxative therapy. There is no specific GLP-1 constipation indication, but the underlying physiology (chronic slow-transit constipation) is what these are approved for. A gastroenterology referral is the right step if the OTC ladder has failed.
Tip: Do not rotate laxative classes daily. Pick one, use it consistently for two weeks, then adjust. Constipation regimens fail more often from inconsistency than from wrong choice.
When it is not just constipation
Most of what is written above applies to the majority of users, whose constipation is a manageable nuisance. A smaller subset needs a different level of vigilance.
The FDA added a warning about intestinal obstruction to the tirzepatide label in September 2023 after post-marketing case reports. The Jalleh et al. 2024 review and subsequent FAERS analyses of tirzepatide report bowel obstruction and ileus as identifiable signals, though the absolute event rates remain low relative to prescriptions. The point is not that GLP-1 users routinely obstruct. The point is that the mechanism that produces constipation is the same mechanism that, in a susceptible person, can slow transit to the point of pseudo-obstruction or true mechanical obstruction if there is a pre-existing adhesion or stricture.
Signals that warrant same-week medical evaluation rather than another laxative:
- Cramping abdominal pain plus vomiting. Not delayed satiety, not the mild nausea of dose escalation. Actual crampy pain with vomiting of stomach contents.
- A distended, tense abdomen with reduced or absent bowel sounds.
- No stool or flatus for more than 72 hours on a stable regimen where output had been normal.
- Fresh blood in stool or black tarry stool.
- Prior abdominal surgery with new-onset constipation of this severity. The base rate of adhesive obstruction is meaningfully higher.
None of these are common. All of them are worth an ED visit rather than a phone call. This is one of the reasons the GLP-1 pre-surgical aspiration guide and the ASGE periendoscopic guidance exist: the same delayed motility that produces constipation also produces the residual gastric contents that complicate anesthesia.
How constipation compares to the other GI signals
Constipation is one of four GI adverse events that appear together on essentially every GLP-1 label. The relative rates matter because they inform which one is most likely to drive discontinuation in a given person.
| Adverse event | STEP-1 semaglutide 2.4 mg | SURMOUNT-1 tirzepatide 10 mg | Placebo (pooled) |
|---|---|---|---|
| Nausea | 44.2% | 33.3% | ~10 to 14% |
| Diarrhea | 31.5% | 21.2% | ~10% |
| Constipation | 24.2% | 17.1% | ~6 to 11% |
| Vomiting | 24.8% | 12.2% | ~2 to 7% |
Nausea is by far the loudest signal and the one clinicians titrate around. Constipation is the quieter one that persists after the nausea has settled, because the underlying transit slowing does not fully compensate the way nausea often does. This is worth knowing when planning: the person who tolerates the nausea of the first four weeks is not out of the GI woods. They are moving into the constipation phase, and the management strategy is different.
For the other side of the GI risk spectrum on this drug class, see the GLP-1 gastroparesis evidence review (which covers the extreme end of gastric emptying delay), the GLP-1 gallbladder risk review (an adjacent hepatobiliary signal), and the broader GLP-1 dosing comparison across compounds.
Compound-specific notes
The mechanism is a class effect, but the numeric profile varies.
Semaglutide (Ozempic, Wegovy, Rybelsus). Constipation rate in obesity dosing (STEP-1, 2.4 mg weekly) sits at roughly 24 percent. The T2D dosing (SUSTAIN program at 0.5 to 1.0 mg weekly) runs lower, around 5 to 8 percent, because the steady-state dose is a third to a fifth of the obesity dose. Oral semaglutide (Rybelsus) has a comparable constipation profile to the injectable at equivalent absorbed dose. The full titration schedule for the injectable is in the semaglutide dosage chart; mechanism and pharmacology sit on the semaglutide peptide page.
Tirzepatide (Mounjaro, Zepbound). Rates cluster in the 12 to 17 percent range across doses in obesity trials and 7 to 11 percent in T2D trials. The dual GLP-1/GIP mechanism does not obviously produce more or less constipation than pure GLP-1 at equivalent weight-loss outcome. Head-to-head, SURMOUNT-5 tirzepatide vs semaglutide showed similar overall GI tolerability with the expected constipation-nausea trade-off. The dose ladder is in the tirzepatide dosage chart; pharmacology is on the tirzepatide peptide page.
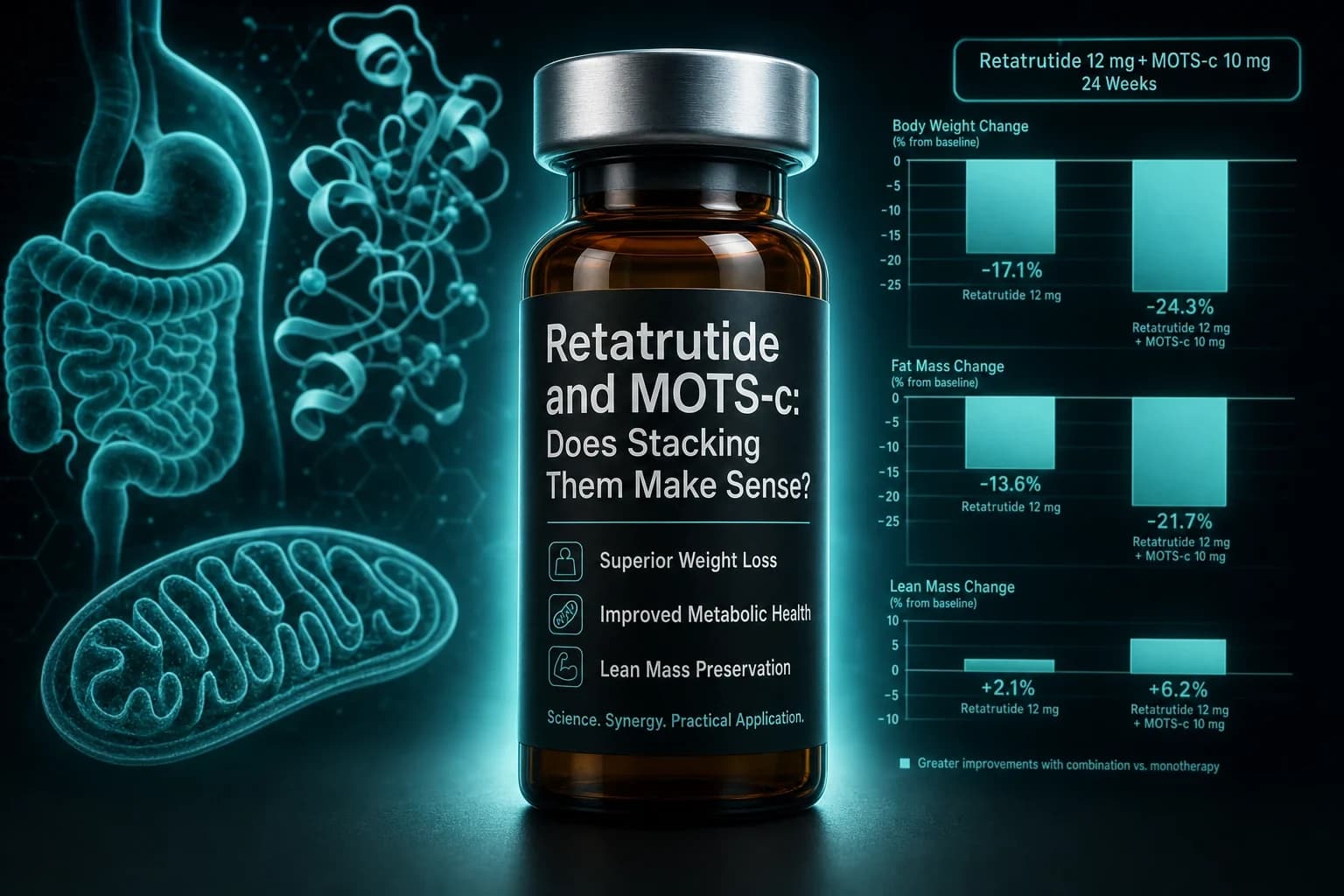
Retatrutide. Phase 2 constipation rates in the highest dose arm ran around 22 to 24 percent, which is closer to STEP-1 semaglutide than to SURMOUNT-1 tirzepatide. This tracks with retatrutide producing more absolute weight loss and pushing GI physiology harder overall. The full retatrutide GI-tolerability profile is in the retatrutide side effects article; the retatrutide peptide page covers mechanism.
Liraglutide (Saxenda, Victoza). Daily dosing at 3.0 mg (Saxenda) produces constipation in around 11 percent, roughly comparable to lower-dose tirzepatide. The daily rather than weekly PK produces a slightly different tolerability shape but not a different mechanism.
Practical decision framework
The question most people are actually asking is not "does this drug cause constipation" but "given my constipation on this drug, what should I do next." A short decision aid:
- Mild, week 1 to 4, no other symptoms. Water plus soluble fiber. Reassess in 7 days.
- Moderate, week 4 to 12, harder stool, less frequent bowel movements. Add daily PEG 3350 at 17 g. Do not stop the GLP-1 at this stage; the underlying titration curve will settle.
- Persistent past week 20 despite osmotic. Talk to the prescriber about either splitting the maintenance dose interval, dropping to the next dose down, or adding a prescription secretagogue. Consider a pause in escalation rather than escalation itself.
- Cramping pain, vomiting, or no output for over 72 hours. Same-week clinical evaluation, not another laxative.
- Weight loss goals achieved and considering dose reduction or discontinuation. The Stopping GLP-1s evidence review covers what happens on cessation across multiple domains, including a general resolution of the GI adverse event profile within weeks.
Sourcing considerations for research-use compounds
For readers running research-use GLP-1 compounds outside the prescription path, the constipation profile is not different because the underlying pharmacology is not different. What does matter for research use is dose accuracy. Uncertain dosing math is the single most common driver of unintentional over-titration, which is the fastest way to produce severe GI adverse events including constipation of the "I have not moved in five days" variety.
Two practical inputs improve dose reliability: verified reconstitution math and third-party COA on the vial. The reconstitution calculator handles the BAC water arithmetic; the Ascension Peptides vendor review walks through the COA and testing methodology on the injectable side, where 50% off using code ENHANCED applies. For oral GLP-1 research work, Limitless Biotech covers oral peptide formats with code ENHANCED.
The reason to mention this in a constipation article is prosaic: if the actual dose delivered is meaningfully higher than the intended dose because of bad reconstitution math, GI tolerability drops off a cliff. Getting the math right up front prevents 80 percent of the "I titrated too fast" stories.
Bottom line
Constipation on GLP-1s is real, quantifiable, mostly manageable, and rarely the reason people stop these drugs. The rates in the pivotal trials sit between 11 and 24 percent depending on compound and dose, most cases cluster during the first 12 to 20 weeks of titration, and the mechanism is downstream water reabsorption from slower colonic transit rather than anything neural or psychological.
Management follows the standard chronic constipation ladder with an emphasis on getting fluid right first, because appetite suppression predictably reduces spontaneous water intake. PEG 3350 handles the majority of cases that fluid and soluble fiber do not. Stimulant laxatives and prescription secretagogues remain available for the persistent minority. Bowel obstruction is rare but not zero, and the specific cluster of cramping pain, vomiting, and absent output warrants an urgent evaluation rather than another laxative.
One thing worth internalizing before starting a GLP-1: the constipation is not a bug in the drug that a better formulation will eventually engineer out. It is the same slowed gastric emptying that produces the satiety, measured at the other end of the gut. Plan for it, manage it early, and it becomes a minor tax rather than the reason therapy fails.
This article is for research and educational purposes only. GLP-1 receptor agonists are prescription medications; dose adjustments, laxative additions, and discontinuation decisions should be made with a qualified prescriber. Statistics cited come from the peer-reviewed publications linked inline. Nothing here is medical advice, and adverse-event rates from randomized trials do not always translate directly to real-world experience. If you are experiencing severe abdominal symptoms while on a GLP-1, seek clinical evaluation rather than relying on this or any other article.