At a glance
- Carmina 2023 (PMID 37762862): 27 obese PCOS women on semaglutide 0.5 mg weekly lost 7.6 kg in 3 months; ~80% saw menstrual cycles normalize.
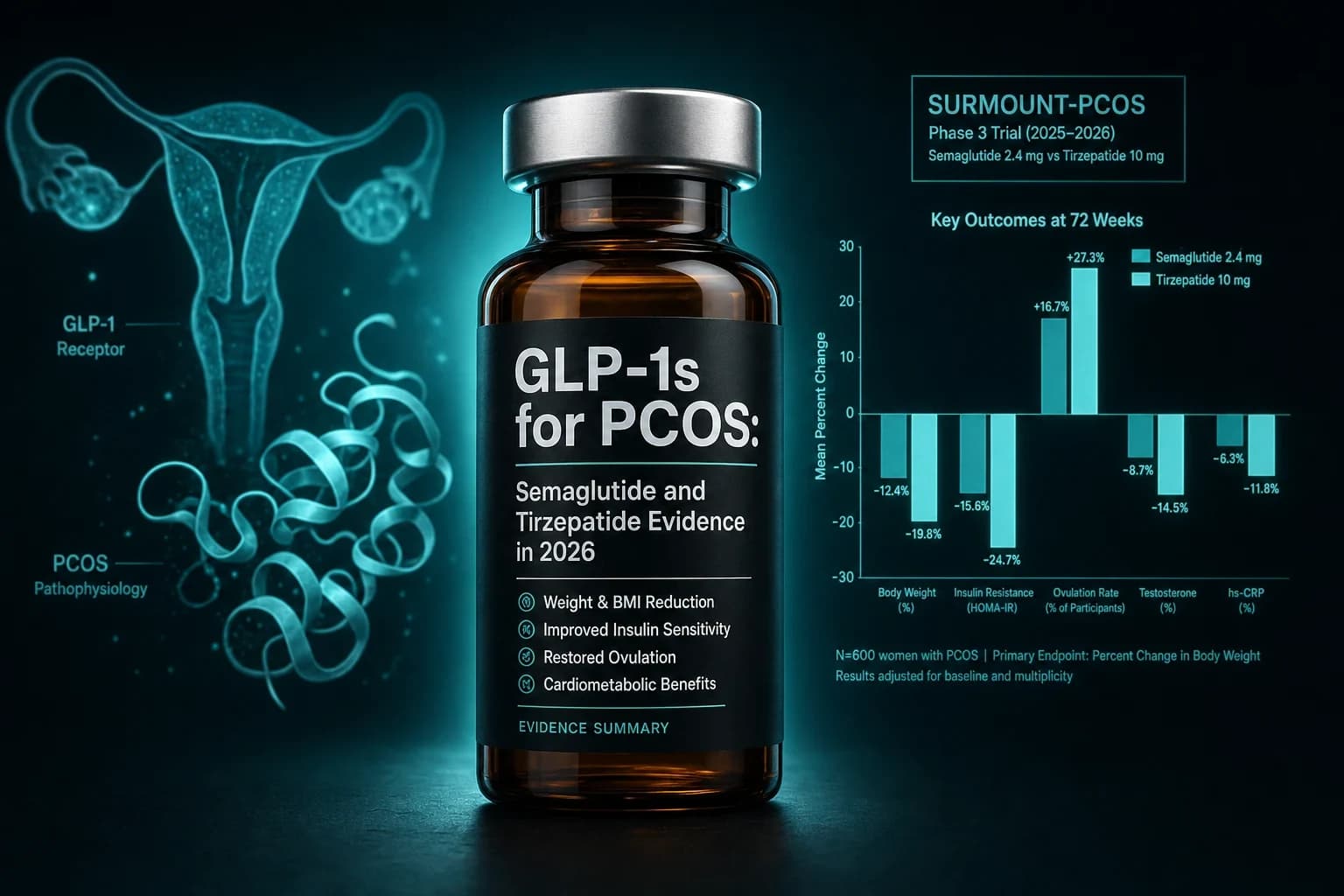
- ObesityWeek 2025 cohort of 4,241 women with PCOS on tirzepatide: 90.8% reached at least 10% weight loss at 10 months; mean loss 18.81%.
- Jensterle 2023 (PMID 36511825): semaglutide retained 37% of a solid meal in the stomach at 4 hours in PCOS women vs 0% on placebo; gastric half-emptying 171 vs 118 minutes.
- Chen 2025 RCT (PMID 40713699): metformin plus semaglutide produced a 35% natural pregnancy rate vs 15% on metformin alone in 100 overweight PCOS women.
- Jensterle 2024 withdrawal study: 25 PCOS women regained roughly one third of semaglutide-induced loss two years after stopping; 84% stayed below baseline weight and androgen gains held.
The shift the prescribing data made visible before the trial data did
Between 2021 and 2025, the share of women with PCOS prescribed semaglutide or tirzepatide for off-label weight loss rose from 2.4% to 17.6%, a roughly seven-fold jump that outpaced every other class of weight medication in the same window (Truveta 2025 analysis). The randomized data behind that shift are smaller than the prescribing trend suggests, but they are not nothing. Carmina and Longo got roughly 80% of obese PCOS patients to a normalized menstrual cycle on 0.5 mg semaglutide alone over three months (PMID 37762862). A 2024 Frontiers in Endocrinology withdrawal study showed weight regain after stopping the drug but with most of the androgen and ovulation benefit retained at two years (Jensterle et al. 2024). And the November 2025 ObesityWeek presentation of 4,241 PCOS women on tirzepatide put 90.8% of them at or beyond 10% body weight loss in ten months.
The short version is that semaglutide has the deepest published RCT base in PCOS, tirzepatide has the steepest real-world weight loss curve, and neither is FDA-approved for PCOS specifically.
Bottom line: In overweight or obese women with PCOS, semaglutide produces 7 to 14 kg of weight loss over 3 to 12 months, drops total and free testosterone, and normalizes menstrual cycles in roughly half to four fifths of responders. Tirzepatide shows larger real-world weight loss (18.8% mean in 4,241 women at 10 months) but the randomized PCOS data set is much smaller. Effects on ovulation and natural fertility are real but track closely with how much weight comes off, not with the drug itself.
The trials and cohorts that actually inform the question
Six datasets do most of the work for any honest 2026 read on GLP-1 receptor agonists in PCOS. Smaller case series exist; the table below limits itself to randomized trials, prospective cohorts, and the largest real-world dataset.
| Source | Design | n | Drug, dose | Duration | Key finding |
|---|---|---|---|---|---|
| Jensterle 2014 (PMID 25221543) | Observational | 84 | Liraglutide 1.2-1.8 mg/d | 4+ wk | Mean weight loss 9.0 kg; 81.7% lost more than 5% |
| Jensterle 2023 (PMID 36511825) | RCT, scintigraphy | 20 | Semaglutide 1.0 mg/wk | 16 wk | 37% gastric retention at 4 h vs 0% placebo |
| Carmina 2023 (PMID 37762862) | Prospective open-label | 27 | Semaglutide 0.5 mg/wk | 3 mo | -7.6 kg mean weight; ~80% menstrual normalization |
| 2024 PCOS meta-analysis (PMID 39178623) | Meta-analysis | 4 RCTs, 176 women | GLP-1 RAs vs placebo | Varies | Reduced BMI, triglycerides, waist circumference, total testosterone |
| Jensterle 2024 (DOI 10.3389/fendo.2024.1366940) | Observational, withdrawal | 25 | Semaglutide 1.0 mg/wk + metformin | 16 wk + 2 yr | 101 to 92 kg on therapy; 95 kg at 2 yr post-withdrawal; 84% below baseline |
| Chen 2025 (PMID 40713699) | RCT, open-label | 100 | Metformin +/- semaglutide 1.0 mg/wk | 16 wk | Combo: -6.09 kg vs -2.25 kg; 35% vs 15% pregnancy rate by wk 40 |
| 2025 Heliyon pilot (PMID 41421448) | Prospective pilot | 20 | Metformin + semaglutide 0.25-0.5 mg/wk | 5 mo | -13 kg, fat mass -9 kg, lean mass unchanged; 60% pregnancy in follow-up |
| ObesityWeek 2025 (Healio coverage) | Retrospective real-world | 4,241 | Tirzepatide titrated | 10 mo | 90.8% reached at least 10% loss; mean 18.81%; engagement bumped mean to 21.0% |
A few interpretive notes before the section-by-section read. Three of the trials are run by the same Slovenian group (Jensterle and colleagues), which means a chunk of the semaglutide PCOS evidence base shares one investigator team and one population sampling frame. The Chen 2025 RCT and the 2025 Heliyon pilot are the cleanest fertility-focused readouts. The tirzepatide PCOS evidence is dominated by one large real-world cohort and one ongoing Phase 4 trial (PERIODS), with the randomized data not yet published.
What semaglutide does in PCOS
The Carmina open-label study is the cleanest single read for the most common real-world protocol. Twenty-seven obese women with PCOS who had not lost weight on lifestyle intervention received semaglutide 0.5 mg subcutaneously once weekly for three months. Mean body weight fell 7.6 kg, mean BMI dropped 3.1 kg/m^2, and approximately 80% of the cohort reached the 5% weight-loss threshold (Carmina and Longo 2023, PMID 37762862). Roughly 80% of women whose menstrual cycles normalized on drug had been oligomenorrheic or amenorrheic at baseline.
Two methodological caveats matter. The Carmina cohort used 0.5 mg, not the 1.0 mg or 2.4 mg used in STEP-class obesity trials. The 7.6 kg figure understates what higher doses produce, and menstrual cycle normalization tracks the weight loss, not the dose.
The Jensterle gastric emptying study is mechanistically the most informative semaglutide-in-PCOS paper. Twenty obese women with PCOS underwent technetium scintigraphy at baseline and after 16 weeks of semaglutide 1.0 mg weekly. At four hours after a standardized solid test meal, the semaglutide group still had 37% of the meal in the stomach versus 0% on placebo. The half-emptying time stretched from 118 to 171 minutes (Jensterle et al. 2023, PMID 36511825). That paper is the cleanest in-PCOS evidence that semaglutide is acting via the same delayed gastric emptying mechanism that drives weight loss in non-PCOS obesity, and it is the reason GLP-1-related vomiting in pregnancy planning is taken seriously in the discontinuation literature.
A 2024 withdrawal study addresses the most common practical question women with PCOS ask their endocrinologist: what happens if I stop. Twenty-five women received semaglutide 1.0 mg weekly plus metformin 2,000 mg/day for 16 weeks, then continued metformin and lifestyle for two more years. Mean weight fell from 101 to 92 kg during semaglutide treatment, then rebounded to 95 kg by the two-year follow-up. Eighty-four percent of participants remained below baseline weight, and the free testosterone improvement seen on drug did not significantly deteriorate after discontinuation (Jensterle et al. 2024). The pattern is consistent with the broader stopping-GLP-1 weight regain research, which finds maintenance therapy with metformin or lifestyle programs blunts but does not eliminate the rebound.
Chen et al.'s 2025 randomized trial is the largest PCOS-specific RCT of semaglutide published to date. One hundred overweight or obese women with PCOS were randomized to metformin 1,000 mg twice daily or the same metformin plus semaglutide 1.0 mg weekly for 16 weeks. The combination group lost 6.09 kg versus 2.25 kg on metformin alone, showed greater reductions in total testosterone, and had higher rates of menstrual cycle recovery. The interesting endpoint is later in the trial timeline: from week 16 to week 40, the combination group had a 35% natural pregnancy rate versus 15% on metformin alone (Chen et al. 2025, PMID 40713699). Semaglutide was discontinued at week 16; pregnancy outcomes were measured after washout.
A 2025 Heliyon pilot replicated the fertility signal in a smaller, prospective sample. Twenty PCOS patients with obesity and prediabetes received metformin 1,000 mg daily plus semaglutide 0.25 to 0.5 mg weekly for five months. Body weight fell from 98.4 to 85.5 kg, fat mass dropped 9 kg, lean mass was preserved, and 60% of participants achieved pregnancy during the follow-up period (PMID 41421448). Lean mass preservation here is notable because the GLP-1 lean mass loss signal is a documented concern for the class, and the PCOS phenotype overlaps with sarcopenic patterns more often than is recognized.
What tirzepatide does in PCOS
The tirzepatide PCOS evidence base is structurally different from the semaglutide one. There is no published randomized trial yet. The largest dataset comes from a UK-based digital weight management service that prescribed tirzepatide to 4,241 women with PCOS and tracked them for ten months. Median age was 34, median BMI 35.6. At month ten, 96.6% reached at least 5% weight loss, 90.8% reached at least 10%, and 76.0% reached at least 15%. Mean weight loss was 18.81%, with engaged users hitting 21.0% versus 17.2% for non-engaged users (ObesityWeek 2025 presentation, Healio coverage November 2025).
These are real-world numbers, not a randomized trial, and a digital weight management service population is not representative of all PCOS patients. But the magnitudes track what tirzepatide produces in adult obesity outside PCOS (SURMOUNT-1 evidence and the tirzepatide vs semaglutide comparison), and the consistency suggests the underlying drug effect is similar in PCOS to what it does in obesity generally. If menstrual and androgen changes follow weight loss linearly, the implication is that tirzepatide should outperform semaglutide on those endpoints too, because the weight loss is larger.
The PERIODS Phase 4 trial is the missing randomized read. PERIODS is a 72-week, double-blind, placebo-controlled trial running across five German sites under University of Bonn sponsorship. The primary endpoint is improvement in ovarian dysfunction, defined by menstrual irregularity and ovulation frequency in premenopausal overweight or obese women with PCOS. The protocol titrates to the maximum tolerated dose (up to 15 mg) and is the first randomized study designed specifically to test whether tirzepatide produces ovarian dysfunction improvement beyond what weight loss alone delivers. PERIODS is not expected to report before late 2027.
Mechanism: is it the weight loss or the drug
Most defensibly, the dominant effect in PCOS is the weight loss, with a smaller but plausible direct contribution from gastric emptying and insulin-sparing.
PCOS is mechanistically anchored to hyperinsulinemia. Insulin drives ovarian thecal cell androgen production and lowers hepatic sex hormone-binding globulin (SHBG) synthesis, which raises free testosterone. Anything that reduces fasting insulin in PCOS reduces ovarian androgen output and raises SHBG, which lowers free testosterone, which reduces hyperandrogenic symptoms and shifts the LH-driven ovulation pattern back toward normal cyclicity. Weight loss of 5 to 10% is the threshold most PCOS guidelines flag as sufficient to restore ovulation in a majority of patients, regardless of the intervention that produced it.
Semaglutide and tirzepatide reduce body weight through appetite suppression, delayed gastric emptying, and central energy balance effects. None of these are PCOS-specific. A 2024 meta-analysis of GLP-1 receptor agonists versus placebo pooling four randomized PCOS trials (176 women) found reductions in BMI, waist circumference, triglycerides, and total testosterone, with no significant difference in HOMA-IR or total cholesterol (PMID 39178623). That pattern is consistent with the weight-loss-dominant mechanism: the drug works in PCOS because of the weight, not in spite of it.
The drug-direct hypothesis is not zero. The Jensterle gastric emptying paper documents that semaglutide-induced delayed emptying in PCOS is roughly the same magnitude as in non-PCOS obesity, suggesting no pharmacodynamic blunting in this population. A 2025 randomized study of taste perception in PCOS women on semaglutide found shifts in sweet and fat preference not fully explained by weight loss (PMID 40341357).
Note: The androgen and ovulation gains are anchored to weight loss. Patients who lose less than 5% of body weight on a GLP-1 receptor agonist generally do not see menstrual cycle normalization, even if their fasting insulin drops modestly. This is the same threshold that applies to bariatric surgery, lifestyle, and metformin in PCOS.
GLP-1 receptor agonists versus metformin
Metformin has been the cornerstone of PCOS pharmacotherapy for two decades. Two 2024 to 2026 meta-analyses compared GLP-1 receptor agonists head-to-head with metformin in PCOS.
The Cureus February 2026 systematic review pooled four randomized trials and 218 participants comparing GLP-1 receptor agonists with metformin in women with PCOS. The GLP-1 arms produced greater reductions in BMI, waist circumference, and insulin resistance, with comparable effects on menstrual cyclicity. No randomized trial reported a head-to-head fertility comparison (Cureus 18(2), DOI 10.7759/cureus.103927). The Scientific Reports 2025 meta-analysis (s41598-025-99622-4) reached the same direction with a slightly different included-trial set.
A decision matrix that emerges from these comparisons, with all the usual off-label caveats, looks roughly like this:
| Patient profile | Drug most data supports | Why |
|---|---|---|
| BMI 25-29 with insulin resistance | Metformin first line | Less expensive, oral, decades of fertility-safety data |
| BMI 30+ with insulin resistance | GLP-1 receptor agonist | Greater weight loss, larger androgen and menstrual effect |
| Failed metformin (no 5% loss at 6 mo) | Add or switch to GLP-1 | Strongest single indication for add-on therapy |
| Actively trying to conceive | Metformin maintained, GLP-1 stopped pre-conception | GLP-1 receptor agonists are not pregnancy-safe |
| Severe hyperandrogenism + obesity | GLP-1 + anti-androgen + metformin | Multi-mechanism approach for severe phenotype |
| Lean PCOS, BMI under 25 | Neither, lifestyle and ovulation-induction first | GLP-1 evidence in lean PCOS is sparse |
The combination question (metformin plus semaglutide vs metformin alone) has the cleanest fertility evidence. The Chen 2025 trial and the 2025 Heliyon pilot both used the combination and both reported pregnancy signals. No published trial has directly compared the combination to GLP-1 monotherapy in PCOS.
Fertility and pregnancy
This is the part that needs the most care. GLP-1 receptor agonists are not approved for use in pregnancy and the label specifically directs discontinuation before conception. Reproductive toxicology data are mixed, but the standing recommendation across endocrine societies is to stop semaglutide at least two months and tirzepatide at least one month before attempting conception, in line with the drugs' half-lives and to allow GI tone to normalize before pregnancy.
What the trials actually measured is post-washout pregnancy. The Chen 2025 design is the cleanest illustration: semaglutide was given for 16 weeks alongside metformin, then discontinued, with pregnancy outcomes followed for an additional 24 weeks. The 35% pregnancy rate in the combination arm versus 15% in the metformin-only arm was measured after semaglutide was out of the system. The implication is that the weight loss and the androgen and menstrual improvements that occurred during the active treatment phase persisted long enough into the washout to drive a higher conception rate.
The 2025 Heliyon pilot reinforced the same pattern. Of 20 PCOS patients on metformin plus semaglutide for five months, 60% achieved pregnancy during follow-up. Body composition data from the same study showed fat mass loss without lean mass loss, which is the body composition profile most likely to support implantation and early pregnancy (PMID 41421448).
Warning: Do not continue semaglutide, tirzepatide, or any GLP-1 receptor agonist into a known or planned pregnancy. The official labels and Canadian Women's Health Today 2025 guidance recommend stopping semaglutide at least two months and tirzepatide at least one month before attempting conception. If a pregnancy occurs while on drug, the standing recommendation is immediate discontinuation and obstetric consultation. None of the PCOS fertility data described above involved on-treatment pregnancy.
Side effects, safety, and what to flag
GI side effects in PCOS populations follow the same pattern as in non-PCOS obesity: nausea, vomiting, constipation, and diarrhea, predominantly during dose escalation. The Carmina cohort reported "very few" side effects at 0.5 mg, which is the lowest standard dose. The Jensterle and Chen trials used 1.0 mg and reported the full GI profile.
Three signals warrant specific attention in PCOS:
-
Lean mass. PCOS commonly overlaps with insulin-resistance-driven body composition that already includes elevated fat mass relative to lean mass for any given BMI. The general GLP-1 lean mass loss research shows roughly 25 to 40% of total weight loss comes from lean tissue without resistance training intervention. The 2025 Heliyon pilot is a counterpoint: lean mass was preserved in combination therapy with adequate protein. Protein target of 1.6 to 2.2 g/kg target body weight and 2 to 3 resistance sessions per week is the standard recommendation derived from the broader literature.
-
Hair shedding. Telogen effluvium from rapid weight loss is the dominant mechanism behind the GLP-1 hair loss signal. PCOS patients often have baseline androgenetic pattern hair thinning, which means a telogen pulse from rapid weight loss can unmask pre-existing pattern loss. Slower titration and screening for ferritin and iron are the standard mitigation.
-
Mood and anxiety. PCOS is associated with elevated rates of depression and anxiety. The general GLP-1 mental health evidence is reassuring on average, but individual susceptibility varies and the rapid weight loss context can amplify body image stress.
The Cureus 2026 meta-analysis reported no signal increase in serious adverse events on GLP-1 receptor agonists versus metformin across the included trials, but the sample sizes were too small to characterize rare events. The cancer-risk question covered in the GLP-1 cancer risk meta-analysis review is the same in PCOS as in obesity generally: no signal in current cohort and trial data, but the PCOS-specific cancer-risk profile (endometrial cancer is elevated at baseline in PCOS) has not been directly measured in any GLP-1 trial.
Where the evidence is still soft
Four gaps shape the honesty of a 2026 read:
- No randomized tirzepatide PCOS trial has reported. PERIODS is the first dedicated Phase 4 and does not read out before late 2027. Everything on tirzepatide in PCOS is observational or real-world.
- Long-term ovarian outcomes are unmeasured. No trial has followed PCOS patients on GLP-1 receptor agonists past two years.
- Fertility outcomes are post-washout only. Conception-rate signals come from short courses followed by discontinuation, not continuous on-treatment data.
- Lean PCOS is unstudied. Roughly 20 to 30% of PCOS patients have BMI under 25, and the trials almost exclusively enrolled overweight or obese patients.
What this means for women with PCOS researching their options today
Three takeaways do most of the work:
- If you have BMI 30+, PCOS, and have failed metformin or lifestyle, GLP-1 receptor agonists have the best published evidence in this population for restoring menstrual cyclicity and lowering androgens. The mechanism runs through weight loss; the magnitude tracks the dose; tirzepatide has the steepest real-world weight loss but the smallest randomized trial base.
- If you are trying to conceive, the published data support short-course GLP-1 therapy with metformin, washout, then conception attempts. Continuous on-treatment conception is not what the trials measured and is not what the labels permit.
- If you have lean PCOS or BMI under 27, the evidence base is thin and the standing first-line therapy remains metformin and lifestyle. GLP-1 receptor agonists in this phenotype are unstudied territory.
For researchers and clinicians tracking dosing logistics on the injectable side, the reconstitution calculator covers the BAC water math for any standard semaglutide or tirzepatide protocol. The GLP-1 dosing comparison covers titration schedules across the class, including the slower-titration approach most often recommended for PCOS patients who want to limit the rate of weight loss and the associated telogen and lean mass risks.
Researchers sourcing reference standards in the compounded space have access to semaglutide, tirzepatide, and cagrilintide through Ascension Peptides with public per-batch COAs and 50% off using code ENHANCED.
FAQ
Will GLP-1 receptor agonists restore my menstrual cycle without weight loss?
Probably not. The published menstrual cycle restoration data are concentrated in women who lost at least 5% of body weight on the drug. Carmina 2023 and the 2024 meta-analysis both anchor the menstrual benefit to the weight loss, not to a direct ovarian effect. Patients who lose less weight tend to see proportionally smaller hormonal changes.
Do I have to stop semaglutide or tirzepatide before trying to conceive?
Yes. The labels for both drugs explicitly recommend discontinuation before conception, and the standing guidance is roughly two months for semaglutide and one month for tirzepatide based on half-life and to allow GI tone to normalize. No PCOS fertility trial has measured outcomes on continuous treatment because the labels prohibit it.
Can I take metformin with semaglutide or tirzepatide?
In practice yes, and the combination has the cleanest fertility evidence in PCOS. The Chen 2025 trial and the 2025 Heliyon pilot both used metformin plus semaglutide. The combination produced larger weight loss, larger androgen reductions, and higher post-washout pregnancy rates than metformin alone in the Chen comparison.
Is tirzepatide better than semaglutide for PCOS?
The randomized evidence does not allow a clean answer because no trial has compared them head-to-head in PCOS specifically. Indirect comparison suggests tirzepatide produces larger weight loss in real-world PCOS cohorts (18.8% mean at 10 months vs 7-15% on semaglutide across trials), which by the weight-loss-dominant mechanism should mean larger menstrual and androgen effects. PERIODS Phase 4 may eventually answer this directly, but not before late 2027.
Will I gain the weight back if I stop?
Some, but not all. The Jensterle 2024 withdrawal study is the best evidence: at two years after stopping semaglutide, 25 women had regained roughly one third of the lost weight but 84% remained below baseline. Free testosterone gains did not significantly deteriorate, suggesting some metabolic benefit persists past discontinuation when metformin and lifestyle are continued.
What about hair loss?
PCOS patients have a higher baseline rate of androgenetic alopecia, and the rapid weight loss telogen pulse on GLP-1 receptor agonists can unmask it. The GLP-1 hair loss research review covers the timeline, mitigation, and when to escalate.
Is semaglutide off-label for PCOS?
Yes. No GLP-1 receptor agonist is approved by the FDA or EMA for PCOS. PCOS use is off-label in every jurisdiction.
This article is for educational and research purposes only. It summarizes peer-reviewed randomized trial, observational cohort, prospective open-label, meta-analysis, and conference-abstract data on GLP-1 receptor agonists (primarily semaglutide and tirzepatide) in women with polycystic ovary syndrome. Nothing in this article is medical advice, diagnostic guidance, or a recommendation to start, stop, or modify any prescription drug or research compound. PCOS is a heterogeneous syndrome with several validated diagnostic criteria and many possible treatment paths. Decisions about pharmacotherapy, fertility planning, and contraception should be made with a reproductive endocrinologist, primary care clinician, or obstetric provider who can review individual history. Pregnancy planning while on a GLP-1 receptor agonist requires individualized clinical consultation and discontinuation per label guidance.