At a glance
- Phase 2 NEJM trial (Jastreboff et al. 2025, PMID 40549887): up to 16.2% mean weight loss at 52 weeks in obesity without diabetes, up to 12.3% with type 2 diabetes
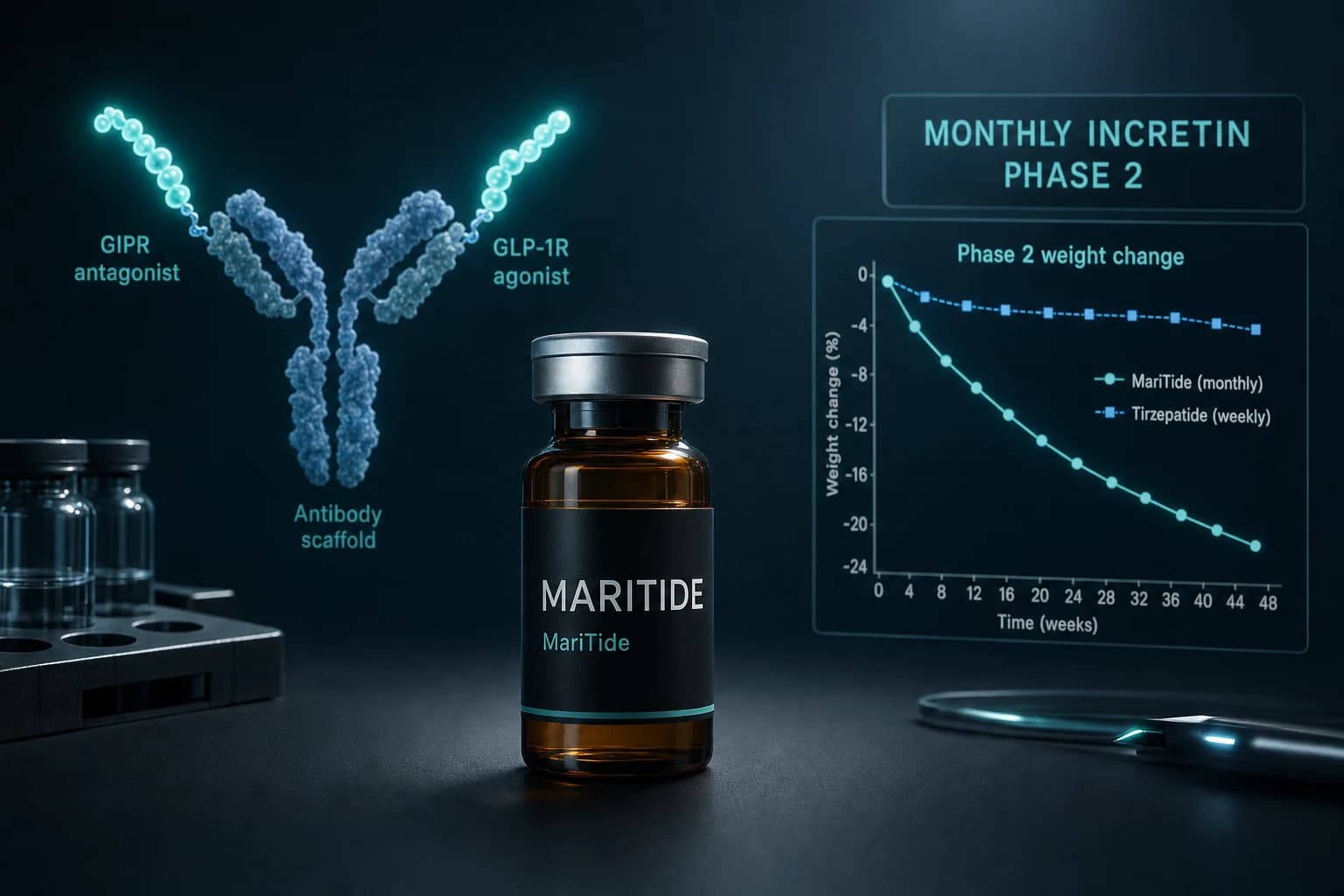
- Mechanism is the inverse of tirzepatide: a GIPR antagonist antibody conjugated to two GLP-1 agonist peptides, dosed once monthly
- Weight curves had not plateaued at 52 weeks, suggesting the ceiling is higher than what the Phase 2 readout shows
- GI adverse events drove discontinuation rates of 12 to 27 percent without dose escalation; the Phase 3 MARITIME program uses an 8-week titration starting at 21 mg
- MariTide is an Amgen biologic, not a research peptide. Compounded or grey-market versions do not exist and would not replicate the antibody scaffold
A monthly weight-loss shot that goes the opposite direction on GIP
Tirzepatide is a GIP receptor agonist. MariTide is a GIP receptor antagonist. Both produce double-digit weight loss. That contradiction is the most interesting thing in obesity pharmacology right now, and the Phase 2 data published in the New England Journal of Medicine in 2025 is the first large human readout that forces the field to take it seriously.
Maridebart cafraglutide, also called MariTide and AMG 133, is Amgen's bid to compete in the GLP-1 era without copying it. It is dosed once a month instead of weekly, it is built as a peptide-antibody conjugate instead of a small peptide, and it blocks GIP signaling instead of activating it. The Phase 2 trial reported mean weight reductions of 12.3 percent to 16.2 percent at 52 weeks in adults with obesity and 8.4 percent to 12.3 percent in adults with obesity plus type 2 diabetes (Jastreboff et al., NEJM 2025).
That puts MariTide in roughly the same league as semaglutide 2.4 mg weekly, behind tirzepatide 15 mg weekly, and ahead of every once-monthly obesity candidate that has reported human data. The weight curve had not flattened at 52 weeks, which is the most important sentence in the paper.
Bottom line: MariTide produces tirzepatide-class weight loss on a monthly schedule using the opposite GIP mechanism. The Phase 2 number people quote is 16.2 percent, but that is mean change at 52 weeks before any plateau, in dose groups that did not yet use the gentler titration the Phase 3 program adopted.
What maridebart cafraglutide actually is
Most obesity drugs in this generation are peptide analogues of native incretin hormones. Semaglutide is a long-acting GLP-1 analogue. Tirzepatide is a single peptide that activates both GIP and GLP-1 receptors. Retatrutide is a triple agonist of GLP-1, GIP, and glucagon receptors. They are all small molecules by biologic standards, dosed weekly, cleared in days.
Maridebart cafraglutide is built differently. It is a fully human IgG2 monoclonal antibody that antagonizes the GIP receptor, with two GLP-1 agonist peptides chemically conjugated to the antibody backbone using amino acid linkers. The antibody scaffold extends the half-life dramatically, which is what makes once-monthly dosing possible. The structural details and discovery program are described in the AMG 133 medicinal chemistry paper and the Nature Metabolism preclinical-plus-Phase-1 report (Lu et al., Nature Metabolism 2024).
The mechanism logic comes from earlier preclinical work showing that anti-GIPR antibodies caused weight loss in mice and obese non-human primates, and that combining GIPR antagonism with GLP-1 receptor agonism produced more weight loss than either approach alone (Killion et al., Sci Transl Med 2018). MariTide is the engineered version of that two-pronged hypothesis: block GIP, agonize GLP-1, and use an antibody to make the dosing schedule humane.
The Phase 2 results in plain numbers
The Phase 2 trial randomized 592 adults with obesity (465 without diabetes, 127 with type 2 diabetes) to placebo or one of several maridebart dose regimens, with treatment continuing for 52 weeks. Primary endpoint was percent change in body weight from baseline.
| Group | Dose regimen | Mean weight change at 52 weeks |
|---|---|---|
| Obesity, no diabetes | Placebo | -2.5% |
| Obesity, no diabetes | Maridebart, range across arms | -12.3% to -16.2% |
| Obesity + T2D | Placebo | -1.7% |
| Obesity + T2D | Maridebart, range across arms | -8.4% to -12.3% |
Source: Jastreboff et al., NEJM 2025 (PMID 40549887).
A few details that get lost in the headline:
- The 16.2 percent figure is the upper end of mean change, not the responder ceiling. Individual participants on the highest-dose arms exceeded that.
- HbA1c dropped 1.2 to 1.6 percentage points in the diabetes cohort. That is competitive with current GLP-1 therapy in T2D.
- The weight loss curve was still trending downward at week 52. The trial did not run long enough to find the plateau, which is unusual for obesity Phase 2 work.
- The diabetes cohort lost less weight than the non-diabetes cohort, which is a consistent pattern across GLP-1 class trials and not a MariTide-specific limitation.
How MariTide stacks up against the rest of the class
The fair comparison is mean weight loss in the high-dose arm of each pivotal obesity trial in adults without type 2 diabetes. Trial design and duration vary, so this is a directional comparison, not a head-to-head.
| Drug | Pivotal trial | Schedule | Highest-dose mean weight loss | Duration |
|---|---|---|---|---|
| Semaglutide 2.4 mg | STEP 1 (Wilding et al., NEJM 2021, PMID 33567185) | Weekly SC | -14.9% | 68 weeks |
| Tirzepatide 15 mg | SURMOUNT-1 (Jastreboff et al., NEJM 2022, PMID 35658024) | Weekly SC | -20.9% (treatment-regimen) / -22.5% (efficacy) | 72 weeks |
| Retatrutide 12 mg | Jastreboff et al., NEJM 2023 | Weekly SC | -24.2% | 48 weeks |
| Maridebart cafraglutide | Phase 2 (Jastreboff et al., NEJM 2025, PMID 40549887) | Monthly SC | -16.2% | 52 weeks |
The honest read: MariTide is roughly semaglutide-tier on a monthly schedule, in a Phase 2 trial that did not reach steady state. Whether it can climb into tirzepatide territory in Phase 3 is the central open question.
For background on the comparator molecules, see our pages on tirzepatide, semaglutide, and retatrutide, and the orforglipron oral GLP-1 Phase 3 evidence guide for the small-molecule oral angle.
The GIP paradox: why does antagonism work when agonism also works?
This is the part that bothers everyone who looks at the field for the first time. Tirzepatide is a GIP receptor agonist. Maridebart is a GIP receptor antagonist. Both produce double-digit weight loss when combined with GLP-1 receptor agonism. They cannot both be straightforwardly correct in the simple "GIP signaling drives weight loss" or "GIP signaling drives weight gain" sense.
The leading explanation is functional desensitization. Sustained high-amplitude GIPR agonism, the kind tirzepatide produces, downregulates GIP receptors at the surface of adipocytes and rapidly desensitizes the receptor. The end result starts to resemble pharmacological antagonism, even though the molecule is technically an agonist (Killion et al. 2020, PMID 33020469). A 2025 review summarizes the broader case for why both pharmacologic strategies can lower body weight despite pointing in opposite directions, and what the underlying physiology implies for next-generation drugs (Hammoud and Drucker, 2025, PMID 40521869). A second 2025 review walks through the historical and genetic evidence that motivated both the agonist and antagonist programs in parallel (Premise of the Paradox, 2025, PMID 40507574).
The clinical implication for readers: do not assume the two strategies are interchangeable. They produce overlapping outcomes by partly different mechanisms, and the metabolic profile, lean mass effects, and durability question may diverge in Phase 3.
Side effects, dose escalation, and what the Phase 3 design fixes
GLP-1 class drugs share a tolerability problem: nausea, vomiting, constipation, and the discontinuations that follow. MariTide's Phase 2 was no exception, and the absence of dose escalation in some arms made the GI signal worse than necessary.
The cleanest summary is this: in arms that used dose escalation, total adverse-event discontinuation was around 11 percent and GI-related discontinuation was under 8 percent. In arms without dose escalation, GI-related discontinuation reached 12 to 27 percent in the obesity cohort and 6 to 16 percent in the diabetes cohort. Nausea and vomiting were typically mild and concentrated around the first dose, with median resolution of about six days for nausea and one to two days for vomiting.
Two design implications carry into Phase 3:
- The MARITIME program uses an 8-week dose escalation that starts at 21 mg and titrates to target doses of 35 mg or 70 mg. This is the same logic Eli Lilly used to make tirzepatide tolerable.
- The monthly schedule means that any given dose stays in circulation longer than a weekly drug. If a patient has a bad reaction, you cannot simply skip the next shot; the antibody is still there. This is a real practical difference between MariTide and weekly GLP-1s, and it shapes how clinicians will manage tolerability.
Note: Monthly dosing is convenient, but it changes the side-effect-management playbook. Adverse events from a long-acting biologic do not disappear when you stop dosing. They taper over the antibody half-life, which is weeks, not days.
What's coming: the MARITIME Phase 3 program
The Phase 3 program covers obesity, type 2 diabetes, and several obesity-related comorbidity studies.
| Trial | Population | Size | Primary read |
|---|---|---|---|
| MARITIME-1 | Obesity or overweight, no T2D | ~3,500 | Weight loss at 72 weeks |
| MARITIME-2 | Obesity or overweight + T2D | ~999 | Weight loss + glycemic control at 72 weeks |
| Obesity + OSA | Obstructive sleep apnea | TBD | AHI reduction (planned start 2025) |
| Cardiovascular outcomes | ASCVD | TBD | MACE (planned start 2025) |
| Heart failure | HFpEF or HFrEF | TBD | Composite endpoints (planned start) |
| Additional T2D studies | T2D | TBD | Three studies planned to initiate in 2026 |
The strategic shape of this program looks a lot like Lilly's SURMOUNT and SURPASS programs around tirzepatide, plus Novo's SELECT and STEP programs around semaglutide. The bet is that the indication that wins approval first (obesity) is the one that opens the door, and the cardiovascular outcomes trial is what makes payers cover the drug at scale.
For context on how comorbidity-focused trials matter for label expansion in this class, see tirzepatide for HFpEF after SUMMIT and tirzepatide for sleep apnea after SURMOUNT-OSA.
Why MariTide will not exist as a research peptide
This is the section most peptide-curious readers actually want and rarely get from mainstream coverage.
MariTide is a peptide-antibody conjugate. The peptide half is the GLP-1 agonist. The antibody half is a fully human monoclonal IgG2 against the GIP receptor. You cannot synthesize a monoclonal antibody on a peptide synthesizer. You cannot reconstitute it from a vendor's lyophilized vial of "MariTide research only." Antibody production requires mammalian cell culture lines, conjugation chemistry that is precisely characterized for the linker and the drug-to-antibody ratio, and quality control that the research peptide market is structurally not equipped to do.
When something shows up online claiming to be MariTide for sale, one of three things is happening:
- It is mislabeled. Most commonly, it is a long-acting GLP-1 analogue or a tirzepatide variant being sold under a trending name.
- It is partially the right peptide component without the antibody scaffold, which is to say it is not MariTide.
- It is a scam.
This is the same pattern we covered when teasing out where to actually source compounds with verifiable certificates of analysis in our BPC-157 vendor and COA review and the broader best legit peptide vendors of 2026.
Warning: Any vendor claiming to sell maridebart cafraglutide, MariTide, or AMG 133 for research use is not selling the same molecule that produced the Phase 2 data. The antibody scaffold is the molecule. Without it, you have a different drug.
What this means if you are looking at GLP-1 alternatives today
If you are interested in the MariTide story because you are weighing what to actually use right now, the path splits cleanly:
- For approved obesity therapy with the strongest evidence today, that is tirzepatide (Zepbound) and semaglutide (Wegovy). MariTide is not approved and will not be for at least another year or two.
- For research peptide exploration with verifiable COAs, GLP-1 class compounds and their reconstitution math are the practical entry point. Our reconstitution calculator is the tool to plug numbers into.
- If you care about lean mass during weight loss, the GLP-1 class generally drives 20 to 40 percent of total weight loss from lean tissue. The mechanism on MariTide will likely look similar, since the GLP-1 component is doing most of the appetite suppression. Our GLP-1 muscle loss research walks through the strategies that hold up.
- If you are thinking about what happens after stopping, weight regain is the rule, not the exception. The stopping GLP-1s and weight regain research covers the maintenance question and what can soften the rebound.
For research-grade injectable peptides that are actually available with batch-tested COAs, Ascension Peptides is where most of the people we trust source from. Code ENHANCED takes 50 percent off. For oral and nasal forms in the same broad space, Limitless Biotech carries oral peptides and nasal sprays; code ENHANCED applies there too. Neither of them carries MariTide, and you should be skeptical of anyone who claims to.
Honest evidence summary
- Mechanism: novel and well-supported in preclinical work. The bispecific GIPR-antagonist plus GLP-1-agonist scaffold is the first of its kind to deliver Phase 2 efficacy data.
- Efficacy: 12.3 to 16.2 percent mean weight loss at 52 weeks in obesity without T2D is competitive with semaglutide on a monthly schedule. Whether MariTide can match tirzepatide once Phase 3 dose escalation is in place is the open question.
- Safety and tolerability: typical GLP-1 class GI profile, with the long half-life adding a wrinkle clinicians will need to manage. Phase 2 discontinuation rates without dose escalation were higher than the eventual Phase 3 program will likely report.
- Clinical timing: Phase 3 is recruiting now. The earliest plausible regulatory submission is roughly 2027 to 2028 if MARITIME-1 reads out cleanly. No commercial launch is imminent.
- Practical takeaway: this is the obesity story to follow over the next 18 months, not a treatment to act on today.
Bottom line
MariTide is the first credible monthly contender in the GLP-1 era and the first molecule built around GIP receptor antagonism to make it through a 500-plus-patient Phase 2 trial with double-digit weight loss. The Phase 2 results put it in semaglutide's neighborhood at a fraction of the injection frequency, the curve was still falling at 52 weeks, and the Phase 3 program addresses the tolerability problem the Phase 2 program flagged. None of that translates into a research peptide you can buy today, and any vendor implying otherwise is selling something else.
The realistic mental model: watch MARITIME-1 in 2027, expect a real fight between Amgen, Lilly, and Novo for share of the next-generation obesity market, and remember that the GIP biology question is far from settled even after the headline numbers.
This article is for educational and research purposes only. Maridebart cafraglutide is investigational and not approved by any regulator. Tirzepatide and semaglutide referenced above are FDA approved for the indications cited; this content is not medical advice and is not a substitute for guidance from a qualified clinician. Citations link to PubMed for verification.