At a glance
- ATTAIN-1: 12.4% mean weight loss at 36 mg over 72 weeks (Wadden et al. NEJM 2025)
- ATTAIN-2 in T2D: 10.5% weight loss with HbA1c down 1.3 to 1.8 percentage points
- ACHIEVE-3: orforglipron beat oral semaglutide on HbA1c by 0.44 to 0.48 points at 52 weeks
- First non-peptide GLP-1 receptor agonist to clear a Phase 3 program
- Once-daily oral, no food or water restrictions, unlike Rybelsus
- Not yet FDA-approved; global regulatory submissions filed across 2025 and 2026
Orforglipron is the first non-peptide oral GLP-1 to clear Phase 3
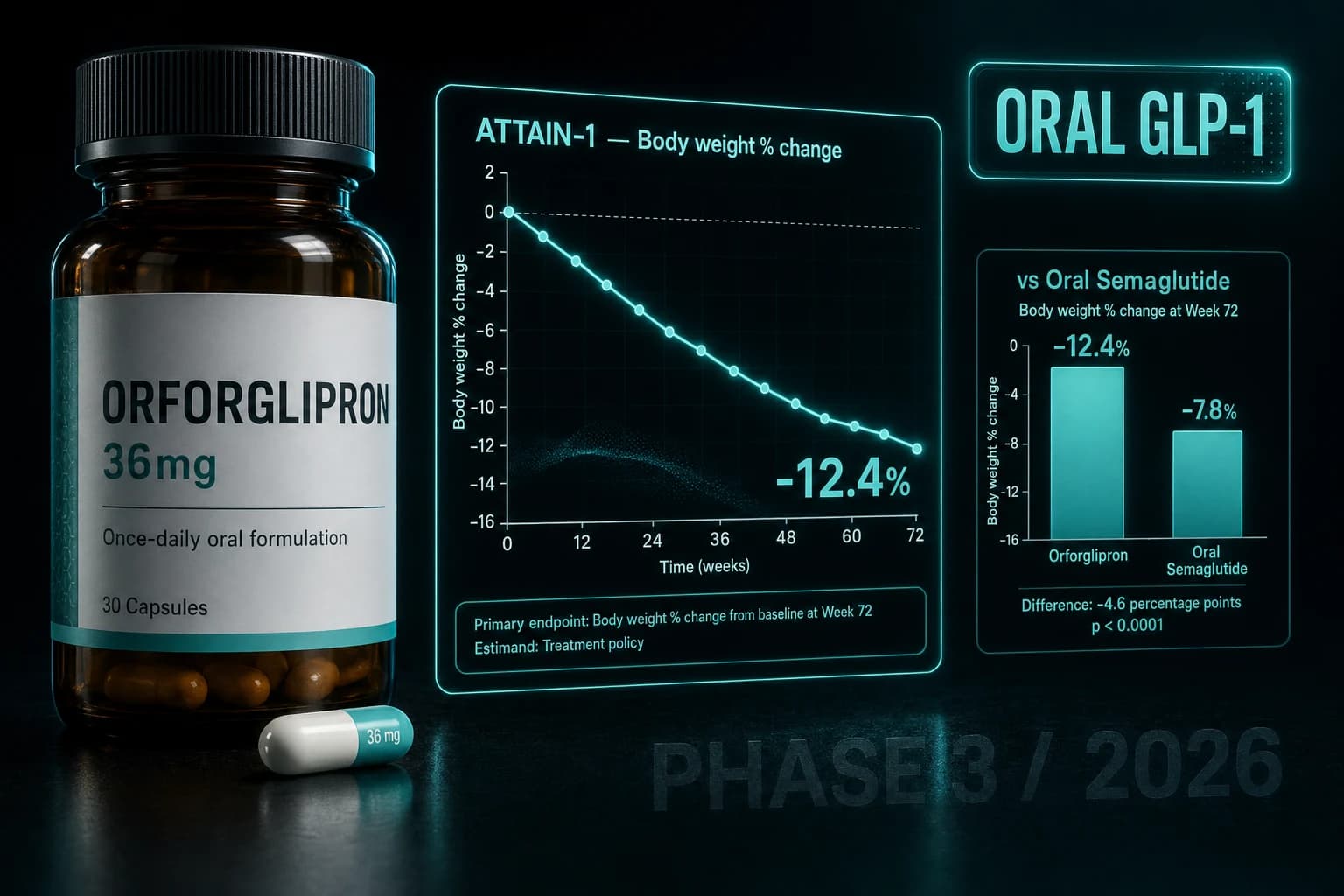
Eli Lilly's orforglipron is the first small-molecule, non-peptide GLP-1 receptor agonist to finish a positive Phase 3 program. In the obesity readout, the 36 mg dose produced 12.4% mean weight loss over 72 weeks (Wadden et al. NEJM 2025). In the diabetes head-to-head, it beat oral semaglutide on HbA1c by 0.44 to 0.48 percentage points at 52 weeks (ACHIEVE-3, Lancet 2026).
For an oral pill with no food or water restrictions, those numbers are the most aggressive readout the GLP-1 class has delivered outside of injectable tirzepatide and retatrutide.
This article walks through what orforglipron actually is at the molecule level, what each of the four published Phase 3 readouts (ATTAIN-1, ATTAIN-2, ACHIEVE-1, ACHIEVE-3) showed in hard numbers, and where it fits against tirzepatide, semaglutide, and retatrutide for researchers tracking the class.
What orforglipron actually is
Orforglipron is a once-daily oral GLP-1 receptor agonist. Two design choices distinguish it from the rest of the class in clinical use.
First, it is a small molecule, not a modified peptide. Semaglutide and tirzepatide are peptide derivatives of native GLP-1 (and GIP, in the case of tirzepatide) with structural changes that extend half-life. Orforglipron was discovered through a Chugai Pharmaceutical screening program and licensed to Lilly. Its molecular weight is roughly one-tenth of semaglutide. It is not absorbed via the same mechanisms and does not require an absorption enhancer like SNAC.
Second, it has been characterized as a partial agonist with a biased signaling profile. The compound preferentially activates cyclic AMP signaling at GLP-1R while showing reduced beta-arrestin recruitment relative to peptide agonists (Wharton et al. NEJM 2023). The pharmacologic argument is that biased agonism may produce less receptor internalization and desensitization. Whether that translates to differentiated long-term efficacy is still unsettled.
The practical consequence of the small-molecule design is the dosing instruction. Oral semaglutide (Rybelsus) requires fasting, plain water (no more than 4 ounces), and a 30-minute window before food or other liquids. Orforglipron has none of those constraints. Once daily, any time, with or without food.
That removes the single largest barrier to oral GLP-1 adherence outside of cost.
ATTAIN-1: the obesity readout
ATTAIN-1 is the pivotal Phase 3 weight loss trial in adults with obesity but without type 2 diabetes (Wadden et al. NEJM 2025).
Design:
- 72 weeks
- Doses: 6 mg, 12 mg, 36 mg, placebo (3:3:3:4 randomization)
- Adjunct to lifestyle intervention
Results at 36 mg, week 72:
- Mean weight reduction: 12.4% (about 27.3 lb)
- 54.6% of participants reached 10% or more loss (vs 12.9% on placebo)
- 36.0% reached 15% or more (vs 5.9% on placebo)
- 18.4% reached 20% or more (vs 2.8% on placebo)
Cardiometabolic markers improved as well. Waist circumference, systolic blood pressure, triglycerides, and non-HDL cholesterol all moved in the expected GLP-1 direction.
The shape of the response curve matters. In injectable trials, weight loss often continues to deepen through 68 to 72 weeks with semaglutide and tirzepatide. ATTAIN-1 followed the same pattern. The mean curve had not fully plateaued at week 72, which leaves room for potential additional reduction with longer exposure.
Headline comparison to STEP 1 (semaglutide 2.4 mg, 68 weeks): ATTAIN-1 36 mg fell short of semaglutide's 14.9% mean reduction. Comparison to SURMOUNT-1 (tirzepatide 15 mg, 72 weeks): ATTAIN-1 36 mg fell well short of tirzepatide's 20.9%. Orforglipron's place in the obesity class lands roughly between liraglutide and injectable semaglutide on raw weight loss, with the access advantage of being an oral pill.
Bottom line: ATTAIN-1 confirmed orforglipron as a real GLP-1 effect, not a weak signal. The absolute weight loss is below injectable semaglutide and well below injectable tirzepatide, but it is the strongest oral GLP-1 number ever published.
ATTAIN-2: orforglipron in patients with comorbid type 2 diabetes
ATTAIN-2 ran the same 72-week design in adults with obesity and type 2 diabetes (ATTAIN-2, Lancet 2025).
Results at 36 mg, week 72:
- Mean weight reduction: 10.5% vs 2.2% with placebo
- HbA1c reductions ranged from 1.3 to 1.8 percentage points across active doses, from a baseline of 8.1%
The smaller percentage weight loss versus ATTAIN-1 mirrors the established class pattern. Patients with type 2 diabetes typically lose 2 to 4 percentage points less weight than non-diabetic patients on the same GLP-1 agonist, likely tied to differences in insulin signaling and energy homeostasis.
The HbA1c result is what makes this trial commercially important. A 1.8 percentage point drop from a baseline of 8.1% is comparable to what semaglutide 2.4 mg produces in similar populations. For an oral pill, that is competitive with the injectable category leader on glycemic control.
ACHIEVE-1: monotherapy in early type 2 diabetes
ACHIEVE-1 enrolled adults with early type 2 diabetes treated only by diet and exercise, no metformin or other agents (ACHIEVE-1, NEJM 2025).
Design:
- 40 weeks
- Doses: 3 mg, 12 mg, 36 mg, placebo (1:1:1:1)
- Baseline HbA1c 7.0 to 9.5%, BMI at least 23
HbA1c reduction (estimated mean difference vs placebo):
- 3 mg: -0.83 percentage points
- 12 mg: -1.06 percentage points
- 36 mg: -1.07 percentage points
Body weight change from baseline at week 40:
- 3 mg: -4.5%
- 12 mg: -5.8%
- 36 mg: -7.6%
- Placebo: -1.7%
The dose-response curve flattens between 12 mg and 36 mg on glycemic control but continues climbing on weight. That is consistent with the broader observation that GLP-1 weight effects scale further with exposure than glycemic effects, which tend to saturate earlier.
No severe hypoglycemia occurred, which matters for early T2D where preserving endogenous insulin response is the priority.
ACHIEVE-3: head-to-head against oral semaglutide
ACHIEVE-3 is the trial that recalibrates the oral GLP-1 lane (ACHIEVE-3, Lancet 2026).
Design:
- 52 weeks
- 1,698 adults with type 2 diabetes inadequately controlled on metformin
- Open-label, four arms (1:1:1:1): orforglipron 12 mg, orforglipron 36 mg, oral semaglutide 7 mg, oral semaglutide 14 mg
- Baseline HbA1c 8.3%
HbA1c change at week 52:
- Orforglipron 12 mg: -1.71 percentage points
- Orforglipron 36 mg: -1.91 percentage points
- Oral semaglutide 7 mg: -1.23 percentage points
- Oral semaglutide 14 mg: -1.47 percentage points
Estimated treatment differences (orforglipron minus oral semaglutide):
- 12 mg vs 7 mg: -0.48 percentage points
- 36 mg vs 14 mg: -0.44 percentage points
Both comparisons crossed non-inferiority and superiority margins. Weight reduction also favored orforglipron at both dose pairings.
The implications are practical. Oral semaglutide has been the only oral GLP-1 in commercial use since 2019. ACHIEVE-3 shows orforglipron beats it on glycemic control and weight at matched dose tiers, with no fasting or water restriction required. If the regulatory path runs as Lilly has guided, orforglipron will likely displace oral semaglutide in real-world prescribing within months of approval.
How orforglipron stacks up against the rest of the class in 2026
| Compound | Route | Class | Top weight loss in trial | HbA1c reduction (T2D) | Trial baseline | Approved? |
|---|---|---|---|---|---|---|
| Orforglipron | Oral, no food/water restriction | Small-molecule GLP-1 | 12.4% at 72 wk (ATTAIN-1, 36 mg) | -1.91 ppt at 52 wk (ACHIEVE-3) | HbA1c 8.3% | No (submissions filed 2025-2026) |
| Oral semaglutide (Rybelsus) | Oral, fasting + 30 min wait | Peptide GLP-1 | ~6 to 8% in PIONEER trials | -1.47 ppt at 52 wk (ACHIEVE-3, 14 mg) | HbA1c 8.3% | Yes (T2D, 2019) |
| Injectable semaglutide (Wegovy/Ozempic) | Injection, weekly | Peptide GLP-1 | 14.9% at 68 wk (STEP 1, 2.4 mg) | -1.6 to -1.8 ppt | varies | Yes |
| Tirzepatide | Injection, weekly | GIP/GLP-1 dual | 20.9% at 72 wk (SURMOUNT-1, 15 mg) | -2.0 to -2.4 ppt | varies | Yes |
| Retatrutide | Injection, weekly | GIP/GLP-1/glucagon triple | 24.2% at 48 wk (Phase 2, 12 mg) | -2.0+ ppt (Phase 2) | varies | No (Phase 3 ongoing) |
The numbers above use the highest dose in each landmark trial. Cross-trial comparisons are imperfect (different baselines, durations, populations), so treat the table as a frame of reference rather than a strict ranking.
Side effects: same class, similar profile
ATTAIN-1 reported the gastrointestinal pattern that defines the GLP-1 class:
- Nausea: 28.9% (6 mg), 35.9% (12 mg), 33.7% (36 mg) vs 10.4% (placebo)
- Constipation: 21.7%, 29.8%, 25.4% vs lower single-digit rates on placebo
- Treatment discontinuation due to adverse events: 5.3 to 10.3% on active doses vs 2.7% on placebo
Most events were mild to moderate and concentrated during the dose-escalation window. The absolute discontinuation rates sit in the same range as published numbers for tirzepatide in SURMOUNT-1 and semaglutide in STEP 1.
For researchers tracking real-world tolerability, two specifics matter. Oral GLP-1 nausea appears not to be lower than injectable, despite the prior intuition that smoother PK might smooth out side effects. And the dose-escalation schedule used in the Phase 3 trials (slow titration over roughly 12 to 16 weeks) appears to be necessary for tolerability, not a marketing-driven schedule.
Warning: The same class warning about thyroid C-cell tumors that applies to peptide GLP-1 agonists, based on rodent carcinogenicity work, is expected to apply here. Personal or family history of medullary thyroid carcinoma or MEN2 was an exclusion in the published trials.
What is not yet known
Cardiovascular outcomes. ATTAIN and ACHIEVE measured surrogate cardiometabolic markers but neither was a dedicated cardiovascular outcomes trial. The cardiovascular outcomes program is enrolling and will read out later. Until then, orforglipron does not have the cardiovascular outcomes evidence semaglutide built through SUSTAIN-6 and SELECT.
Long-term durability. Trials run 40 to 72 weeks. Real-world durability beyond two years has not been characterized. The same caveat applies to muscle preservation, which has emerged as a meaningful concern for the GLP-1 class generally. See GLP-1 muscle loss research for the broader context.
MASH and liver. Lilly has signaled intent to develop orforglipron for steatohepatitis (MASH), but no Phase 3 readout has been published in that indication.
Regulatory status. As of May 2026, Lilly has filed global submissions across multiple regions, but orforglipron is not yet approved or commercially available in the United States. Compounding pharmacies cannot legally compound it, and any product marketed as orforglipron from research-grade vendors is not the actual molecule. Because orforglipron is a Lilly-proprietary small molecule rather than a peptide, it cannot be synthesized through standard peptide manufacturing.
That last point is worth emphasizing. Researchers cannot meaningfully access orforglipron outside Lilly's clinical trials and post-approval supply chain. Any vial or capsule sold under the orforglipron name from a peptide vendor is, at best, mislabeled.
Where orforglipron fits in the 2026 GLP-1 lineup
Three tiers of efficacy have emerged across the class.
The top tier on weight loss is retatrutide and tirzepatide, both injectable. Retatrutide produced 24.2% mean weight loss in its Phase 2 readout at 48 weeks. Tirzepatide produced 20.9% in SURMOUNT-1 at 72 weeks. These set the current ceiling.
The middle tier is injectable semaglutide and orforglipron. Injectable semaglutide 2.4 mg produced 14.9% in STEP 1. Orforglipron 36 mg produced 12.4% in ATTAIN-1. The gap is real but narrower than expected given the route difference.
The bottom tier is oral semaglutide and earlier injectables (liraglutide), with weight loss in the 6 to 9% range.
If access matters more than peak efficacy, orforglipron will likely shift the center of gravity in the oral lane. If peak efficacy matters more, retatrutide and tirzepatide remain the leaders.
For research compounds in the metabolic lane, Ascension Peptides ships research-grade tirzepatide, semaglutide, and retatrutide for injectable comparison work, with 50% off using code ENHANCED. Limitless Biotech sells oral metabolic capsules including 5-Amino-1MQ and tesofensine for adjacent research lanes, with code ENHANCED. Orforglipron itself is not available outside Lilly's clinical supply.
Bottom line
Bottom line: Orforglipron is a real GLP-1 effect in a non-peptide oral pill with no food or water restrictions. It is below injectable tirzepatide on weight loss and HbA1c, but it beats oral semaglutide head-to-head in ACHIEVE-3 and matches the class on cardiometabolic markers. If Lilly's regulatory submissions clear in 2026 to 2027, the oral GLP-1 lane gets rebuilt around this molecule.
The most defensible reading is that orforglipron does for oral GLP-1s what tirzepatide did for the dual-agonist concept. It moves the lane forward by enough to retire most of what came before it. The pharmacology improvement is concrete and the access advantage is real. Hard numbers, not marketing language, are doing the work.
For full context on where orforglipron sits in the broader Phase 2 record, see the original Phase 2 obesity readout (14.7% mean reduction at 36 weeks, Wharton et al. NEJM 2023) and the Phase 2 type 2 diabetes readout (Frias et al. Lancet 2023). Both informed the Phase 3 dose selection above.
Related research on this site
- Tirzepatide vs Semaglutide (2026)
- Retatrutide vs Tirzepatide vs Semaglutide (2026)
- Retatrutide explained: the triple agonist
- Stopping GLP-1 weight regain research
- GLP-1 muscle loss and lean mass preservation
- Semaglutide and alcohol use disorder research
- Tirzepatide and sleep apnea (SURMOUNT-OSA)
- Semaglutide research page
- Tirzepatide research page
- Retatrutide research page
- Reconstitution Calculator
This article is for educational and research purposes only. It is not medical advice. Orforglipron is an investigational oral GLP-1 receptor agonist developed by Eli Lilly and is not FDA-approved as of May 2026. Trial results summarized here describe what was measured under controlled clinical conditions and do not establish efficacy or safety for any specific individual outside of those trials. Class-wide GLP-1 risks including pancreatitis, gallbladder disease, severe gastrointestinal adverse events, and the rodent-model thyroid C-cell tumor signal apply broadly to GLP-1 receptor agonists; the long-term safety of orforglipron specifically is not yet characterized beyond the Phase 3 trial windows. Doses and schedules summarized here describe what the published literature tested; they are not protocols and do not constitute a recommendation.