At a glance
- Oral ghrelin mimetic with ~24-hour half-life; no injections needed
- 25 mg daily restored IGF-1 to young-adult levels in elderly within 4 weeks
- Stage IV deep sleep increased ~50% in polysomnography studies
- 67% of users report increased appetite; bedtime dosing mitigates this
- Modest fasting glucose increase (~5 mg/dL); monitor HbA1c every 3-6 months
One capsule. No needles. No reconstitution. No math.
MK-677 (ibutamoren) raised IGF-1 levels in elderly subjects to those of healthy young adults within four weeks. One pill a day, taken at bedtime. No subcutaneous injections. No bacteriostatic water. No 29-gauge insulin syringes.
That single data point, from Chapman et al. (1996) at the University of Virginia, is why MK-677 sits in a category of its own among growth hormone secretagogues. But the full picture is more nuanced than any supplement brand wants you to believe.
Here is what the clinical trials actually show, where the compound falls short, and how to decide whether it belongs in your protocol.
MK-677 is not a peptide (and that matters)
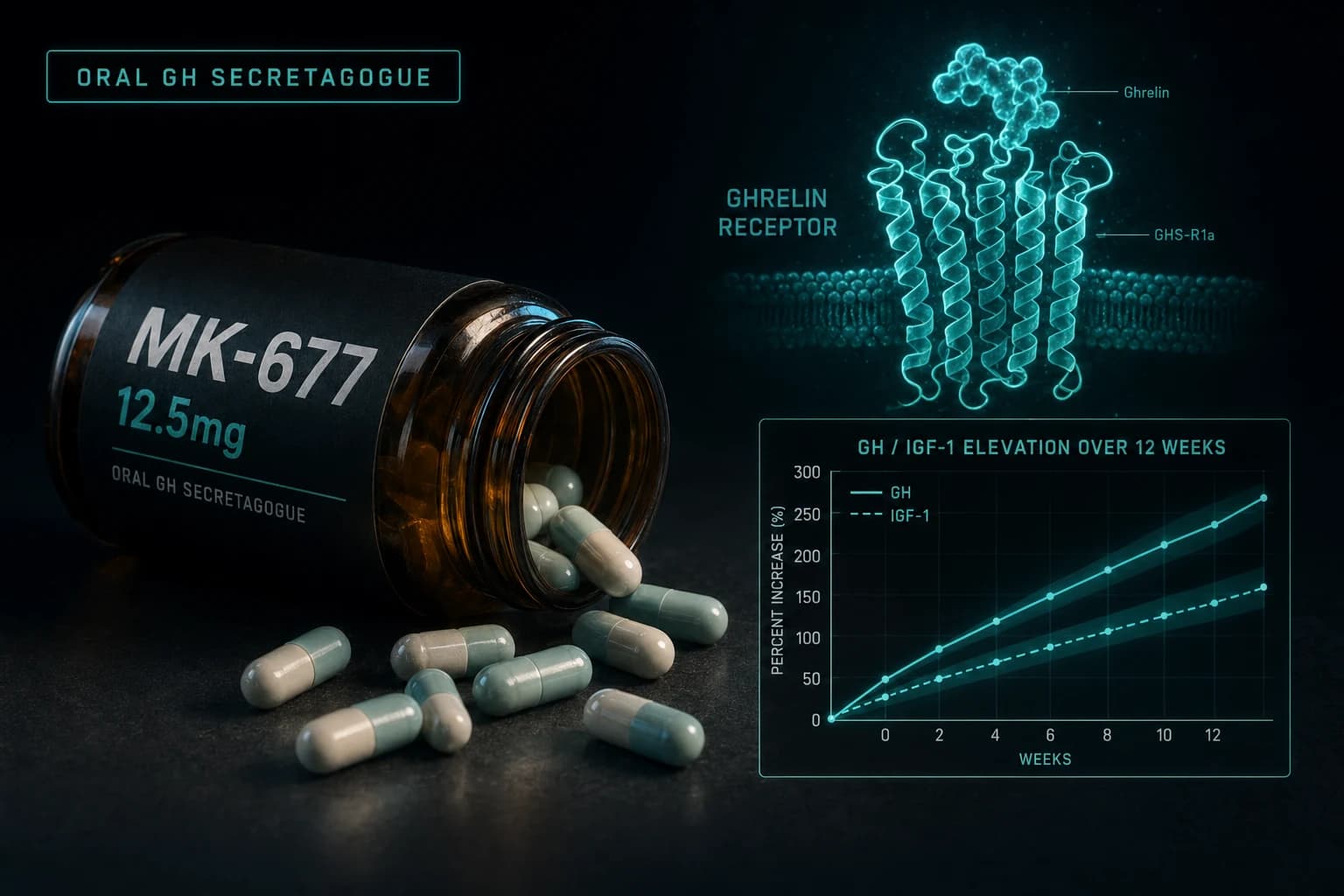
First, a classification issue that most sites get wrong. MK-677 is not a peptide. It is a non-peptide spiropiperidine, a small molecule designed to mimic the structure of ghrelin (your body's hunger hormone) well enough to activate the same receptor: GHS-R1a (growth hormone secretagogue receptor type 1a).
Why does this distinction matter? Peptides like CJC-1295 and ipamorelin are chains of amino acids. They get destroyed by stomach acid and digestive enzymes, which is why they require subcutaneous injection. MK-677's non-peptide structure resists proteolysis entirely, allowing oral absorption through the GI tract.
Think of it this way: ghrelin is the key your body makes. Injectable GHRPs like ipamorelin are a copy of that key, fragile enough that you have to sneak it past the front door (inject it under the skin). MK-677 is a lockpick, a completely different shape that still turns the same tumbler.
The structural biology confirms this. Cryo-EM imaging published in Nature Communications shows that ibutamoren occupies the same binding pocket as ghrelin's first four amino acid residues, including the octanoyl chain, but does so using a completely different molecular scaffold (Liu et al., 2021).
How MK-677 works: the GHS-R1a pathway
When MK-677 binds GHS-R1a receptors in the hypothalamus and anterior pituitary, it triggers pulsatile growth hormone release. This is the same mechanism your body uses during deep sleep and intense exercise.
Three things happen downstream:
- GH pulses increase in both frequency and amplitude. Your pituitary releases more growth hormone per pulse, and fires more often.
- IGF-1 rises over days to weeks. The liver converts circulating GH into IGF-1 (insulin-like growth factor 1), which drives most of the anabolic and recovery effects people associate with growth hormone.
- The negative feedback loop stays intact. Unlike exogenous GH injections (which suppress your own production), MK-677 works through endogenous signaling. Your hypothalamic-pituitary axis still regulates the process, so you do not get the supraphysiological spikes that come with injecting recombinant GH.
One critical nuance: because MK-677 activates ghrelin receptors throughout the body (not just in the pituitary), it also stimulates appetite, raises cortisol modestly, and affects insulin sensitivity. These are not bugs. They are direct pharmacological consequences of the mechanism. More on that in the side effects section.
Pharmacokinetics: why once-daily dosing works
The pharmacokinetic profile of MK-677 is what separates it from every injectable GH secretagogue on the market.
| Parameter | MK-677 (Ibutamoren) | Ipamorelin | CJC-1295 (DAC) |
|---|---|---|---|
| Route | Oral | Subcutaneous | Subcutaneous |
| Tmax | ~1 hour | ~15-30 min | ~2 hours |
| Half-life | ~24 hours | ~2 hours | ~6-8 days |
| Dosing frequency | Once daily | 1-3x daily | 1-2x weekly |
| Reconstitution needed | No | Yes | Yes |
The ~24-hour elimination half-life means a single daily dose maintains steady-state plasma concentrations. Peak GH secretion occurs within 1-2 hours of oral administration, but the compound keeps working around the clock, amplifying your natural overnight GH pulses as well.
For a deeper look at how half-life affects dosing decisions, see our half-life calculator.
Clinical evidence: what the trials actually found
MK-677 has more human clinical data than most compounds in the peptide space. Here are the key studies, with actual numbers.
Murphy et al. (1998): reversing diet-induced catabolism
Murphy et al. (1998) ran a double-blind, placebo-controlled crossover trial in 8 healthy volunteers (ages 24-39) placed on a calorie-restricted diet (18 kcal/kg/day) for 14 days. During the second week, 25 mg daily MK-677 reversed the nitrogen loss seen with caloric restriction.
The numbers: nitrogen balance was +0.31 g/day with MK-677 versus -1.48 g/day with placebo. Mean IGF-1 rose to 264 ng/mL (vs. 188 ng/mL on placebo). Translation: MK-677 protected lean mass during a cut, suggesting utility for anyone running a caloric deficit who wants to preserve muscle.
Svensson et al. (1998): obese males, 8 weeks
Svensson et al. (1998) studied 24 obese males (BMI > 30) given 25 mg MK-677 or placebo daily for 8 weeks. Fat-free mass increased significantly in the MK-677 group (measured by both DEXA and four-compartment modeling, p < 0.01). IGF-1 increased approximately 40% (p < 0.001 vs. placebo). Total and visceral fat did not change significantly.
Nass et al. (2008): the 12-month landmark trial
The longest and most rigorous MK-677 trial, Nass et al. (2008), followed 65 healthy older adults (ages 60-81) for up to two years. Daily 25 mg MK-677 produced these 12-month results:
- Fat-free mass: increased 1.1 kg with MK-677 vs. decreased 0.5 kg with placebo (p < 0.001)
- GH and IGF-1: restored to levels of healthy young adults
- Strength and function: no significant change (the extra lean mass did not translate to measurable strength gains)
- Fasting glucose: increased ~5 mg/dL on average (statistically significant but clinically modest)
- Cortisol: increased 47 nmol/L in MK-677 recipients
The strength finding is worth pausing on. MK-677 reliably adds lean tissue, but the tissue itself does not appear to automatically improve performance in older adults. Resistance training alongside the compound may be necessary to realize functional gains.
Sleep quality: the underrated benefit
This might be the most practically relevant finding for daily users. Copinschi et al. (1997) conducted a double-blind, placebo-controlled sleep study in young (18-30) and older adults using polysomnography (the gold standard for sleep measurement).
In young subjects taking 25 mg MK-677 at bedtime:
- Stage IV (deep sleep) duration increased ~50% (p < 0.05)
- REM sleep increased > 20% (p < 0.05)
- Deviations from normal sleep architecture dropped from 42% to 8% (p < 0.03)
In older adults, REM sleep increased nearly 50% (p < 0.05) with decreased REM latency (p < 0.02).
Stage IV sleep is when your body does its heaviest repair work. More deep sleep means better recovery, better consolidation of motor learning, and stronger immune function. Many users report that improved sleep is the first noticeable effect within the first week, before any body composition changes become apparent.
This is also why bedtime dosing is the standard protocol. You align the compound's peak GH secretory effect with your natural overnight GH pulses, and you get the appetite spike while you are asleep instead of fighting cravings all day.
Side effects: the honest breakdown
Every site that tells you MK-677 is side-effect-free is selling you something. The clinical data is clear about the trade-offs.
Appetite increase (the big one)
In the Nass 2008 trial, 67% of MK-677 users reported increased appetite (vs. 36% on placebo). This is a direct consequence of activating the ghrelin receptor. You are literally taking a hunger hormone mimetic.
The good news: in 50% of subjects, appetite returned to baseline within 3 months. The body appears to partially adapt. Bedtime dosing helps significantly, because the strongest appetite surge hits while you are asleep or heading to sleep.
Water retention
Mild, transient lower-extremity edema was the most common adverse event in clinical trials. Growth hormone increases sodium and water retention at the kidney level. Most users report 2-5 pounds of water weight in the first 2-4 weeks, which stabilizes or resolves.
This is cosmetic, not dangerous, for most people. But if you have hypertension or heart failure risk factors, the fluid shift matters.
Insulin resistance and fasting glucose
This is the side effect that deserves the most respect. Both the Nass 2008 and the Svensson 1998 data show modest but real increases in fasting blood glucose (~5 mg/dL average) and insulin resistance. HbA1c increased slightly but significantly at 12 months.
At 25 mg daily, the effect is small for metabolically healthy individuals. At higher doses (50 mg), or in people who already have impaired glucose tolerance, the risk of clinically meaningful insulin resistance increases. This is why monitoring fasting glucose and HbA1c every 3-6 months is strongly recommended for anyone running MK-677.
Cortisol elevation
Cortisol increased 47 nmol/L in the Nass trial. This is a modest bump, well within normal range, but it is nonzero. If you are already running a high-stress protocol or have cortisol issues, factor this in.
What about cancer risk?
IGF-1 is a growth factor. It promotes cell growth indiscriminately, including potentially cancerous cells. There is no clinical evidence that MK-677 causes cancer, but elevated IGF-1 is associated with increased risk in epidemiological studies. Anyone with a personal or family history of hormone-sensitive cancers should discuss this with their physician before using any GH secretagogue.
Dosing: what the research supports
| Dose | Use case | Notes |
|---|---|---|
| 10-12.5 mg/day | Conservative start, sleep optimization | Well-tolerated, modest GH/IGF-1 increase, minimal side effects |
| 25 mg/day | Standard research dose | Most clinical data exists at this level. Best balance of efficacy and tolerability |
| 50 mg/day | Aggressive (not recommended) | Diminishing returns on IGF-1 with substantially more side effects (insulin resistance, edema) |
Timing: Bedtime, 30-60 minutes before sleep. Aligns peak GH secretion with natural sleep-related GH pulses. Minimizes appetite disruption during waking hours.
Cycle length: Clinical trials ran 8 weeks to 2 years continuously. There is no established consensus on cycling. Some researchers run 8-12 week cycles with 4-week breaks. Others run it continuously with periodic blood work (fasting glucose, IGF-1, HbA1c) every 3 months.
Empty stomach vs. with food: The pharmacokinetic data shows rapid absorption regardless, but some users report less GI discomfort when taken with a small meal. Clinical trials did not standardize this.
MK-677 vs. CJC-1295 + Ipamorelin: choosing your path
This is the comparison most people are actually trying to make. Both approaches elevate GH and IGF-1 through endogenous stimulation. The trade-offs are real.
| Factor | MK-677 (oral) | CJC-1295 + Ipamorelin (injectable) |
|---|---|---|
| Administration | Swallow a capsule | Reconstitute, draw, inject subcutaneously |
| Frequency | Once daily | CJC-1295 DAC: 1-2x/week; Ipamorelin: 1-3x/day |
| Appetite increase | Significant (ghrelin receptor) | Minimal (ipamorelin is selective for pituitary GHS-R) |
| Cortisol effect | Modest increase | Ipamorelin has minimal cortisol/prolactin impact |
| Insulin sensitivity | Moderate negative effect | Minimal at standard doses |
| Sleep benefit | Well-documented (50% increase in stage IV) | Anecdotally reported, less clinical data |
| Cost per month | $40-80 (oral capsules) | $80-150+ (peptides + supplies) |
| Clinical data volume | Extensive (multiple RCTs, up to 2 years) | Moderate (shorter trials, often separate compounds) |
| Convenience | High | Low (cold chain, reconstitution, injection) |
Choose MK-677 if: You want simplicity, you value the sleep data, you do not mind managing appetite, and you are metabolically healthy. It is particularly well-suited for a first GH secretagogue experience because there is zero injection learning curve.
Choose CJC-1295 + Ipamorelin if: You want cleaner GH elevation without appetite stimulation, you are comfortable with injections, or you have insulin sensitivity concerns. The Fit Stack protocol covers this combination in detail.
Some researchers run both, using MK-677 at a lower dose (10-12.5 mg) for the sleep benefits alongside a CJC-1295/Ipamorelin stack for the GH elevation. This is an advanced approach that requires monitoring.
For a broader comparison of oral vs. injectable formats across all peptides, see our oral peptides guide.
Who MK-677 is for (and who it is not for)
Good candidates:
- Researchers interested in GH optimization who want to avoid injections entirely
- People prioritizing sleep quality improvement alongside body composition goals
- Those in a caloric deficit who want to protect lean mass (Murphy 1998 data)
- First-time GH secretagogue users who want the simplest possible protocol
Think twice if you have:
- Pre-diabetes or impaired glucose tolerance (insulin resistance risk)
- A history of or active hormone-sensitive cancers (elevated IGF-1)
- Congestive heart failure or significant edema risk (fluid retention)
- Difficulty controlling food intake (the appetite increase is substantial and lasts 1-3 months)
Where to source MK-677
Because MK-677 is an oral compound, it is available as capsules, which eliminates the reconstitution and cold storage requirements of injectable peptides. Available from Limitless Biotech in oral capsule form with code ENHANCED at checkout.
For the full breakdown of MK-677 compound data, dosing references, and stacking options, see the compound page.
This article is for educational and informational purposes only. MK-677 (ibutamoren) is not approved by the FDA for human use. All dosing information is derived from published clinical research and is intended for research purposes only. Consult a qualified healthcare professional before making any decisions about peptide research or supplementation.