At a glance
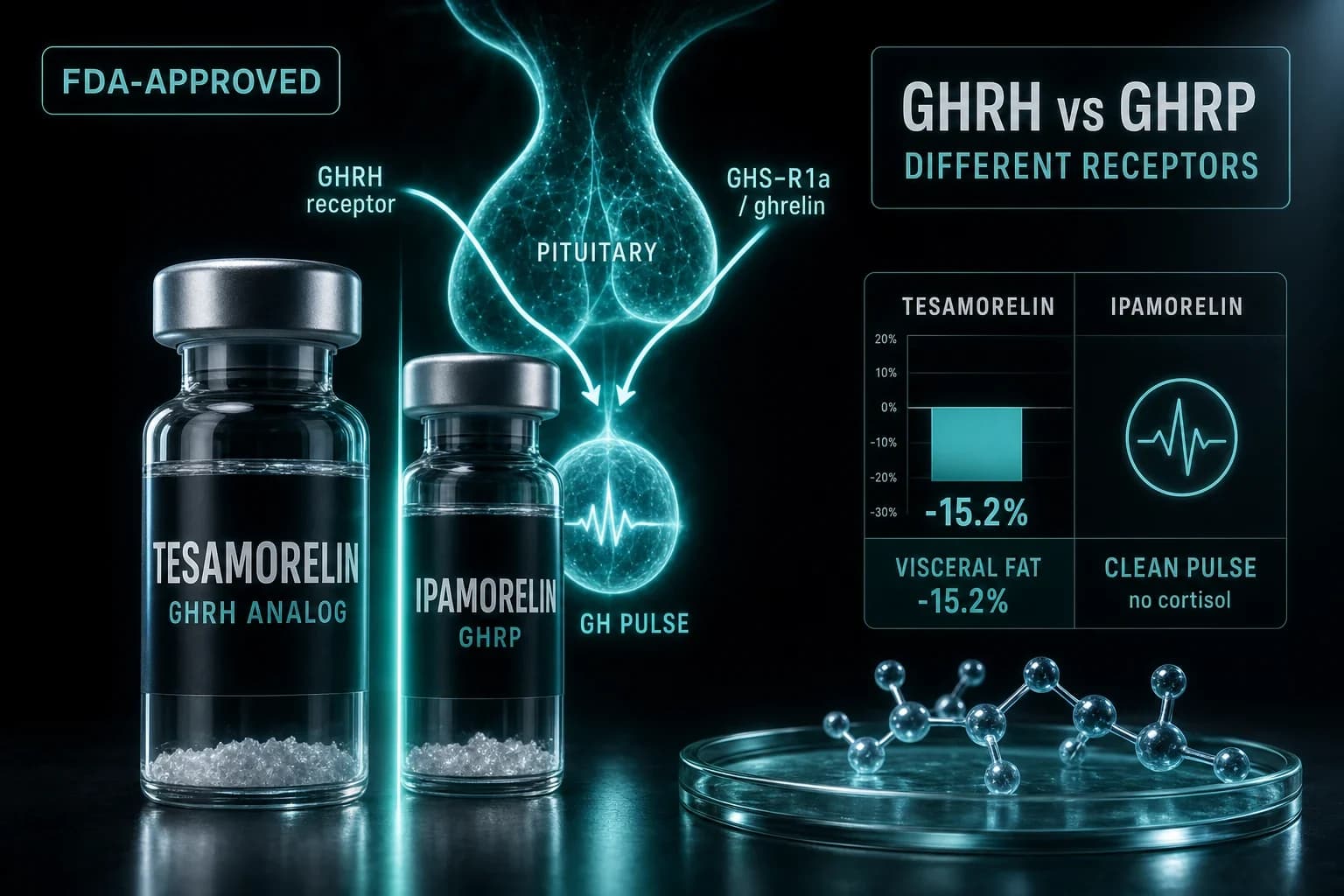
- Tesamorelin is a GHRH analog; ipamorelin is a selective ghrelin-mimetic GHRP. Different receptors.
- Tesamorelin cut visceral fat 15.2% in HIV lipodystrophy (Falutz 2007). It is FDA-approved.
- Ipamorelin raises GH without spiking cortisol or prolactin, even at 200x its ED50 (Raun 1998).
- They are not either/or: GHRH plus GHRP hit separate receptors and stack synergistically.
- Ipamorelin half-life is roughly 2 hours; tesamorelin peaks fast and clears within ~30 minutes.
Tesamorelin cut visceral fat by 15.2% in a Phase 3 trial while placebo patients gained 5%. Ipamorelin, in its founding study, raised growth hormone without touching cortisol or prolactin at doses 200 times higher than the threshold for GH release. Both are growth-hormone peptides. That is where the similarity ends.
If you are comparing these two, you are probably being told they are interchangeable "GH peptides." They are not. They act on different receptors, chase different outcomes, and one of them is actually approved by the FDA. Here is how they split.
The core mechanistic difference
Your pituitary releases growth hormone on two signals. GHRH (growth hormone-releasing hormone) tells it to make and release GH. Ghrelin, working through a separate receptor, amplifies that pulse and blunts somatostatin, the brake pedal on GH.
Tesamorelin is a stabilized GHRH analog. It is a modified version of the natural releasing hormone, engineered with a trans-3-hexenoic acid group so it survives in the bloodstream longer than native GHRH. It pushes the "make GH" signal.
Ipamorelin is a GHRP, a growth hormone-releasing peptide that mimics ghrelin at the GHS-R1a receptor. It presses the accelerator on the ghrelin side. Older GHRPs like GHRP-6 did this dirtily, dragging cortisol, prolactin, and hunger up with the GH. Ipamorelin was the first one selective enough to leave those alone. In the founding rat and pig work, Raun et al. (1998) showed it released GH with a selectivity "similar to that displayed by GHRH" and no significant rise in ACTH, cortisol, FSH, LH, prolactin, or TSH, even at 200x the ED50 for GH.
Two switches, two locations. That single fact drives everything below, including why researchers often run them together instead of picking one.
Tesamorelin: the one with an approval
Tesamorelin is the only peptide in this comparison that carries an FDA indication. It is approved (as Egrifta) to reduce excess visceral abdominal fat in HIV patients with lipodystrophy, a real condition where fat accumulates viscerally around the organs.
The pivotal data are specific. In the Phase 3 trial reported by Falutz et al. (2007), patients on 2 mg daily saw visceral adipose tissue fall 15.2% over 26 weeks, while the placebo group's VAT rose 5.0%. Triglycerides dropped and IGF-1 rose without meaningful loss of subcutaneous fat, which matters because visceral fat is the metabolically dangerous kind wrapped around your liver and gut.
The mechanism is clean: tesamorelin restores a more youthful GHRH signal, the pituitary releases GH in a natural pulsatile pattern, and elevated GH drives lipolysis preferentially in visceral depots. It is not a general "recomp" peptide. Its documented strength is one thing, visceral fat, and it does that thing better than anything else in the class.
Bottom line: If the target is visceral abdominal fat and you want the compound with actual regulatory approval and Phase 3 numbers behind it, tesamorelin is the GHRH analog with the receipts.
Full compound details are on the tesamorelin peptide page, and protocol-level dosing lives on the tesamorelin dosage chart.
Ipamorelin: the clean pulse
Ipamorelin does not have a headline body-composition trial. What it has is the cleanest side-effect profile in the GHRP family, and that is precisely why researchers reach for it.
The pitch is a strong, natural-shaped GH pulse without the collateral hormones. No cortisol spike means no stress-hormone drag on recovery or sleep. No prolactin rise means none of the associated side effects that plague dirtier secretagogues. No significant hunger surge, unlike GHRP-6. This is the selectivity Raun et al. (1998) built the molecule around.
Because the pulse mimics natural ghrelin timing, ipamorelin is favored for recovery and sleep-quality contexts, where the goal is nudging GH output back toward a younger baseline rather than flooding the system. It is the GHRP most often paired with a GHRH partner. See the ipamorelin peptide page for the full breakdown.
Why they are combined, not compared
Here is the part most "X vs Y" articles miss. Tesamorelin and ipamorelin hit different receptors, so their effects are additive, sometimes synergistic. Fire the GHRH switch and the GHRP switch at the same time and you get a larger GH pulse than either alone, because you are simultaneously pushing the accelerator and releasing the somatostatin brake.
In practice, the more common pairing is a GHRH like CJC-1295 with ipamorelin, because CJC-1295 is purpose-built for the stacking role. Teichman et al. (2006) showed a single dose of CJC-1295 produced dose-dependent GH increases lasting six or more days and elevated IGF-1 for 9 to 11 days. That long tail pairs neatly with ipamorelin's short, sharp pulse. Tesamorelin can play the GHRH role too, but its clinical identity is so tied to visceral fat that most stacking protocols default to CJC-1295. The mechanics of that trio are covered in our sermorelin vs CJC-1295 vs ipamorelin comparison.
If your interest is body composition and lean mass rather than the visceral-fat indication specifically, the best peptides for muscle growth guide maps where each of these fits.
Side by side
| Feature | Tesamorelin | Ipamorelin |
|---|---|---|
| Class | Stabilized GHRH analog | Selective GHRP (ghrelin-mimetic) |
| Receptor | GHRH receptor | GHS-R1a (ghrelin receptor) |
| FDA status | Approved (HIV lipodystrophy, visceral fat) | Not approved; research use only |
| Best documented for | Visceral fat reduction (15.2%, Falutz 2007) | Clean GH pulse, recovery, sleep contexts |
| Cortisol / prolactin | Not the concern; GHRH-type signal | No significant rise, even at 200x ED50 |
| Half-life | Short; clears within ~30 minutes | Roughly 2 hours |
| Typical research dose | ~1-2 mg daily, subcutaneous | ~200-300 mcg per dose, 1-3x daily |
| Usual role | Standalone, visceral-fat target | Stacked with a GHRH (e.g. CJC-1295) |
Dosing and half-life in practice
Tesamorelin's clinical protocol is straightforward: the approved regimen is 2 mg subcutaneously once daily. It peaks quickly and clears fast, which is why it is dosed daily rather than pulsed multiple times.
Ipamorelin runs shorter per molecule but is often dosed more frequently, commonly around 200 to 300 mcg per injection, once to three times daily, timed around workouts and before bed to ride the natural nocturnal GH rise. Its roughly two-hour half-life means the pulse is done well before the next one, preserving the pulsatility your pituitary expects.
Both are reconstituted from lyophilized powder, and getting the concentration right is where most dosing errors happen. Our reconstitution calculator converts your vial size and bacteriostatic water volume into exact units on the syringe so you are not guessing.
Warning: Growth-hormone peptides are not a free lunch. Elevated GH and IGF-1 can raise blood glucose, cause water retention, and produce joint aches or carpal-tunnel-type symptoms. Tesamorelin carries specific contraindications around active malignancy. This is why bloodwork matters.
The honesty section
Peptide marketing loves to imply these compounds turn back the clock. The evidence says be careful. Liu et al. (2007) systematically reviewed growth hormone in healthy elderly adults across 18 studies and found the antiaging case unconvincing: modest lean-mass changes came bundled with higher rates of soft-tissue edema, joint pain, and glucose intolerance. GH is a real tool for real deficiencies, not a lifestyle upgrade for people whose GH is already normal.
That framing separates the two peptides cleanly. Tesamorelin has a defined medical target and Phase 3 data proving it hits that target. Ipamorelin has an excellent safety and selectivity profile but no equivalent outcome trial, so its use rests more on mechanism and researcher experience than on a landmark result.
Anyone running either compound should track IGF-1, fasting glucose, and HbA1c before and during use. A baseline and follow-up panel through at-home lab tests is the single most responsible step in any GH-peptide protocol, and it is the step most people skip.
So which one
Choose based on the endpoint, not the hype.
Pick tesamorelin if the goal is visceral abdominal fat and you want the compound with an FDA indication and Phase 3 numbers. Pick ipamorelin if you want a clean, selective GH pulse for recovery and sleep contexts, and expect to stack it with a GHRH partner like CJC-1295 rather than run it solo. And recognize that for many research protocols the answer is not one or the other. Two receptors, two switches, one combined pulse.
Research-grade tesamorelin and ipamorelin are available from Ascension Peptides at 50% off with code ENHANCED, supplied for laboratory and research use only.
This article is for research and educational purposes only. None of these compounds are approved for the uses described here, with the sole exception of tesamorelin's FDA indication for HIV-associated lipodystrophy. Nothing here is medical advice. Consult a qualified physician before making any health decision.