At a glance
- Semaglutide 2.4 mg alone in COURAGE cut fat 15.7% and lean mass 6.5% at 26 weeks, with about a third of weight loss from lean tissue.
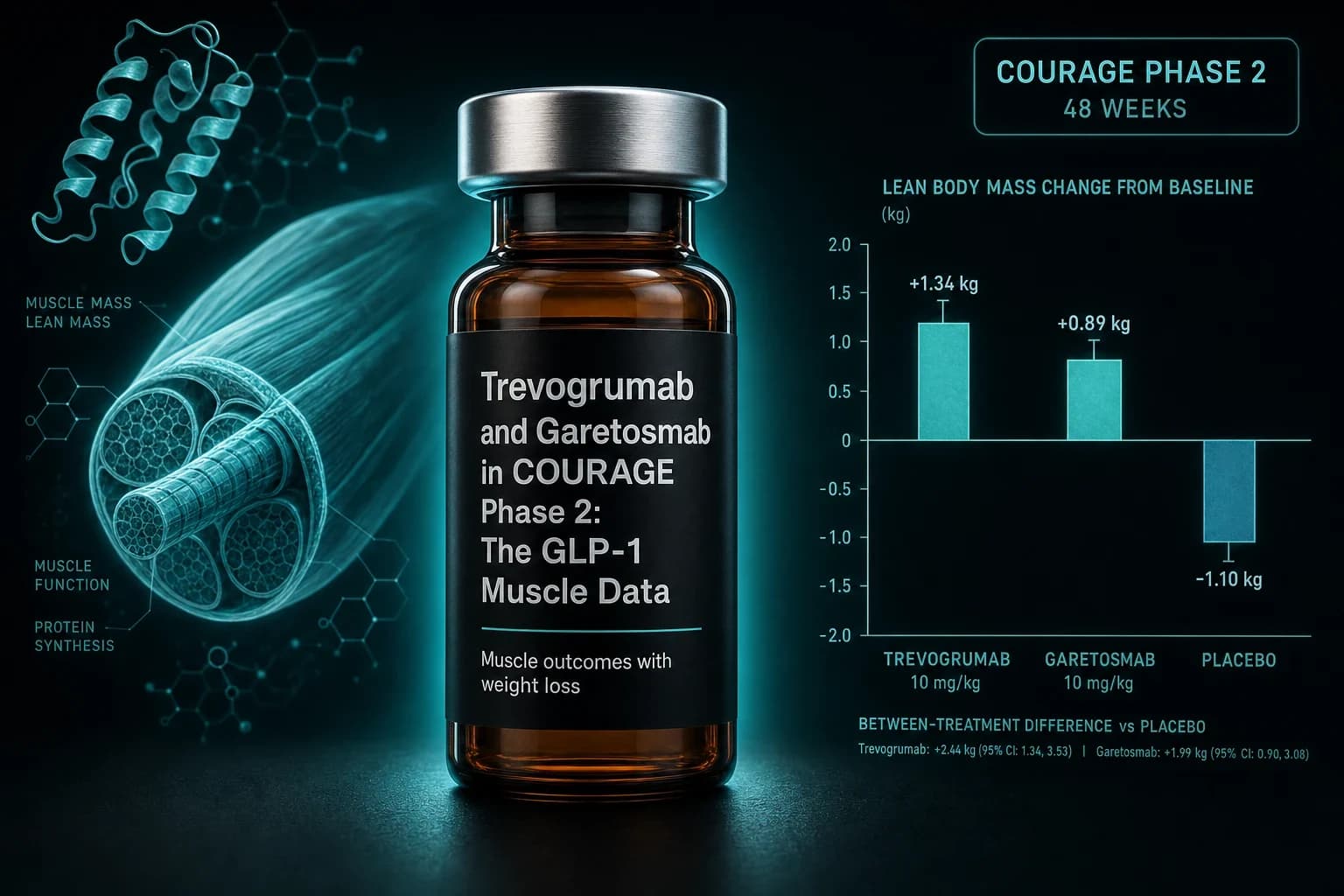
- Adding trevogrumab 400 mg (anti-GDF8/myostatin) attenuated lean mass loss to roughly 3.3-3.8% and pushed fat reduction up to 19.1%.
- The triplet with garetosmab (anti-activin A) hit 27.1% fat loss and only 2.0% lean loss, but two deaths occurred in that arm.
- Regeneron's Phase 1 in postmenopausal females (Gonzalez Trotter 2025, PMID 40360471) already showed the antibody pair adds muscle while shedding fat.
- Full COURAGE results and the maintenance phase read out late 2026; no myostatin or activin A antibody is FDA-approved for GLP-1 muscle preservation.
Semaglutide's Phase 3 numbers rewrote obesity medicine. The body composition numbers kept prescribers up at night. About a third of every kilogram lost on semaglutide came off as lean tissue, and no approved combination changed that ratio. Regeneron's Phase 2 COURAGE trial pairs semaglutide with two monoclonal antibodies to see if the ratio actually is fixed. The 26-week interim results say it is not. The safety numbers say to wait for more data before celebrating.
What COURAGE is actually testing
COURAGE (NCT06299098) is a randomized, double-blind Phase 2 trial that combines semaglutide 2.4 mg with two Regeneron antibodies:
- Trevogrumab (REGN1033) is a fully human IgG4 monoclonal against myostatin, also called growth differentiation factor 8 (GDF8). Myostatin is the endogenous brake on skeletal muscle mass. Blocking it releases the brake.
- Garetosmab is an IgG4 monoclonal against activin A, a related TGF-beta family ligand that signals through the same receptor as myostatin. Activin A restricts muscle in a partly overlapping and partly independent way.
The full cohort runs at roughly 1,000 adults aged 18 to 80 with obesity. Treatment splits into a 26-week weight-loss phase and a 26-week weight-maintenance phase. During weight loss, participants were randomized across four arms:
- Semaglutide 2.4 mg alone
- Semaglutide + trevogrumab 200 mg
- Semaglutide + trevogrumab 400 mg
- Semaglutide + trevogrumab 400 mg + garetosmab 10 mg/kg (the "triplet")
Interim 26-week data landed in a Regeneron release in June 2025 and got a full presentation at the European Association for the Study of Diabetes (EASD) meeting in September 2025. The maintenance phase and full safety analysis were still enrolling at that point.
Because this is Phase 2 and interim, the composition numbers below come from Regeneron's release and conference deck. There is no peer-reviewed COURAGE manuscript yet. Everything you can currently verify against a PubMed record is either the Phase 1 safety trial in postmenopausal females, the preclinical mechanism papers that led into COURAGE, or the Phase 3 trials of semaglutide and tirzepatide alone that supply the comparison baseline.
The 26-week interim numbers
| Arm | Reported weight loss | Fat mass change | Lean mass change | Fraction of loss from lean tissue |
|---|---|---|---|---|
| Semaglutide 2.4 mg alone | ~10.1% | −15.7% | −6.5% | ~33% |
| Sema + trevogrumab 400 mg | Higher than sema alone | Up to −19.1% | −3.3% to −3.8% | Roughly half the sema-alone lean loss |
| Sema + trevogrumab + garetosmab (triplet) | Highest across arms | −27.1% | −2.0% | Over 80% of lean mass preserved vs sema alone |
Source: Regeneron June 2025 interim release and EASD 2025 presentation. Fat and lean mass percentages are DXA-measured change from baseline. Neither the underlying dataset nor a peer-reviewed COURAGE manuscript is available yet.
Read left to right, the story is a shift in what gets lost, not a slowdown in how much. Semaglutide alone still moved the scale. Adding trevogrumab pushed a larger share of the change into adipose tissue while sparing skeletal muscle. Adding garetosmab pushed that further and preserved almost all lean mass. The tradeoff shows up in the safety column, which is where the story gets careful.
Bottom line: The COURAGE interim data is the first Phase 2 signal in humans that a myostatin plus activin A antibody combination substantially rebalances the composition of GLP-1-induced weight loss. That is a mechanism shift, not a body-composition rounding error.
Why myostatin blockade matters here
Myostatin/GDF8 restricts skeletal muscle mass across mammals. It is secreted mainly by muscle itself, binds activin receptor type IIB (ActRIIB), and drives Smad2/3 signaling downstream. Loss-of-function in cattle, whippets, and one documented human infant produces heavy muscling. Post-natal pharmacological blockade in adult animals reproduces the effect at a smaller scale.
Trevogrumab was built for that pathway. The founding paper by Latres and colleagues (Skeletal Muscle 2015, PMID 26457176) showed that chronic dosing in young mice increased fiber size, muscle mass, and force production. The same antibody prevented atrophy from immobilization, glucocorticoids, and hindlimb unweighting. In aged mice it raised muscle strength and treadmill performance. That was the pharmacology baseline: this specific antibody actually blocks myostatin at a dose that changes muscle in a living animal.
What was less clear until 2025 was how much of the muscle-restricting signal in humans was myostatin versus activin A, a related ligand that binds the same receptor. Adding an activin A antibody to a myostatin one tests whether both need to be blocked to fully release the brake. That is the biological question COURAGE's triplet arm is asking.
Why activin A too
Garetosmab is an IgG4 anti-activin A antibody originally developed for fibrodysplasia ossificans progressiva (FOP), a genetic disease where activin A drives ectopic bone formation. In the muscle context, activin A is another ActRIIB ligand that suppresses growth. Older receptor-body approaches like ACE-031 and bimagrumab blocked ActRII directly, catching all upstream ligands at once. A specific antibody like garetosmab catches only activin A and leaves the other TGF-beta ligands alone.
The Phase 1 trial by Gonzalez Trotter and colleagues (Nature Communications 2025, PMID 40360471) tested trevogrumab and garetosmab alone and together in healthy postmenopausal females at two New Zealand sites. Dual blockade produced larger increases in muscle mass than either antibody alone, and the muscle gains were accompanied by fat mass reductions. That was the first human-scale confirmation that GDF8 and activin A are both dominant, non-redundant negative regulators of muscle mass. It also justified spending trial slots on the triplet arm in COURAGE rather than sticking with trevogrumab monotherapy.
What the mouse and monkey data predicted
The preclinical work most directly relevant to COURAGE is Mastaitis and colleagues (Nature Communications 2025, PMID 40360507). In diet-induced obese male mice and in obese non-human primates, GLP-1 receptor agonism reduced body weight but also cut skeletal muscle mass. Dual blockade of GDF8 and activin A during GLP-1 therapy prevented the muscle loss, in some cases reversed it, and enhanced fat loss on top. In non-human primates, the combination also improved insulin sensitivity beyond what GLP-1 alone achieved.
The COURAGE 26-week numbers are the human echo of that animal pattern. That is not proof it will hold at 52 weeks or in Phase 3. The mechanism transferring across species is the strongest reason to take the interim numbers at face value while waiting for the maintenance data.
How this compares to bimagrumab
Bimagrumab is the only other Phase 2 muscle-preservation antibody with published GLP-1 combination data. It targets activin receptor type II directly rather than the individual ligands, so it catches every upstream signal at once. In the BELIEVE Phase 2 (Nature Medicine 2026, PMID 41772149), high-dose bimagrumab plus semaglutide 2.4 mg produced 22.1% weight loss at 72 weeks with 92.2% of that loss from fat mass.
| Feature | Trevogrumab plus optional garetosmab (Regeneron) | Bimagrumab (Lilly, ex-Versanis) |
|---|---|---|
| Target | GDF8 (trevogrumab) and activin A (garetosmab) as separate ligands | Activin receptor type II, blocks all upstream ligands |
| Trial | COURAGE Phase 2, 26-week interim data | BELIEVE Phase 2, 72-week published data |
| Weight loss with semaglutide 2.4 mg | ~10.1% at 26 weeks (semaglutide-alone arm) | 22.1% at 72 weeks (combination arm) |
| Fat mass change (peak arm) | −27.1% (triplet) | ~92.2% of total loss from fat mass |
| Lean mass change (peak arm) | −2.0% (triplet) | Roughly 2.5% gain as monotherapy at 30 mg/kg |
| Safety concern | 2 deaths in triplet arm; higher tolerability dropout | Diarrhea, muscle spasms, pancreatic enzyme rises |
| Development stage | Phase 2 interim, Phase 3 planning | Phase 2 complete, Phase 3 planning |
Both approaches say the muscle-loss half of GLP-1 body composition is not fixed. They arrive at that answer through different receptor-level logic. Bimagrumab blocks the receiver of the muscle-restriction signal. Trevogrumab and garetosmab block the specific ligands that transmit it. If both work at Phase 3 scale, the reason is that ActRII really is the choke point GLP-1 therapy exposes.
For a full walk through the BELIEVE dataset itself, see the Bimagrumab BELIEVE guide. For the broader picture of how much lean mass GLP-1 drugs actually take, the GLP-1 muscle loss research review walks through STEP, SURMOUNT, and today's preservation strategies.
Where the triplet ran into trouble
The activin A arm is where COURAGE's story turns careful. Regeneron disclosed two deaths in the triplet arm during the 26-week weight-loss phase, alongside a substantially higher rate of tolerability-related discontinuations than in any other arm. The company has not published detailed causes of death or full adverse-event tables. It continues to advance the double-antibody design and appears more cautious about the triplet than the initial press coverage implied.
Activin A signals well beyond muscle. It is expressed in reproductive tissue, vasculature, and immune cells, so broad blockade can produce effects that fall outside the muscle axis in ways a strict myostatin antibody does not. That is why the Phase 1 in postmenopausal females was the entry point rather than a general obesity cohort. Regeneron's data-monitoring committee has more relevant information now than the public releases show, and that information is what will decide whether garetosmab stays in the Phase 3 plan.
The comparison with bimagrumab matters here too. Bimagrumab has its own tolerability profile, but no Phase 2 deaths of the same signal. If the triplet's mortality signal turns out to be real and drug-related, the field likely converges on trevogrumab alone or on ActRII-level blockade rather than dual-ligand blockade.
What still has to happen before this reaches patients
COURAGE has three things left to report:
- The weight-maintenance phase, another 26 weeks after weight loss ends, expected to read out in late 2026. The relevant question is whether the antibody effect on lean mass persists once semaglutide is titrated down or held steady.
- A full safety analysis, including cause-of-death adjudication in the triplet arm and any downstream effects on bone, immune function, and glucose control.
- A peer-reviewed publication. Conference interim data is real, but the field will not treat any COURAGE finding as settled until it lands in Nature Medicine or NEJM with a full methods section and open access to the DXA data.
Even if all three land favorably, Phase 3 registration is a separate multi-year process. Regeneron would need at least one large trial with a hard clinical endpoint, physical function or fall risk in older adults, not just DXA-measured composition. That Phase 3 is not enrolled yet.
The practical timeline: no FDA-approved myostatin or activin A blocker is likely to reach obesity clinics before 2028 at the earliest. Bimagrumab is on a similar arc.
What GLP-1 users can actually do right now
Anyone starting or continuing semaglutide, tirzepatide, or retatrutide today has to work with the tools that already exist. The evidence for those tools is smaller than the antibody trials but consistent across the Phase 3 substudies:
- Resistance training three to four times a week during active weight loss is the most consistent finding across GLP-1 body-composition substudies for preserving lean mass.
- Protein intake in the 1.2 to 1.6 g/kg range (of goal body weight, not baseline) tracks with better lean mass retention in the same substudies.
- Slower titration and lower final doses appear to reduce absolute lean mass loss at the cost of less absolute weight loss, based on cross-trial comparisons across STEP and SURMOUNT (Wilding et al., NEJM 2021, PMID 33567185; Jastreboff et al., NEJM 2022, PMID 35658024).
If cost is the main gate keeping someone from titrating carefully, the cheapest GLP-1 access page covers compounded routes and telehealth pathways that support a slower ramp than the standard 16-week label protocol. That matters for muscle preservation more than most protocols acknowledge, because rapid early titration also produces the fastest early lean mass drop.
For research-grade injectable semaglutide and tirzepatide access, Ascension Peptides sells verified GLP-1 stacks with code ENHANCED for 50% off, and their COA library is worth checking whether or not you use them (it is the single strongest signal a research vendor can send). For oral peptides like BPC-157 that some users pair with resistance training during GLP-1 cycles for connective-tissue support, Limitless Biotech sells research-grade oral blends with code ENHANCED. Oral BPC-157 is a separate mechanism from muscle antibodies and has weaker direct evidence for muscle preservation, so treat it as adjunctive rather than a substitute for the antibody data.
For a fuller picture of maintenance strategies once weight loss stalls, see the ATTAIN-MAINTAIN oral orforglipron analysis.
The bigger picture
The obesity field spent the last three years treating the composition of GLP-1 weight loss as fixed. About 25 to 35% of every kilogram would come off as lean mass depending on the trial, and the mitigation was exercise plus protein plus hope the person keeps the weight off. COURAGE is the first Phase 2 to show a pharmacological way to break that ratio at a scale that matters. BELIEVE showed the same conclusion with a different receptor strategy.
Two Phase 2 trials do not make an approved treatment. Two Phase 2s that hit the same mechanism through different antibodies do change what the next Phase 3 wave of GLP-1 combinations will look like. The retatrutide era of "how much weight can we shed" was already narrowing the marginal returns on more potent GLP-1 agonists. The next front is which tissue that weight comes off.
Tip: If you are tracking body composition on a GLP-1 today, run a baseline DXA before starting and again at 16 to 20 weeks. That gives you the same reference points COURAGE used and lets you decide whether your muscle loss is trending closer to the semaglutide-alone number or something more preserved.
Research and educational purposes only. This article is not medical advice. Trevogrumab, garetosmab, and bimagrumab are investigational. The peptides discussed are unapproved for the muscle-preservation use covered here. Consult a licensed clinician before making decisions about weight-loss therapy, exercise, or supplementation. Nothing here establishes clinical efficacy or safety in humans beyond what the cited studies specifically report.