At a glance
- BELIEVE Phase 2 (PMID 41772149): high-dose bimagrumab + semaglutide 2.4 mg produced 22.1% weight loss at 72 weeks, with 92.2% of that loss coming from fat mass.
- Bimagrumab monotherapy at 30 mg/kg increased total body lean mass by 2.5% above baseline, the opposite direction from every approved GLP-1.
- Visceral adipose tissue fell 58.2% with combination therapy vs 35.8% with semaglutide 2.4 mg alone over 72 weeks.
- Heymsfield 2021 (PMID 33439265) earlier showed roughly 20.5% fat mass loss and 3.6% lean mass gain at 48 weeks in adults with T2D and obesity.
- Bimagrumab is Phase 2 only. No Phase 3 readout, no FDA approval, and no access outside Lilly-sponsored trials as of mid-2026.
The 22.1% number that changed the GLP-1 muscle question
Up to 40% of weight lost on GLP-1 receptor agonists comes from lean mass. That has been the asterisk on every Wegovy and Mounjaro success story since STEP and SURPASS landed. The standard mitigation, resistance training plus high protein intake, is the right answer and an incomplete one. Drug developers took the question more literally, and the most aggressive bet on the table came from Eli Lilly's $1.9 billion acquisition of Versanis Bio in 2023 to take ownership of bimagrumab, a fully human monoclonal antibody that blocks the activin type II receptor. In March 2026, the BELIEVE Phase 2 trial published in Nature Medicine gave the first head-to-head answer to whether the activin receptor bet works on top of semaglutide (Heymsfield et al. 2026, PMID 41772149). It did.
This article walks through what BELIEVE actually measured, what the four prior bimagrumab trials taught us, why the activin receptor pathway is mechanistically different from a pure myostatin block, what the safety profile looks like at clinical doses, and what sits between today's data and a marketed product.
Bottom line: In BELIEVE, 30 mg/kg bimagrumab IV every 12 weeks plus 2.4 mg semaglutide weekly produced 22.1% weight loss at 72 weeks with 92.2% of that loss from fat mass and lean mass preserved or increased. The same combination cut visceral adipose tissue by 58.2%. Bimagrumab is Phase 2 only. No Phase 3 readout, no approval, no access outside trials.
What bimagrumab actually is
Bimagrumab is a human monoclonal antibody that binds the activin type II receptors ActRIIA and ActRIIB with high affinity. ActRII receptors sit on the surface of skeletal muscle cells and respond to a family of negative growth regulators that includes myostatin, activin A, activin B, GDF11, and others. When myostatin or activin binds ActRII, it pairs with an ALK4 or ALK5 type I receptor, activates Smad2/3 signalling, and tells the muscle cell to stop growing or to break down protein. Block the receptor and that brake comes off.
The drug differs from earlier myostatin-pathway compounds in two ways. First, it blocks the receptor rather than the ligand. Follistatin and ACE-031 (ramatercept) work upstream by sequestering myostatin or by acting as decoy receptors. Bimagrumab binds the receptor directly, which means it neutralizes the entire panel of ActRII ligands at once. Second, bimagrumab is a long-acting human IgG1 antibody given intravenously every 4 to 12 weeks at clinical doses, which produces sustained receptor occupancy without daily peptide dosing.
For context on the pure myostatin-blocking compounds the research community uses, see our ACE-031 (ramatercept) myostatin inhibitor evidence review and Follistatin 344 myostatin pathway research. Bimagrumab covers a broader pharmacological surface than either.
A 2024 mechanistic review in the Journal of Basic and Clinical Physiology and Pharmacology (PMID 39385353) summarized the preclinical rationale: ActRII blockade increases muscle protein synthesis and decreases protein degradation, and animal data show a secondary effect on brown adipose tissue differentiation that may contribute to the fat loss signal observed in trials. Whether that brown fat effect translates to humans at clinical doses is unsettled.
BELIEVE: the trial Lilly bought Versanis to run
The BELIEVE study (NCT05616013) was the registrational-grade Phase 2 trial Versanis designed before the Lilly acquisition and that Lilly carried through to readout. It randomized 507 adults with obesity but without type 2 diabetes across 26 sites in the United States, Australia, and New Zealand into nine arms: placebo, bimagrumab monotherapy at 10 or 30 mg/kg IV every 12 weeks, semaglutide monotherapy at 1.0 or 2.4 mg subcutaneously weekly, and four combination arms crossing the two bimagrumab doses with the two semaglutide doses. The primary endpoint was percent change in body weight at 48 weeks, with body composition measured by DEXA. An open-label extension carried the highest-dose arms to 72 weeks (Heymsfield et al. 2026, PMID 41772149).
Headline results at 72 weeks
| Arm | Weight loss | % from fat mass | Visceral adipose tissue change |
|---|---|---|---|
| Placebo | ~0% | reference | reference |
| Bimagrumab 30 mg/kg alone | 10.8% | ~93% | -45.1% |
| Semaglutide 1.0 mg alone | ~11% | ~75% | not separately reported |
| Semaglutide 2.4 mg alone | 15.7% | 76% | -35.8% |
| Bimagrumab 30 + semaglutide 2.4 | 22.1% | 92.2% | -58.2% |
Three things in that table matter more than the headline weight loss number.
The combination produced 22.1% total weight loss, which is in the same neighborhood as tirzepatide at 15 mg in SURMOUNT-1 and well above the 14.9% semaglutide produced in STEP 1. That alone makes the combination an interesting competitive position for Lilly given they already sell tirzepatide.
The composition of the weight loss is the more important finding. In the high-dose combination arm, 92.2% of the lost weight came from fat mass. In the semaglutide-only arm, that number was 76%. Translated bluntly: a 100 kg patient on semaglutide 2.4 mg loses roughly 16 kg over 72 weeks with about 4 kg of that from lean tissue. The same patient on the bimagrumab combination loses roughly 22 kg with about 1.7 kg from lean tissue. The bimagrumab arm patient ends 72 weeks with more lean mass for the same level of physical activity.
The visceral adipose tissue (VAT) number is the most metabolically meaningful. VAT predicts cardiometabolic risk independently of total adiposity. The combination cut VAT by 58.2% versus 35.8% on semaglutide 2.4 mg alone, a 22 percentage-point difference that translates directly to insulin resistance and cardiovascular risk markers.
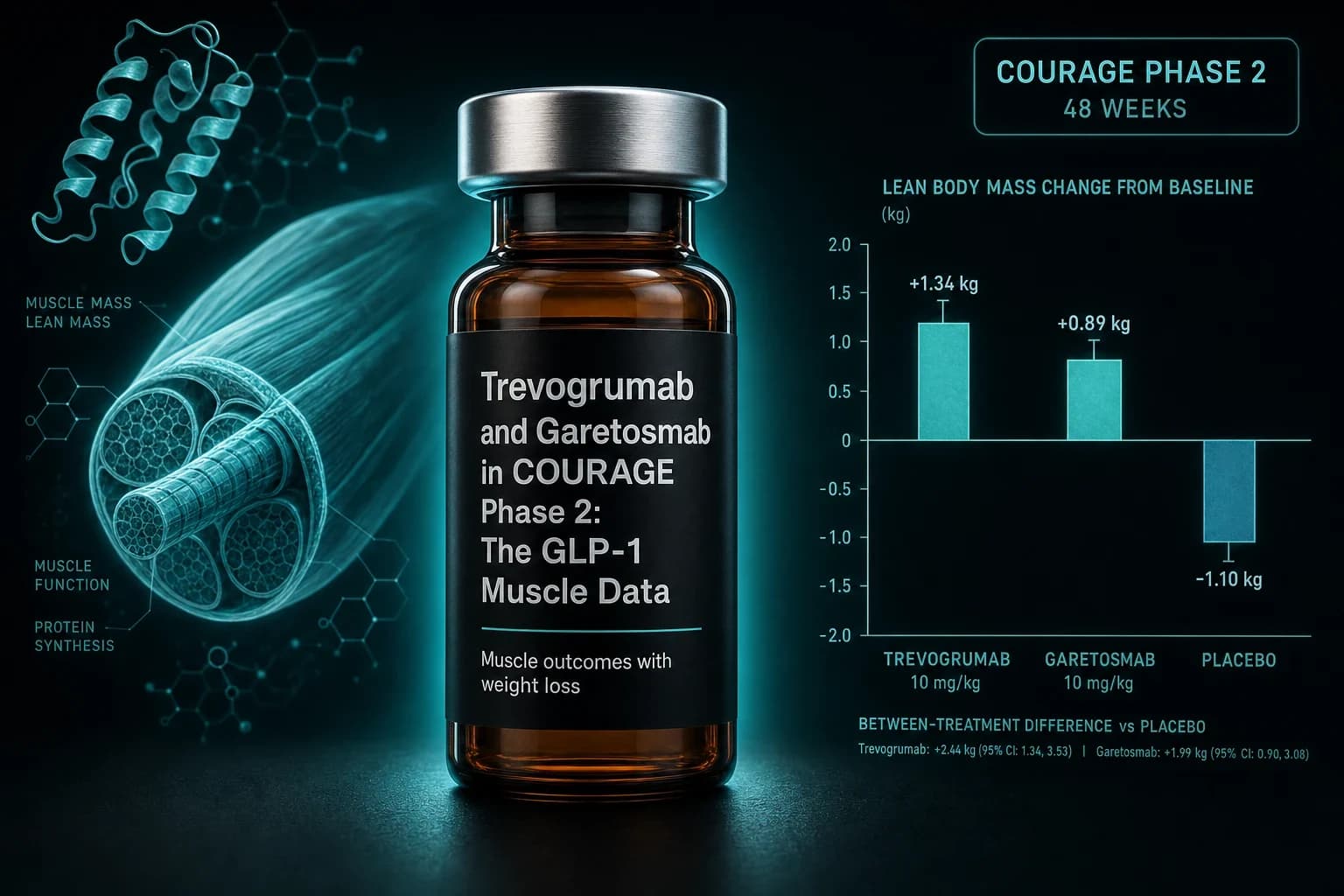
Lean mass: the cleanest signal
Bimagrumab 30 mg/kg monotherapy actually increased total body lean mass by 2.5% above baseline at 72 weeks. Every approved GLP-1 monotherapy moves lean mass in the opposite direction. That divergence is what the activin receptor mechanism predicts, and BELIEVE is the first long-duration human dataset that confirms the prediction holds when combined with a high-efficacy GLP-1.
The combination arm did not produce the same lean mass increase as bimagrumab alone (the catabolic pressure of 22% weight loss eventually shows up somewhere) but the net effect was preserved lean mass at a 22.1% total weight loss endpoint that no GLP-1 monotherapy has matched without measurable lean tissue penalty. The GLP-1 muscle loss research review covers the baseline class numbers in more detail.
The pre-BELIEVE bimagrumab record
BELIEVE did not appear out of nothing. Four earlier bimagrumab trials had already characterized the body composition effect in different populations, and the consistency of the signal across populations is what made the BELIEVE bet plausible to Versanis and to Lilly.
| Study | Population | n | Duration | Bimagrumab effect | PMID | | --- | --- | --- | --- | --- | | Heymsfield 2021 | T2D + obesity | 75 | 48 wk | Body fat -20.5%, lean mass +3.6%, HbA1c -0.76% | 33439265 | | Garito 2018 | Insulin-resistant adults | 16 | 10 wk | Lean mass +2.7%, fat mass -7.9%, insulin sensitivity +20-40% | 28643356 | | Rooks 2020 | Sarcopenia, age 70+ | 180 | 24 wk | Skeletal muscle mass +5.7% vs placebo, gait speed unchanged | 33074327 | | Polkey 2019 | COPD with muscle depletion | 67 | 24 wk | Lean mass +6.0% vs placebo, no functional improvement | 30095981 | | Rooks 2017 | Sarcopenia POC | 40 | 24 wk | Lean mass +7.6% vs placebo, walking distance improved | 28653345 |
The Heymsfield 2021 JAMA Network Open Phase 2 trial is the closest analog to BELIEVE's monotherapy arms. Adults with type 2 diabetes and BMI 28 to 40 received IV bimagrumab or placebo every 4 weeks for 48 weeks. The bimagrumab arm lost 20.5% of total body fat mass versus 0.5% on placebo and gained 3.6% in lean mass versus a 0.8% loss on placebo. HbA1c fell 0.76 percentage points compared with a 0.04 point increase on placebo. The implication that struck the field at the time, and that drove the Versanis acquisition, was that a body composition drug could move HbA1c by a clinically meaningful amount without acting on incretin biology at all.
Garito 2018 in Diabetes, Obesity and Metabolism (PMID 28643356) tested a single dose in 16 insulin-resistant adults and showed lean mass increased 2.7% and fat mass decreased 7.9% at week 10. The insulin sensitivity measurement, done by hyperinsulinaemic-euglycaemic clamp, improved 20% to 40% depending on the metric used. The trial was small but mechanistically important because it confirmed the body composition shift translates to a real change in glucose handling.
The Rooks 2020 sarcopenia trial (PMID 33074327) and the Polkey 2019 COPD trial (PMID 30095981) are the most instructive negative signals. Both produced clean lean mass gains, but neither translated those gains into measurable functional improvements at the prespecified endpoints. Bigger muscle does not automatically mean better function over 24 weeks in older or chronically ill populations. That gap is part of why the obesity application, which cares about composition more than peak function, became the lead indication.
Why the activin receptor approach is not just another myostatin block
Pure myostatin neutralization has a long clinical history. Stamulumab, domagrozumab, landogrozumab, and others were tested in muscular dystrophies and sarcopenia. None produced regulatory-grade functional results. The reason is that myostatin is one of several negative regulators of muscle. Block it alone and the other ligands (activin A, activin B, GDF11) can partially compensate.
Bimagrumab works one step downstream, at the shared receptor. A 2024 systematic review and meta-analysis in Aging Clinical and Experimental Research summarized the body composition effect of bimagrumab across the available trials and concluded the lean mass and fat mass changes are more consistent and larger in magnitude than any pure-ligand myostatin blocker has shown in humans. A 2025 review in Reviews in Endocrine and Metabolic Disorders (PMID 40320499) specifically positioned bimagrumab as the most promising of the muscle-preserving adjuncts to incretin therapy.
The trade-off is target breadth. Blocking the entire ActRII signal also affects activin and GDF11 functions outside skeletal muscle, including signalling in the pituitary, gonads, and bone. The clinical data so far show the on-target side effects are tolerable at the doses tested, but the long-term endocrine signal is one of the open questions Phase 3 will need to answer.
Safety and tolerability
The bimagrumab side-effect profile in BELIEVE and the prior trials is distinct from the GLP-1 class profile. Where semaglutide drives nausea, vomiting, diarrhea, and fatigue through central appetite suppression and delayed gastric emptying, bimagrumab produces a different pattern.
The most consistent bimagrumab-related events across trials are muscle cramps and acne. Both are dose-related and most pronounced at the 30 mg/kg dose used in BELIEVE. Mild and transient laboratory elevations in pancreatic enzymes (lipase and amylase) appear in roughly a third of bimagrumab-treated patients, typically without clinical pancreatitis. Mild elevations in liver enzymes also appear in a fraction of patients. The pattern is consistent with the activin receptor's role in non-muscle tissues and has not produced a serious safety signal in trials to date.
In the combination arms of BELIEVE, discontinuation rates due to adverse events were higher than semaglutide monotherapy. The GI events of the GLP-1 class did not disappear, and they stacked with the cramps and acne signal of bimagrumab. There were no deaths in the trial. The 2025 review in Cardiology in Review (PMID 41248895) covers the cross-trial bimagrumab safety summary across inclusion body myositis, sarcopenia, and obesity programs.
Note: The bimagrumab safety profile in published trials runs to 48 to 72 weeks. Long-term endocrine signals, including pituitary, gonadal, and bone effects predicted by activin biology, will require Phase 3 sample sizes and longer follow-up to characterize properly.
What BELIEVE does not mean
Three things are easy to over-read from a Nature Medicine Phase 2 paper.
First, BELIEVE is not approval. The FDA does not approve drugs on the basis of Phase 2 body composition endpoints. The registrational program for bimagrumab plus semaglutide (or another GLP-1) will require Phase 3 trials with weight loss, cardiovascular outcomes, and likely a body composition co-primary endpoint. Lilly has not publicly committed to a Phase 3 start date or a specific GLP-1 partner. A realistic registrational timeline for the combination is not earlier than 2028 to 2029.
Second, BELIEVE does not say bimagrumab is the only or best answer. The other muscle-preservation adjuncts under active investigation include amylin co-agonists, glucagon co-agonists, and selective androgen receptor modulators. The GLP-1 amylin combinations 2026 review covers the amylin angle, where compounds like cagrilintide and petrelintide produce a different lean-mass profile by reducing total catabolic pressure rather than by anabolic signalling.
Third, BELIEVE does not change what current GLP-1 users can do today. Bimagrumab is not available from any vendor, compounder, or research-peptide source. It is a sponsor-exclusive monoclonal antibody under Lilly clinical development. Anything sold under the bimagrumab name today is not the disclosed molecule.
What current GLP-1 users can actually do about muscle loss
The honest 2026 answer for someone losing muscle on a current-generation GLP-1 has not changed because of BELIEVE. The biggest practical input is still resistance training paired with adequate protein, ideally 1.6 to 2.2 g/kg of target body weight per day. Multiple incretin-class trials show resistance-trained arms preserve lean mass better than sedentary arms even on the highest GLP-1 doses.
The research-peptide options for muscle preservation are pure myostatin-pathway compounds with their own evidence trade-offs. The ACE-031 evidence review covers the activin receptor decoy approach, which is mechanistically related to bimagrumab but blocks at the ligand level. The Follistatin 344 evidence review covers the upstream pathway block. Both are research compounds with limited human data and meaningful uncertainty about long-term safety profiles. They are not bimagrumab, and they should not be treated as equivalent.
For weight regain after discontinuation, which is the related problem, the stopping GLP-1 weight regain research review covers what the withdrawal trials actually show. The most consistent finding is that lean mass lost during the on-treatment phase is the hardest tissue to recover during the post-discontinuation phase, which is a separate argument for taking muscle preservation seriously during the loss phase.
Researchers working with weight-loss peptides today can source tirzepatide and semaglutide from Ascension Peptides with public per-batch COAs and 50% off using code ENHANCED. For ACE-031 and similar research-grade myostatin-pathway compounds, Ascension carries the catalog with the same code. Limitless Biotech carries the oral peptide format for compounds where oral data exist, also with code ENHANCED.
FAQ
Is bimagrumab available anywhere?
No. Bimagrumab is an investigational human monoclonal antibody under Eli Lilly clinical development. It is sponsor-exclusive and not available from any pharmacy, compounder, or research-peptide vendor. The molecule's manufacturing process is also outside the technical scope of standard research-peptide synthesis.
How does bimagrumab compare to retatrutide for muscle preservation?
Retatrutide is a triple agonist of GLP-1, GIP, and glucagon receptors. The TRIUMPH-1 Phase 3 readout showed 30.3% weight loss but did not separately report a body composition split competitive with the BELIEVE numbers. The two approaches are not interchangeable: retatrutide drives total weight loss through multi-incretin signalling, while bimagrumab specifically protects lean mass by blocking activin receptor signalling.
Does ACE-031 or follistatin do the same thing as bimagrumab?
Mechanistically related but not equivalent. ACE-031 is a soluble activin receptor decoy that sequesters myostatin and activin upstream. Follistatin binds myostatin directly. Bimagrumab blocks the receptor itself, which neutralizes all ActRII ligands at once. None of the three has the BELIEVE-level published human trial data behind it. ACE-031 development was halted in 2010 over an unrelated vascular signal.
When will bimagrumab plus semaglutide be approved?
Not before 2028 to 2029 on the most optimistic timeline. Lilly has not publicly committed to a Phase 3 start date or a specific GLP-1 partner as of mid-2026. The Phase 3 program will need a hard clinical endpoint, likely weight loss or cardiovascular outcomes, with body composition as a co-primary or secondary. A realistic FDA decision is in the late 2020s at the earliest.
Why did Lilly buy Versanis instead of running this themselves?
Versanis owned the bimagrumab development rights from Novartis, who had taken it through the muscle disease and obesity Phase 2 trials. Lilly's $1.9 billion acquisition in 2023 gave them ownership of the BELIEVE trial in flight, with the readout protected from competing development. The strategic logic is that combining bimagrumab with Lilly's own tirzepatide or a next-generation incretin could produce a body composition profile no competitor can match.
This article is for educational and research purposes only. It summarizes Phase 2 randomized clinical trial data for an investigational human monoclonal antibody. Bimagrumab is not FDA-approved, not EMA-approved, and not available outside Lilly-sponsored clinical trials as of June 2026. The BELIEVE trial described here measured body composition and weight loss endpoints under controlled 72-week conditions and does not establish efficacy or safety for any individual outside of that trial. Long-term endocrine, bone, and reproductive signals predicted by activin receptor biology have not been characterized at clinical Phase 3 sample sizes. Nothing in this article is medical advice or a recommendation to use any compound. Discuss any peptide or biologic use with a qualified clinician.