At a glance
- SLIM LIVER (A5371) cut liver fat 31.3% in 24 weeks of semaglutide 1 mg in PWH with MASLD (Lake 2024, PMID 38684100).
- The Eckard phase 2b RCT dropped visceral fat 30.6% at 32 weeks in HIV lipohypertrophy (Eckard 2024, PMID 38964354).
- Semaglutide reduced hsCRP roughly 48%, IL-6, and sCD163 in the Funderburg inflammation substudy (2025, PMID 40160348).
- CROI 2026 CNICS tirzepatide poster: weight -5.9% and HbA1c -0.58% at 1 year across 743 PWH.
- Atazanavir and rilpivirine warrant ART level monitoring during GLP-1 titration because of delayed gastric emptying.
Modern combination antiretroviral therapy turned HIV into a chronic disease that people live with for decades. Then it created a new problem: 40 to 50 percent of adults on suppressive ART now meet criteria for obesity, central adiposity, or metabolic-associated steatotic liver disease (MASLD), a rate substantially higher than age-matched HIV-negative peers. Every pivotal GLP-1 trial that produced the Wegovy, Zepbound, and Mounjaro approvals excluded people with HIV. For the population arguably most at risk of GLP-1-treatable comorbidities, the evidence base had to be built separately.
That evidence is now landing. The SLIM LIVER trial (A5371), the Eckard and McComsey lipohypertrophy phase 2b RCT, an inflammation substudy, an epigenetic aging pilot, and two real-world cohorts presented at CROI 2026 all point in the same direction. Semaglutide and tirzepatide work in people with HIV, and they may do more than shed weight. This article walks through what has been published, what CROI 2026 added, where the tesamorelin story still fits, and what the drug interaction realities look like when a GLP-1 lands on top of modern ART.
Why HIV needs its own GLP-1 evidence base
Two things make GLP-1 data in people living with HIV (PWH) not automatically portable from the general trials.
First, the phenotype is different. Modern integrase inhibitor-based regimens, particularly dolutegravir and bictegravir combined with tenofovir alafenamide, drive weight gain that concentrates centrally. The result often looks less like classical HIV-associated lipodystrophy of the 2000s (peripheral fat wasting plus dorsocervical fat pads) and more like a metabolically active central adiposity that overlaps with, but is not identical to, general-population obesity. That is the population the modern GLP-1 studies actually enrolled.
Second, the comorbidity profile is different. Baseline inflammation is elevated on suppressive ART. MASLD prevalence in PWH runs roughly 30 to 40 percent, higher than the general-population 25 percent baseline. Cardiovascular risk sits about 1.5 to 2 times higher after adjustment for traditional risk factors. Insulin resistance is more common. A drug that only moves the scale would not be as interesting as a drug that also moves the underlying inflammatory and metabolic milieu.
The 2024 and 2025 RCTs test exactly that broader question.
SLIM LIVER (A5371): the liver fat readout
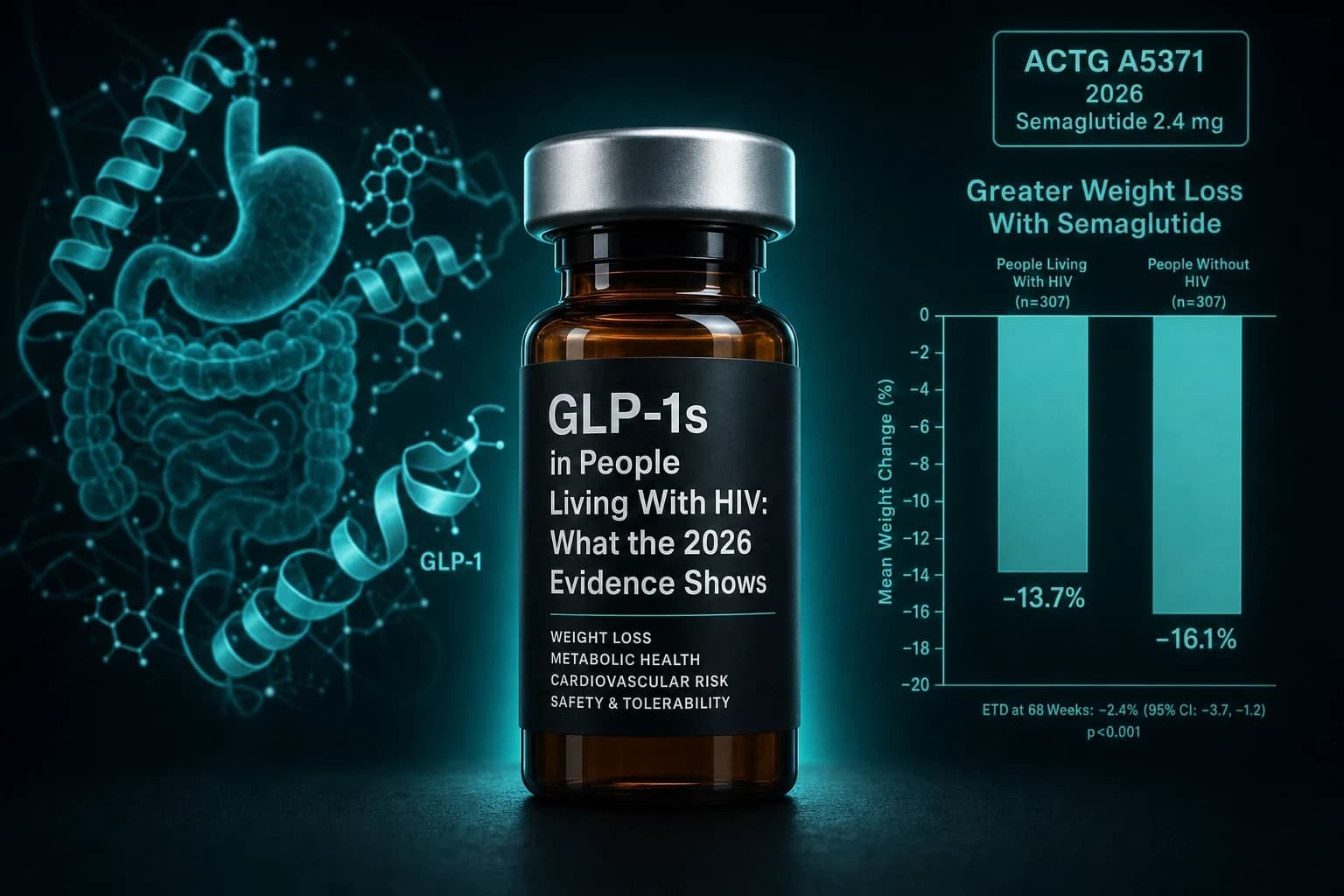
Lake et al., Ann Intern Med 2024 (PMID 38684100) reported the first prospective GLP-1 trial for MASLD in people with HIV. A5371, the SLIM LIVER study, was a single-arm open-label pilot funded by the NIH ACTG network. Fifty-one adults on suppressive ART with intrahepatic triglyceride content of 5 percent or higher on MRI-PDFF received subcutaneous semaglutide titrated to 1 mg weekly for 24 weeks.
Primary endpoint: change in MRI-quantified intrahepatic triglycerides at week 24. The trial hit hard.
- Intrahepatic triglycerides fell by 31.3 percent (absolute -4.6 percentage points on the MRI-PDFF scale)
- 29 percent of participants had complete MASLD resolution (defined as post-treatment liver fat under 5 percent)
- 58 percent had a relative reduction of 30 percent or greater in liver fat
- Weight loss ran roughly 8 percent
- Hemoglobin A1c, insulin resistance, and triglycerides all fell
For a single-arm 24-week pilot, that is a strong signal. For context, the ESSENCE phase 3 semaglutide trial in general-population MASH hit similar liver endpoints in a much larger, controlled setting. The SLIM LIVER magnitude was not smaller in the HIV cohort. If anything, the liver fat reduction sat on the high end of what semaglutide produces in metabolic MASLD.
Bottom line: In PWH with MASLD, 24 weeks of semaglutide 1 mg weekly cut liver fat by 31.3 percent and drove complete steatosis resolution in nearly 30 percent of participants. Effect size is comparable to what semaglutide produces in general-population MASH.
The follow-up work from SLIM LIVER also reported that semaglutide did not accelerate muscle mass loss in a way that was clinically concerning, an important safety signal in a population that is already at elevated sarcopenia risk from ART and chronic inflammation.
The lipohypertrophy phase 2b RCT
The largest single-site RCT of a GLP-1 in PWH was published as Eckard, McComsey, and colleagues, Lancet Diabetes Endocrinol 2024 (PMID 38964354). NCT04019197 enrolled 108 adults with HIV-associated lipohypertrophy and randomized them 1:1 to once-weekly subcutaneous semaglutide (8 weeks of titration to 1 mg, then 24 weeks at target) or matched placebo.
Primary endpoint at 32 weeks was change in abdominal visceral adipose tissue (VAT).
- VAT dropped 30.6 percent on semaglutide versus placebo
- Abdominal subcutaneous adipose tissue fell 11.2 percent
- Total body fat fell 18.9 percent
- Weight dropped roughly 6 to 8 kg on average
- Discontinuation for adverse events was rare; GI symptoms were the dominant AE and mirrored the general-population semaglutide profile
The VAT signal is the number that matters most in this population. Central adiposity is what drives the cardiometabolic risk in modern-era PWH. A 30.6 percent reduction at a dose (1 mg) that sits a step below the 2.4 mg weight-loss target is a large effect for a compartment that was historically hard to move without tesamorelin.
Inflammation and immune activation
The Eckard trial included a prespecified inflammation substudy, Funderburg, Eckard et al., Open Forum Infect Dis 2025 (PMID 40160348). At week 32, semaglutide-treated participants showed:
- High-sensitivity CRP: reduced roughly 48 percent from baseline
- Interleukin-6: reduced (p less than 0.02)
- Soluble CD163 (a marker of monocyte and macrophage activation): reduced (p less than 0.02)
- Soluble CD14: trend toward reduction (p equal to 0.08)
These are not weight-loss surrogates. Inflammation reductions of this magnitude on a GLP-1 in a general-population trial would be considered noteworthy. In PWH, where chronic low-grade inflammation on ART is one of the mechanisms proposed for accelerated cardiovascular and cognitive aging, they may be the more clinically important signal than the fat-loss numbers.
Epigenetic aging: the 2025 substudy
The most speculative but most striking readout so far comes from Semaglutide Slows Epigenetic Aging in People with HIV-associated lipohypertrophy (PMID 40791720), a 2025 analysis of DNA methylation clocks in the same NCT04019197 cohort. Eighty-four participants had baseline and 32-week epigenetic clock measurements. Compared to placebo, semaglutide moved multiple clocks in the same direction:
- PCGrimAge: -3.1 years
- GrimAge V1: -1.4 years
- GrimAge V2: -2.3 years
- PhenoAge: -4.9 years
- DunedinPACE: -0.09 units (roughly 9 percent slower pace of aging)
- OMICmAge multi-omic clock: -2.2 years
- RetroAge transposable-element clock: -2.2 years
These are surrogate biomarkers, not proof of longer life. Epigenetic clocks are still being validated as outcome measures, and 32 weeks is a short window. But the fact that a metabolic drug moved multiple independent aging clocks in the same direction in a placebo-controlled setting is the first mechanistic signal that GLP-1 receptor engagement in a chronically inflamed population may reach beyond weight, glycemia, and lipids.
Note: Epigenetic clock changes are hypothesis-generating, not clinically actionable. Do not extrapolate a specific decline in biological aging to any promise about lifespan or healthspan on a GLP-1.
Real-world weight loss in the CNICS cohort
Trials answer efficacy questions. Real-world data answers the follow-up question of how a drug behaves in clinic. The CNICS observational cohort, drawing from eight academic HIV centers in the US, is the largest published PWH GLP-1 real-world dataset.
The semaglutide analysis, PMID 37976053, followed 222 PWH who initiated semaglutide between 2018 and 2022 for at least 1.1 years on average.
- Weight change at 1 year: -6.47 kg (95% CI -7.67 to -5.18)
- HbA1c change at 1 year (in 157 participants with follow-up A1c): -1.07 percent (95% CI -1.64 to -0.50)
Both numbers track the general-population semaglutide observational literature over similar durations.
At CROI 2026, the CNICS group presented an expanded tirzepatide analysis in 743 PWH who initiated tirzepatide between June 2022 and February 2025. Mean age 53. 28 percent women. Mean BMI 35 kg per square meter, with 84 percent at BMI 30 or higher. 62 percent had type 2 diabetes. 95 percent were virally suppressed.
- Mean weight reduction at 1 year: 5.9 percent
- HbA1c change at 1 year: -0.58 percent
- Sex difference in glycemic response: men -0.66 percent, women -0.15 percent (p less than 0.01)
The tirzepatide weight loss in this cohort was smaller than SURMOUNT-1 (roughly 20 percent) and smaller than the general-population real-world studies on tirzepatide (roughly 10 to 13 percent at 1 year). Two candidate explanations. First, dose distribution: many patients did not titrate to top doses in the real-world setting. Second, the high proportion of patients with type 2 diabetes, where GLP-1 weight loss magnitudes are typically 30 to 40 percent lower than in nondiabetic obesity cohorts. The SURMOUNT-5 head-to-head between tirzepatide and semaglutide sets the general-population benchmark against which the PWH numbers should be read.
What the data looks like side by side
| Trial or cohort | Population | Compound and dose | Duration | Weight | Key non-weight endpoint |
|---|---|---|---|---|---|
| SLIM LIVER (PMID 38684100) | PWH with MASLD, N=51 | Semaglutide 1 mg wk, open-label | 24 wk | ~-8% | Liver fat -31.3%; MASLD resolution 29% |
| Eckard 2024 (PMID 38964354) | PWH with lipohypertrophy, N=108 | Semaglutide 1 mg wk vs placebo | 32 wk | ~-6 to -8 kg | VAT -30.6%; total body fat -18.9% |
| Funderburg substudy (PMID 40160348) | Same N=108 | Same | 32 wk | (same) | hsCRP ~-48%; IL-6, sCD163 reduced |
| Epigenetic aging substudy (PMID 40791720) | Same N=84 with clocks | Same | 32 wk | (same) | GrimAge V2 -2.3 y; DunedinPACE -0.09 |
| CNICS semaglutide (PMID 37976053) | PWH new users, N=222 | Semaglutide (mixed doses) | 1 y avg | -6.47 kg | HbA1c -1.07% |
| CNICS tirzepatide, CROI 2026 poster | PWH new users, N=743 | Tirzepatide (mixed doses) | 1 y | -5.9% | HbA1c -0.58% |
The picture is consistent across designs. Semaglutide moves weight, visceral fat, liver fat, glucose, systemic inflammation, and multiple aging clocks. Tirzepatide, based on the CROI 2026 real-world data, moves weight and A1c on a similar per-dose basis but has less deep mechanistic characterization in PWH specifically.
Drug-drug interaction realities
No pharmacokinetic study to date has shown a clinically meaningful interaction between GLP-1 receptor agonists and integrase inhibitors, NRTIs, or NNRTIs generally. That is not a green light for every combination. Two specific concerns are worth flagging.
First, delayed gastric emptying. Semaglutide, tirzepatide, and liraglutide all slow gastric transit. Two older ART agents rely on gastric acidity or intact absorption windows: atazanavir requires acidic pH for dissolution and is affected by anything that reduces stomach acid or delays emptying, and rilpivirine absorption is highly food-dependent. Anyone on either agent starting a GLP-1 should coordinate with their HIV clinician on whether therapeutic drug monitoring is warranted during titration.
Second, oral formulations. Oral semaglutide (Rybelsus) has a narrow absorption window and stringent dosing conditions (fasted, small water sip, wait 30 minutes). Adherence in a patient already juggling a single-tablet ART regimen can be a real barrier. For most PWH the injectable weekly formulation is operationally easier.
For the specific case of tirzepatide plus modern integrase-based ART, published pharmacokinetic modeling has consistently predicted no meaningful interaction, and the CNICS real-world dataset presented at CROI 2026 did not surface any safety signal. Even so, the sample of PWH on protease inhibitor backbones with pharmacokinetic monitoring during GLP-1 titration remains small, and post-marketing surveillance is still accumulating.
Where tesamorelin still fits
Tesamorelin has been the go-to injectable for HIV-associated visceral fat since 2010. It is FDA-approved specifically for reduction of excess abdominal fat in HIV-associated lipodystrophy, and the Falutz et al. NEJM 2007 pivotal trial (PMID 18057338) established a roughly 15 percent VAT reduction on a targeted mechanism (GHRH analog upregulating pulsatile growth hormone secretion).
Semaglutide in the Eckard trial produced VAT reductions of 30.6 percent, roughly double the tesamorelin effect. Semaglutide also drives systemic weight loss, HbA1c improvement, and the inflammation signals that tesamorelin does not touch.
The comparison is not "which one wins." It is "which one for what." A pragmatic framework:
- PWH with isolated VAT excess and normal weight: tesamorelin retains a rational niche. The tesamorelin visceral fat guide walks the trial record and dosing details.
- PWH with obesity, MASLD, or T2D: GLP-1 (semaglutide or tirzepatide) is now the more evidence-supported first move.
- PWH with elevated cardiovascular risk where inflammation is the primary concern: GLP-1 for the immune-activation signal; tesamorelin no longer the obvious choice.
The two agents are also potentially combinable in principle, though no RCT has tested that combination and the practical cost of stacking two specialty injectables limits real-world use.
Cost, access, and the pragmatic path
GLP-1 access for PWH runs on the same rails as GLP-1 access for anyone else. Insurance coverage of Wegovy and Zepbound for obesity is uneven; coverage of Ozempic and Mounjaro for type 2 diabetes is generally better. Ryan White programs and 340B pricing can, in some states, materially reduce out-of-pocket cost for PWH specifically. The cheapest GLP-1 access routes article covers the compounded telehealth, brand-name, and research-grade paths without HIV-specific framing.
For prescription telehealth GLP-1 through a licensed clinician, the Yucca Health review walks through pricing, monitoring, and how the intake handles baseline HbA1c, weight, and comorbidity screening. Yucca handles compounded semaglutide and tirzepatide with prescriber oversight, which is the operationally simplest path for a PWH who wants a monitored program without a specialty referral.
Research-use vial sourcing for PWH is not different from research-use sourcing for anyone else in either the practical mechanics or the compliance rules. Ascension Peptides is the reference vendor for injectable research-grade material, with 50% off using code ENHANCED. The reconstitution calculator handles the BAC water arithmetic; the lab tests library is the COA reference for anyone verifying vial identity and purity independently.
Whichever route, the HIV-specific considerations are consistent:
- Coordinate with the HIV clinician on whether ART blood levels need monitoring during GLP-1 titration
- Screen for concurrent MASLD and consider baseline MRI-PDFF or a validated non-invasive score
- Track weight loss quality (lean vs fat mass) more attentively than in general-population obesity, given elevated baseline sarcopenia risk on chronic ART
- Do not swap tesamorelin off a stable regimen without a specific reason
For readers who want the underlying pharmacology context for semaglutide dosing choices, the microdosing GLP-1s evidence review covers why the sub-labeled doses used in some PWH trials still produce meaningful effect on the surrogate endpoints even if they are not the top weight-loss doses tested in the pivotal general-population trials.
Bottom line
GLP-1s work in people living with HIV. The signal replicates across a single-arm liver trial (SLIM LIVER), a randomized visceral fat trial (Eckard 2024), an inflammation substudy, an epigenetic aging pilot, and two real-world cohorts spanning both semaglutide and tirzepatide. Effect sizes on weight, HbA1c, and cardiometabolic surrogates track the general-population data. The inflammation and epigenetic aging findings are the interesting new territory, hinting at benefits that go beyond what a scale or A1c meter reads.
For a PWH with MASLD, obesity, or T2D, the 2026 evidence supports GLP-1 initiation in the same way it does for HIV-negative adults, with three caveats: coordinate ART levels for atazanavir or rilpivirine, screen for lean mass loss, and understand that tesamorelin still occupies a specific niche for isolated visceral adiposity in normal-weight patients. The population that got locked out of every pivotal GLP-1 trial in the last decade is now the one where the mechanism arguably matters most.
Disclaimer
This article is for educational and research purposes only and is not medical advice. Semaglutide and tirzepatide are FDA-approved for type 2 diabetes and chronic weight management in HIV-negative populations; use in people living with HIV falls under general labeling and is not a distinct HIV-specific indication as of July 2026. The SLIM LIVER trial (A5371) was open-label and single-arm; the Eckard and McComsey lipohypertrophy trial is single-center. Epigenetic aging clocks are surrogate biomarkers, not proof of altered lifespan or healthspan. Drug-drug interaction data for GLP-1s with atazanavir and rilpivirine remain limited and are extrapolated from mechanistic considerations rather than dedicated PK studies. Any change to antiretroviral therapy, initiation of a GLP-1, or switching between tesamorelin and a GLP-1 should be made with a qualified HIV clinician familiar with the patient's regimen and comorbidities.