At a glance
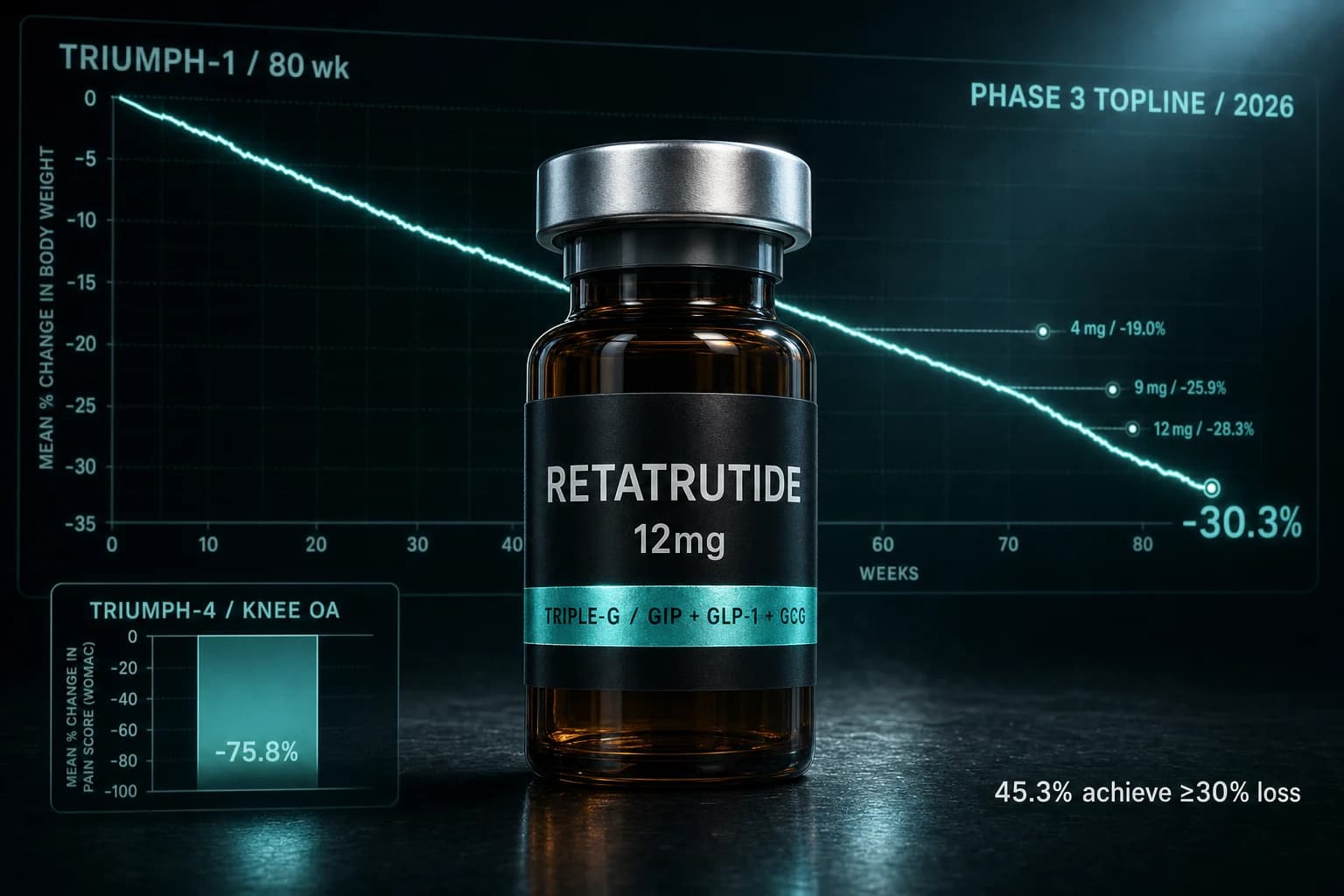
- TRIUMPH-1 (n=2,339): retatrutide 12 mg cut body weight 28.3% at 80 weeks vs 2.2% placebo.
- Extension cohort (BMI ≥35) reached 30.3% / 85.0 lbs at 104 weeks on 12 mg.
- 45.3% of 12 mg participants hit ≥30% weight loss, a threshold previously owned by bariatric surgery.
- TRIUMPH-4 in knee osteoarthritis: 28.7% weight loss plus 75.8% relative WOMAC pain reduction.
- New Phase 3 safety signal: dysesthesia in 20.9% of 12 mg patients vs 0.7% on placebo.
Retatrutide just printed the biggest obesity readout in pharma history. 30.3% body weight reduction at 104 weeks. 85.0 lbs lost on average. 45.3% of the 12 mg arm cleared the bariatric-surgery threshold.
The TRIUMPH-1 topline drop did not just clear the bar set by tirzepatide and semaglutide. It moved the goalposts to a place a once-weekly injectable has never been.
Here is what the data actually shows, what the trial design means in practice, and the one new safety signal worth taking seriously before anyone calls this a clean sweep.
What TRIUMPH-1 actually showed at 80 weeks
TRIUMPH-1 was a randomized, double-blind, placebo-controlled Phase 3 trial in 2,339 adults with obesity or overweight plus at least one weight-related comorbidity. Participants without type 2 diabetes were assigned to retatrutide 4 mg, 9 mg, 12 mg, or placebo, once weekly, for 80 weeks.
The primary endpoint was mean percent change in body weight from baseline. The headline numbers:
| Arm | Weight loss at 80 wk | Avg lbs lost |
|---|---|---|
| Retatrutide 4 mg | -19.0% | ~47 lbs |
| Retatrutide 9 mg | -25.9% | ~64 lbs |
| Retatrutide 12 mg | -28.3% | 70.3 lbs |
| Placebo | -2.2% | ~5 lbs |
At 12 mg, 45.3% of participants achieved at least 30% body weight loss. That number matters. The 30% threshold has been the line where pharmacotherapy historically lost to surgery. TRIUMPH-1 is the first Phase 3 readout where almost half the treatment arm crossed it.
Compare that to the SURMOUNT-5 head-to-head between tirzepatide and semaglutide, where tirzepatide hit 20.9% at 72 weeks. Retatrutide's 28.3% sits roughly 7 percentage points above the best previously-shown Phase 3 number for a single agent. The full SURMOUNT-5 evidence breakdown is in our tirzepatide vs semaglutide SURMOUNT-5 article.
Bottom line: Every dose hit its endpoint with statistical significance. The 12 mg arm reset what "best in class" means for a once-weekly injectable.
The 104-week extension and the 30.3% number
The figure most coverage is leading with, 30.3%, is not the primary endpoint. It comes from a prespecified blinded extension that enrolled 532 participants with baseline BMI of 35 or higher who completed the 80-week main study and tolerated their assigned dose.
In that BMI-35-plus cohort, participants who stayed on retatrutide 12 mg through 104 weeks lost an average of 85.0 lbs, or 30.3% of starting body weight.
Two things to understand about that number:
- It is in a selected subset. People who tolerated the drug and had higher baseline BMI tend to lose more. The 28.3% at 80 weeks across the full 12 mg arm is the more generalizable figure.
- The weight loss curve was still declining at 80 weeks. The extension data confirms what the slope already suggested: retatrutide does not plateau the way Phase 2 trials of tirzepatide and semaglutide did at similar timepoints.
The Phase 2 retatrutide trial published by Jastreboff et al. (2023) in NEJM showed 24.2% weight loss at 48 weeks at the 12 mg dose. The Phase 3 80-week number of 28.3% follows the slope you would have extrapolated from the Phase 2 curve almost exactly. That kind of dose-response coherence between Phase 2 and Phase 3 is rare and predictive.
TRIUMPH-4: the osteoarthritis readout that surprised rheumatologists
Five months before TRIUMPH-1 dropped, Lilly reported TRIUMPH-4, a Phase 3 trial in 445 adults with obesity plus symptomatic knee osteoarthritis. 68 weeks. 1:1:1 randomization to retatrutide 9 mg, 12 mg, or placebo. No participants with type 2 diabetes.
The weight-loss numbers in TRIUMPH-4 tracked TRIUMPH-1:
| Arm | Weight loss at 68 wk |
|---|---|
| Retatrutide 12 mg | -28.7% (-71.2 lbs) |
| Retatrutide 9 mg | -26.4% |
| Placebo | -2.1% |
The pain endpoint is what caught attention. WOMAC pain scores in the 12 mg arm fell by up to 4.5 points, a 75.8% relative reduction from baseline. More than 1 in 8 participants on retatrutide were completely pain-free at 68 weeks.
That magnitude of pain relief is hard to explain by weight loss alone. The standard model says load reduction at the knee improves function and pain, but the curves do not usually go this far. TRIUMPH-4 is the first Phase 3 readout suggesting GLP-1-receptor signaling, GIP, or glucagon may have direct effects on joint inflammation or central pain processing in addition to the mechanical relief from weight loss.
That hypothesis needs dedicated trials to confirm, but the size of the WOMAC effect is large enough that the question is no longer theoretical.
Bottom line: TRIUMPH-4 turned retatrutide from a weight-loss drug into a candidate for symptomatic knee OA, a population currently stuck between NSAIDs, intra-articular injections, and joint replacement.
The cancer signal nobody is leading with
Buried in the retatrutide literature is a preclinical paper that has not made it into most of the obesity-focused coverage. Marathe et al. (2025) in npj Metabolic Health and Disease reported what happens when you give retatrutide to obese mice carrying pancreatic and lung cancer cell lines.
In the pancreatic model, retatrutide delivered a 14-fold reduction in tumor volume compared to controls. Semaglutide in the same model produced a 4-fold reduction. In the lung model, retatrutide cut tumor engraftment by 50% and produced a 17-fold reduction in tumor volume.
The notable detail: when mice were taken off retatrutide and regained weight, the anti-tumor effect persisted. That suggests the mechanism is not purely "less obesity equals less cancer." Something about triple-G receptor activation appears to do work beyond weight loss alone.
This is preclinical. Mouse engraftment models do not always translate to human oncology. But the magnitude is large enough that the obesity-cancer link is now a real research question for the triple-G class, not a footnote. Expect dedicated oncology endpoints in the next wave of Phase 3 retatrutide programs.
Cardiometabolic effects nobody should sleep on
The primary endpoint was weight, but the secondary endpoints are arguably more important for long-term risk. In TRIUMPH-1, the 12 mg arm showed:
- Systolic blood pressure reduction of approximately -14 mmHg
- Significant improvements in non-HDL cholesterol, triglycerides, and total cholesterol
- Reductions in HbA1c despite enrolling people without diabetes
- Lower high-sensitivity C-reactive protein (hsCRP), a systemic inflammation marker
- Waist circumference reduction proportional to weight loss
A 14 mmHg drop in systolic BP is the kind of number you usually see in a hypertension trial, not a weight-loss trial. For context, achieving that with a typical antihypertensive requires either a thiazide-loop combination or RAAS blockade at full dose. Retatrutide is doing it as a metabolic side effect.
The same Phase 2 program also generated the Rosenstock et al. (2023) Lancet paper on retatrutide in type 2 diabetes, which showed HbA1c reductions up to 2.0 percentage points at the 12 mg dose. TRIUMPH-2, the Phase 3 readout in T2D, is expected later this year. If it confirms the Phase 2 glycemic effect, retatrutide will sit in three drug classes simultaneously: obesity, type 2 diabetes, and cardiometabolic risk reduction.
Safety profile and the dysesthesia signal that is new in Phase 3
The GI side effects look like every other GLP-1 trial. Nausea, diarrhea, constipation, vomiting, mostly mild to moderate, mostly during titration:
| Adverse event class | 12 mg arm | Placebo |
|---|---|---|
| Nausea | ~43% | ~10% |
| AE-driven discontinuation | 11.3% | 4.9% |
| Discontinuation at 9 mg | 6.9% | - |
| Discontinuation at 4 mg | 4.1% | - |
The new thing is dysesthesia. In TRIUMPH-1, dysesthesia (abnormal sensations: tingling, numbness, prickling, or unpleasant sensations on normal touch) was reported in:
- 0.7% of placebo participants
- 8.8% of 9 mg participants
- 20.9% of 12 mg participants
One in five people on the top dose. This signal did not show up in the Phase 2 program, which means dose plus duration plus the larger Phase 3 population is what surfaced it. Most events were classified as mild and did not lead to drug discontinuation, but a clinically detectable sensory effect in over 20% of patients on the top dose is the kind of finding that will be examined closely in the label and in TRIUMPH-2 and TRIUMPH-3.
The mechanism is unclear. Glucagon receptor activation has known effects on metabolic flux that could plausibly affect peripheral nerve function, but this is hypothesis. Lilly will need to characterize whether the signal is reversible, dose-dependent in the clinical sense, and whether titration speed changes its frequency.
Warning: A 20.9% dysesthesia rate at 12 mg is a real signal, not a footnote. If retatrutide reaches the market, expect the 12 mg label and titration schedule to look conservative.
Where retatrutide sits in the field now
The Phase 3 GLP-1 class field at top doses, in head-to-head-adjusted terms:
| Drug | Mechanism | Best Phase 3 weight loss | Timepoint |
|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 | -14.9% (STEP-1) | 68 wk |
| Tirzepatide 15 mg | GIP + GLP-1 | -20.9% (SURMOUNT-5) | 72 wk |
| Semaglutide 7.2 mg (HD) | GLP-1 high-dose | ~-20.7% (STEP UP) | 72 wk |
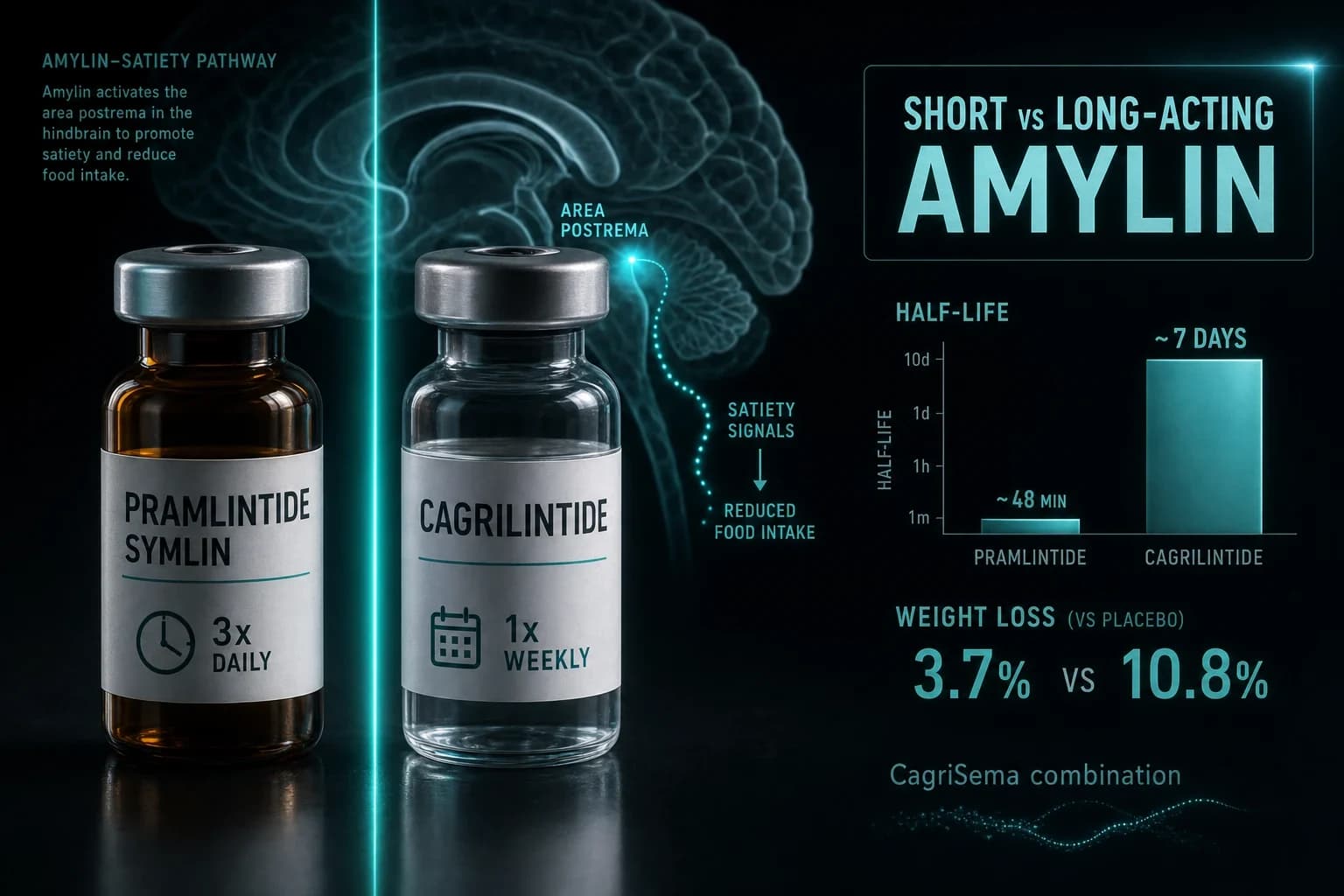
| Cagrilintide 2.4 mg + Semaglutide 2.4 mg | Amylin + GLP-1 | -20.4% (REDEFINE 1) | 68 wk |
| Retatrutide 12 mg | GIP + GLP-1 + GCG | -28.3% (TRIUMPH-1) | 80 wk |
| Retatrutide 12 mg (extension, BMI ≥35) | GIP + GLP-1 + GCG | -30.3% | 104 wk |
If the comparison were apples-to-apples on identical trial designs, the gap would tighten slightly. But the order is unambiguous: retatrutide sits at the top of the Phase 3 obesity ranking by 7 to 10 percentage points.
Our GLP-1 dosing comparison guide covers titration schedules across the class. The retatrutide vs tirzepatide vs semaglutide head-to-head goes deeper on the mechanism differences. For step-up dosing alongside the semaglutide high-dose program, see the Wegovy HD 7.2 mg trial guide.
What is still coming in the TRIUMPH program
TRIUMPH-1 and TRIUMPH-4 are two of nine Phase 3 trials in the retatrutide program. The remaining readouts and the populations they cover:
- TRIUMPH-2: Adults with type 2 diabetes (glycemic and weight endpoints)
- TRIUMPH-3: Adults with established cardiovascular disease (MACE outcomes)
- TRIUMPH-5: Sleep apnea
- TRIUMPH-6: Chronic low back pain
- TRIUMPH-7: Metabolic dysfunction-associated steatotic liver disease (MASLD)
- TRIUMPH-Outcomes: Long-term cardiometabolic outcomes
- Plus additional pediatric and special-population programs in setup
Additional TRIUMPH-1 detail is scheduled for the 86th American Diabetes Association Scientific Sessions in June, including secondary endpoints, subgroup analyses, and the full safety dataset. The FDA filing timeline based on Lilly's prior guidance points to a Q4 2026 NDA submission, with potential approval in 2027.
Bottom line: TRIUMPH-1 is the headline, but the program will not be fully characterized until the cardiovascular outcome data from TRIUMPH-3 lands. That readout is the one that will determine whether retatrutide replaces semaglutide and tirzepatide in cardiometabolic guidelines or sits alongside them as a higher-magnitude option.
FAQ
When will retatrutide actually be available?
Lilly is expected to file the NDA in Q4 2026 based on prior program guidance, with potential FDA approval in 2027. The TRIUMPH-2 (T2D) and TRIUMPH-3 (CV outcomes) readouts later this year will round out the regulatory package.
How is retatrutide different from tirzepatide?
Retatrutide activates three receptors (GIP, GLP-1, and glucagon). Tirzepatide activates two (GIP and GLP-1). The glucagon-receptor activation is what is hypothesized to drive the additional weight-loss magnitude in retatrutide via increased energy expenditure on top of the appetite suppression both drugs share.
Is 30.3% weight loss really comparable to bariatric surgery?
In magnitude, yes. Roux-en-Y gastric bypass typically produces 25-35% total weight loss at one to two years. Sleeve gastrectomy averages 20-30%. TRIUMPH-1's 12 mg arm at 80 weeks (-28.3%) and the BMI-35-plus extension (-30.3%) overlap with both procedures. The durability past 2 years remains to be established and will depend on whether patients can continue therapy long-term.
What is dysesthesia and should I be worried about it?
Dysesthesia is any abnormal sensation, often tingling, numbness, or unpleasant feeling on touch. In TRIUMPH-1, it affected 20.9% of patients on the 12 mg dose vs 0.7% on placebo. Most events were mild and did not lead to drug discontinuation, but it is a new signal that did not appear in Phase 2. Expect more characterization in TRIUMPH-2 and TRIUMPH-3 and in the eventual label.
Does retatrutide really reduce cancer risk?
In obese mice, yes, with large magnitude effects in pancreatic and lung models per Marathe et al. (2025). In humans, this has not been tested in a controlled trial. The TRIUMPH-Outcomes program is expected to capture cancer incidence as a secondary endpoint, but a dedicated oncology trial would be required to make a causal claim.
Why is retatrutide 12 mg so much harder to tolerate than 4 mg?
Higher dose, same titration steps. AE-driven discontinuation went from 4.1% at 4 mg to 11.3% at 12 mg. The trade-off is built in: the 4 mg dose produces 19% weight loss with the lowest discontinuation rate. The 12 mg dose produces 28.3% with three times the dropout risk. Clinical use will need to balance magnitude against tolerability per patient.
How does retatrutide compare to semaglutide on cardiometabolic markers?
Both drugs improve blood pressure, lipids, glycemia, and inflammation markers. The magnitude appears larger with retatrutide based on TRIUMPH-1 secondary endpoints (SBP -14 mmHg vs roughly -5 to -6 mmHg for semaglutide in STEP trials), but direct head-to-head comparisons are not yet available. TRIUMPH-3 will be the definitive cardiovascular readout.
Further reading
- Retatrutide vs tirzepatide vs semaglutide 2026 head-to-head
- Retatrutide where to buy 2026
- Retatrutide reconstitution guide for 30 mg vials
- GLP-1 dosing comparison guide 2026
- Tirzepatide vs semaglutide SURMOUNT-5 head-to-head evidence
- Wegovy HD 7.2 mg step-up trial guide
- Retatrutide compound guide
- Tirzepatide compound guide
- Semaglutide compound guide
- Cagrilintide compound guide
Shop retatrutide research at Ascension: 50% off with code ENHANCED
Research-grade injectable retatrutide is available from our partner Ascension Peptides with public per-batch COAs and cold-chain shipping. Code ENHANCED takes 50% off the entire catalog including retatrutide, tirzepatide, semaglutide, and cagrilintide.
For the deeper vendor evaluation, see the Ascension Peptides review 2026 and the best legit peptide vendors 2026 ranking.
This article is for educational and informational purposes only. Retatrutide is an investigational drug not yet approved by the FDA, EMA, or any major regulator for human use. Topline Phase 3 results have been disclosed by the sponsor but the full peer-reviewed publication, complete safety dataset, and regulatory review have not yet occurred. Nothing in this article constitutes medical advice or a recommendation to use retatrutide outside of an approved clinical trial. Always consult a qualified clinician before considering any GLP-1-class or triple-agonist therapy.