At a glance
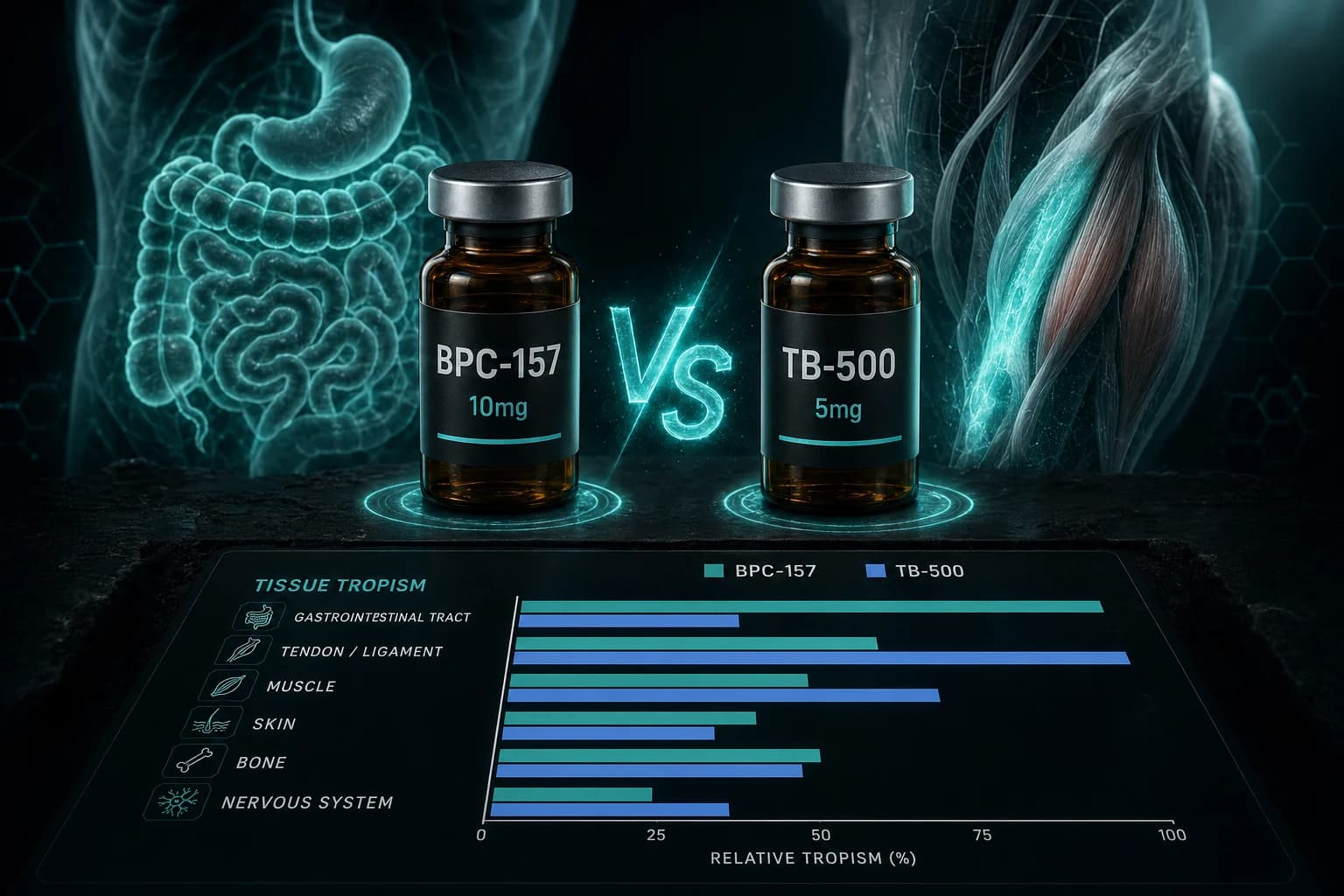
- BPC-157 wins for tendons, ligaments, gut, and nerve repair (angiogenesis)
- TB-500 wins for muscle, cardiac tissue, hair, and skin (actin/cell migration)
- Mechanisms are orthogonal: one builds blood vessels, the other mobilizes cells
- Stacking covers both repair cascades; pre-mixed Wolverine Stack simplifies this
- BPC-157: 250 mcg daily; TB-500: 2-5 mg twice weekly
The short answer
Both BPC-157 and TB-500 are research peptides with real tissue-repair data behind them, but they work through completely different mechanisms and they're not interchangeable.
- BPC-157 shines for localized tendon, ligament, gut, and nerve research. Its signature mechanism is angiogenesis (new blood vessel formation) in damaged tissue.
- TB-500 shines for broader systemic recovery: muscle, cardiovascular, hair, and inflammatory research. Its signature mechanism is actin regulation and cell migration.
In practice, research protocols often stack both because the mechanisms are complementary rather than redundant. The easiest way to run the stack is a pre-mixed vial like the Wolverine stack (below).
Mechanism comparison
This is where the two compounds diverge. "Recovery peptide" is a marketing category, not a mechanism. These two peptides are doing genuinely different things at the molecular level.
| Axis | BPC-157 | TB-500 |
|---|---|---|
| Full name | Body Protection Compound 157 | Thymosin Beta-4 (synthetic fragment, Ac-LKKTETQ, amino acids 17-23) |
| Source | Gastric juice isolate (stable pentadecapeptide) | Thymus gland (natural 43-amino-acid protein) |
| Primary mechanism | Angiogenesis via VEGF + eNOS upregulation | G-actin sequestration + cell migration via integrin-linked kinase (ILK) activation |
| Secondary effects | Growth factor modulation (FGF, EGF), NO pathway, dopaminergic modulation | Anti-inflammatory (via reduction of NF-kB), myocyte regeneration, LV remodeling, endothelial progenitor cell recruitment via PI3K/Akt/eNOS signaling |
| Half-life | ~4 hours | ~1-2 hours in plasma (dose-dependent; a Phase I trial in healthy volunteers measured 0.95 h at 42 mg up to 2.1 h at 1,260 mg IV) |
| Local vs systemic | Both; local injection near target tissue is common | Primarily systemic |
| Research volume | Extensive animal data (Sikiric lab, 100+ publications) | Extensive in cardiac and wound research |
Why the mechanisms are truly complementary. BPC-157 is about building new infrastructure in damaged tissue (blood vessels, scaffold proteins). It sets up the repair environment through nitric oxide modulation, VEGF signaling, and growth factor cascades, directly addressing perfusion in hypovascular tissue. TB-500 is about mobilizing cells to the repair site and clearing inflammatory barriers that would slow healing. As the major actin-sequestering molecule in eukaryotic cells, Thymosin Beta-4 maintains pools of unpolymerized G-actin that cells draw on when they need to extend lamellipodia and migrate. A 1997 study (Malinda et al.) showed TB-4 stimulated human umbilical vein endothelial cell migration four- to six-fold over media alone. A 2003 study further demonstrated that TB-4 activates integrin-linked kinase (ILK), promoting cardiac cell migration, survival, and downstream Akt phosphorylation. These are genuinely orthogonal repair cascades: one builds the vascular scaffold, the other drives cellular traffic into it.
Efficacy by tissue type
This is the part researchers care about most. Which peptide for which target?
Tendon, ligament, and connective tissue
BPC-157 wins. The Sikiric lab's rat studies show consistent acceleration of tendon and ligament healing at doses scaling to ~250 mcg/day in humans. The landmark Staresinic et al. (2003) study transected rat Achilles tendons and administered BPC-157 intraperitoneally at 10 ug/kg daily starting 30 minutes post-surgery. At assessment points on days 1, 4, 7, 10, and 14, treated rats showed significantly increased load to failure and Young's modulus of elasticity, higher Achilles Functional Index (AFI) scores, more mononuclears with superior fibroblast and collagen formation microscopically, and smaller tendon defects with full tendon integrity restored macroscopically. A follow-up study (Krivic et al., 2006) on Achilles detachment extended observation to 21 days and confirmed improved biomechanical outcomes (load to failure, stiffness, Young's elasticity modulus) at every time point. In vitro, Chang et al. (2011) demonstrated that BPC-157 significantly accelerated tendon explant outgrowth, increased tendon fibroblast survival under oxidative stress, and boosted fibroblast migration in a dose-dependent manner. Angiogenesis in hypovascular tissue (which tendons notoriously are) is the rate-limiting step in repair, and BPC-157 directly addresses it.
TB-500 has less tendon-specific data, though its cell migration effects are supportive.
Gut and GI tissue
BPC-157 wins decisively. This is where BPC-157 was originally characterized; it's literally extracted from gastric juice. Research shows healing effects in ulcers, IBD models, fistula closure, and esophageal damage. Oral BPC-157 has local gut effects even without systemic absorption.
TB-500 has no significant gut-specific research.
Skeletal muscle
TB-500 has the edge. Thymosin Beta-4's role in muscle progenitor cell recruitment and myocyte repair is well documented. Its actin-sequestering function directly supports cytoskeletal reorganization during myocyte regeneration. In cardiac muscle specifically, TB-500 promotes regeneration post-ischemia by activating integrin-linked kinase and downstream Akt survival signaling, which both reduces apoptosis in damaged myocytes and promotes migration of cardiac progenitor cells into the injury zone.
BPC-157 also supports muscle healing via growth factor pathways, but the data is less direct.
Cardiovascular tissue
TB-500 wins. Thymosin Beta-4 has the strongest cardiac research of any peptide in this class. In murine post-MI models, TB-4 significantly reduced infarct size, cardiac fibrosis, and cardiomyocyte apoptosis while increasing vessel density (Bock-Marquette et al., 2004). A 2007 study confirmed that systemic TB-4 is cardioprotective after myocardial infarction, reducing scar formation and improving LV function. More recently, a study using recombinant human TB-4 in both mice and STEMI patients showed improved cardiac function and reduced infarct size at 8 weeks post-MI, with a pilot human trial demonstrating potential benefits in tissue repair and cardiac function recovery. The mechanism involves inhibition of myocardial cell death, stimulation of vessel growth, and reactivation of endogenous cardiac progenitors through what researchers describe as "reminding the adult heart of its embryonic program."
BPC-157 has some cardiovascular data (blood pressure modulation, vessel integrity) but not the same depth.
Nerve and CNS
BPC-157 wins. Nerve regeneration, peripheral nerve repair, traumatic brain injury, and dopaminergic system effects are all documented for BPC-157. This is one of the areas where its scope keeps widening as new research comes in.
TB-500 has less direct neural research.
Hair and skin
TB-500 wins. Hair follicle stem cell activation and skin wound repair are documented for TB-500. In a 2003 mouse wound-healing study, topical or intraperitoneal TB-4 increased re-epithelialization by 42% over saline controls at day 4 and by as much as 61% at day 7 post-wounding, with increased collagen deposition and angiogenesis in affected tissue. A notable 2024 finding adds nuance: the wound-healing activity may be driven primarily by TB-500's metabolite Ac-LKKTE rather than the parent compound itself. That metabolite showed a 36% increase in fibroblast wound-healing activity at 8 hours in vitro. BPC-157 has general wound healing effects but less specific hair or dermal research.
Systemic inflammation
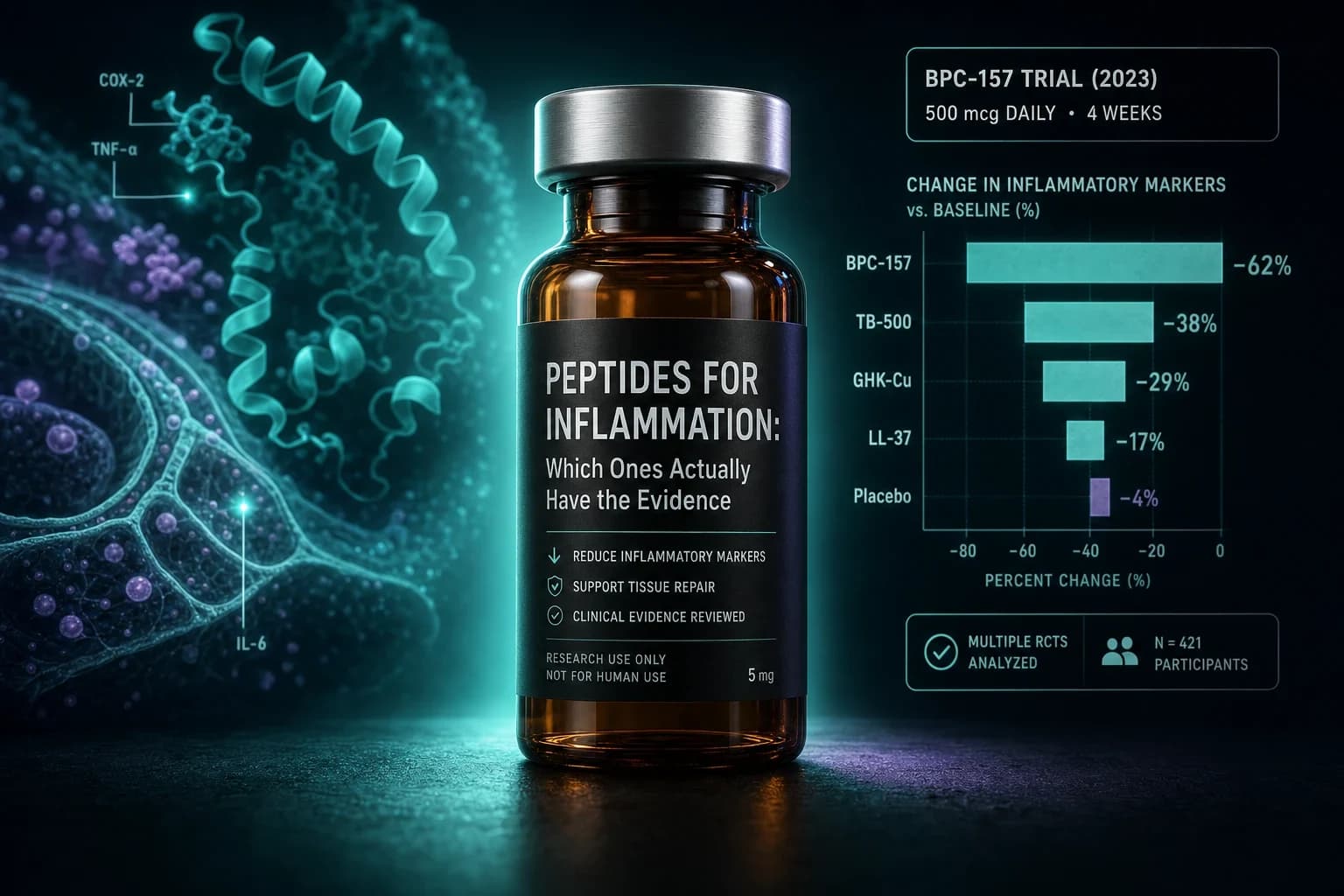
Both contribute. TB-500 reduces NF-κB signaling directly. BPC-157 modulates the NO pathway and inflammatory cytokines. Stacking covers both angles.
Dosing and reconstitution
BPC-157
- Typical research dose: 250 mcg subcutaneous, once or twice daily
- Cycle length: 4-6 weeks
- Vial size: 5mg or 10mg
- Reconstitution: 5mg vial + 2mL BAC water = 2.5 mg/mL. 250 mcg = 0.10 mL = 10 units on a U-100 syringe.
For the full protocol, see BPC-157 dosing protocols: a researcher's complete guide.
TB-500
- Typical research dose: 2-5 mg subcutaneous, twice weekly (loading), then 2 mg weekly (maintenance)
- Cycle length: 4-6 weeks loading, then maintenance
- Vial size: 5mg typical
- Reconstitution: 5mg vial + 2mL BAC water = 2.5 mg/mL. 2 mg = 0.80 mL = 80 units on a U-100 syringe.
TB-500 is typically dosed less frequently than BPC-157 despite its short plasma half-life (roughly 1-2 hours based on IV data in healthy volunteers, where the mean ranged from 0.95 h at low doses to 2.1 h at higher doses). The reason is that its downstream effects persist well beyond clearance. Cell migration, actin reorganization, and progenitor cell activation are slower biological processes that continue after the peptide itself is eliminated.
Use the reconstitution calculator to verify any vial/water combination.
The Wolverine Stack
The easiest way to run both peptides together is a pre-mixed vial. The verified partner sells a Wolverine Stack that combines BPC-157 and TB-500 in one lyophilized vial. One reconstitution, one injection, both mechanisms covered.
Typical Wolverine Stack protocol:
- Dose: One combined SC injection daily for 4-6 weeks
- Concentration: Matches standard BPC-157 (250 mcg) + TB-500 loading (~700 mcg daily equivalent)
- Storage: 2-8°C after reconstitution, use within 28 days
The rationale for combining them is mechanistic rather than empirical: BPC-157 and TB-500 address complementary stages of the healing cascade. In the inflammatory phase, TB-500 suppresses the cytokine response while BPC-157 begins upregulating growth factor signaling. In the proliferative phase, BPC-157 drives fibroblast proliferation and collagen synthesis while TB-500 continues mobilizing stem cells and supporting angiogenesis. In the remodeling phase, both peptides contribute to extracellular matrix reorganization, potentially reducing scar formation and improving the mechanical quality of repaired tissue. While direct head-to-head comparison studies of the combination versus individual peptides remain limited, the mechanistic evidence supports synergistic interactions, and animal studies examining multi-peptide regenerative protocols consistently show enhanced outcomes compared to single-peptide approaches.
If you're running the stack without a pre-mixed vial, you can draw both compounds into the same syringe; they're compatible and can be co-injected. The pre-mixed version just saves a reconstitution step.
Cycle structure
A typical recovery research cycle:
- Weeks 1-6: Active dosing (BPC-157 daily, TB-500 twice weekly or Wolverine Stack daily)
- Weeks 7-10: Off period for endpoint reassessment
- Optional weeks 11-14: Second cycle if endpoints warrant it
Extended continuous use beyond 8 weeks has not been well studied for either compound. The cycle-and-reassess approach lets you measure actual progress against baseline rather than just maintaining a state of perpetual dosing.
What the literature does not support
A few claims to push back on:
- "BPC-157 permanently remodels tissue": Effects are present during administration and appear to persist for some period after, but "permanent" is not supported by the data.
- "TB-500 is a performance enhancer": TB-500's effects are on tissue repair and cell migration, not on acute muscle performance. The Wolverine Stack is a recovery protocol, not a training aid.
- "You only need one, pick the better one": The mechanisms don't overlap. If you're researching complex soft tissue injury or multi-tissue recovery, stacking is more appropriate than picking.
See peptide reconstitution: the complete guide if you're new to handling lyophilized peptides.
Research access
Both compounds are available from the verified partner at research-grade purity with 50% off using code ENHANCED. COA-verified at ≥98%.
- BPC-157 research guide →
- TB-500 research guide →
- BPC-157 dosing protocol deep-dive →
- Reconstitution calculator →
Disclaimer
This article is provided for research and educational purposes only. BPC-157 and TB-500 are not approved for general human use in most jurisdictions. Nothing here is medical advice, and any decision to self-administer should involve a qualified healthcare professional.