At a glance
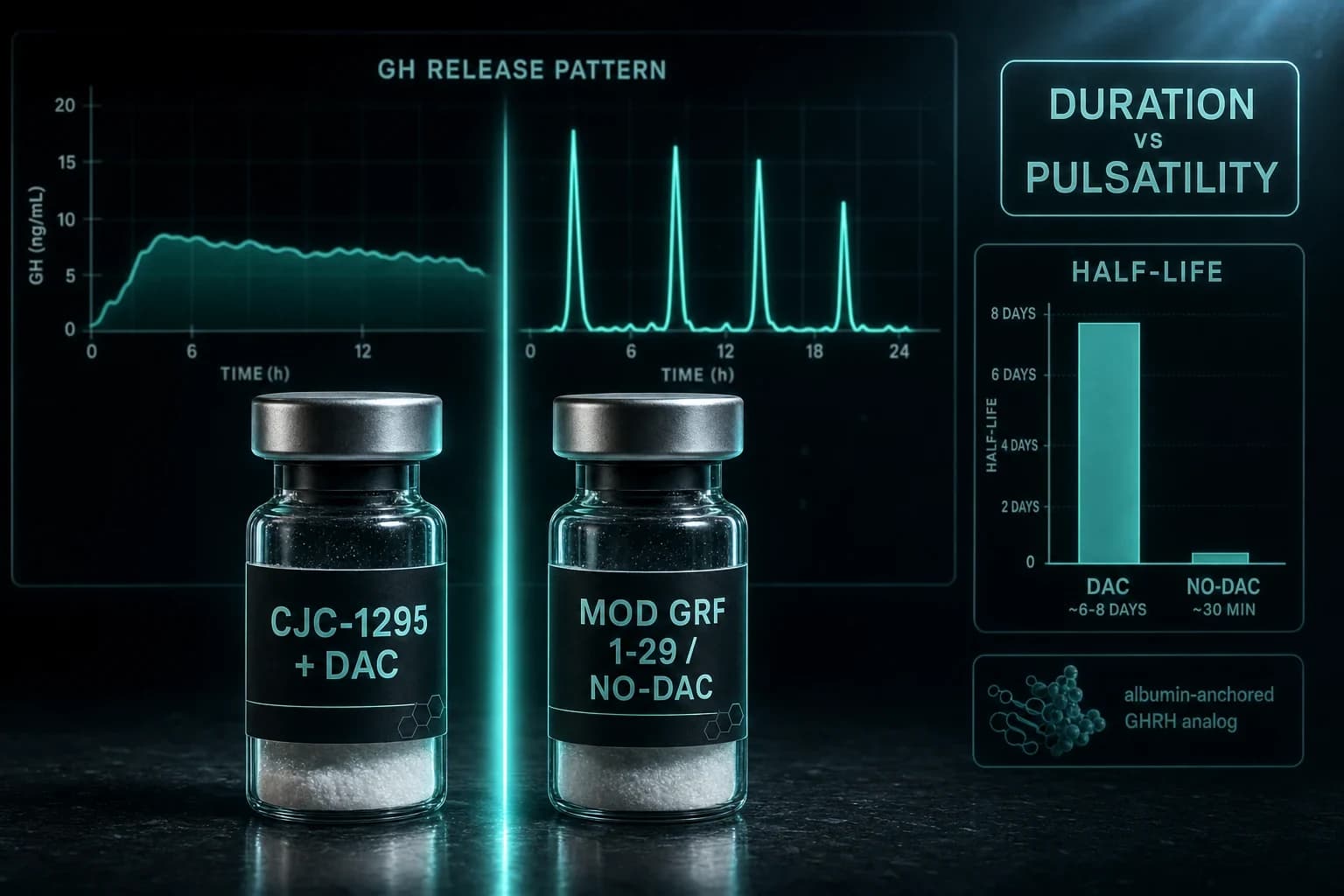
- CJC-1295 with DAC has a 6-8 day half-life; Modified GRF 1-29 clears in about 30 minutes.
- With-DAC means 1-2 injections per week and steady IGF-1; no-DAC means 1-3 daily pulses that track natural GH rhythm.
- Teichman 2006: one CJC-1295 DAC dose raised GH 2- to 10-fold for 6+ days and IGF-1 for 9-11 days.
- Ionescu & Frohman 2006: with-DAC kept GH pulse frequency intact while lifting trough GH roughly 7.5-fold.
- Both are paired with a GHRP like Ipamorelin because GHRH and ghrelin-mimetics hit separate receptors and stack.
Same peptide backbone. Same four amino acid swaps. Same receptor. The only thing that separates CJC-1295 with DAC from Modified GRF 1-29 is a single molecular hook that decides whether the compound leaves your bloodstream in half an hour or hangs around for a week. That one difference changes your injection schedule, your IGF-1 curve, and whether your growth hormone comes out in clean pulses or a steady drip.
If you have been told these are two different drugs, that is the first thing to unlearn. They are the same tetra-substituted analog of GHRH(1-29). One wears an anchor. The other does not.
The only real difference is a molecular anchor
Both compounds start from the same place: the first 29 amino acids of growth hormone-releasing hormone, the signal your hypothalamus normally sends to your pituitary to release GH. Native GHRH(1-29) is Sermorelin, and it is fragile. Dipeptidyl peptidase-4 (DPP-4) chops it at position 2 within minutes, so its half-life sits around 7 minutes.
To fix that, chemists made four substitutions to the sequence: D-Ala at position 2 to block DPP-4, plus Gln at 8, Ala at 15, and Leu at 27 to resist deamidation and enzymatic clipping. That tetra-substituted molecule is Modified GRF 1-29, also sold as CJC-1295 without DAC. The swaps push the half-life to roughly 30 minutes. Better, but still short.
Now the fork in the road. DAC stands for Drug Affinity Complex. It is a maleimidopropionamide group attached to a lysine at the C-terminus of the same tetra-substituted peptide. Once injected, that group forms a covalent bond with the free thiol on Cys34 of your own serum albumin. Jetté et al. (2005) demonstrated exactly this in rats and named the winning candidate CJC-1295, showing it was still present in plasma beyond 72 hours while the unmodified peptide was long gone. Bolt the peptide to albumin, a protein that circulates for weeks, and you drag the whole thing's clearance out with it.
That is the entire story. CJC-1295 with DAC is Modified GRF 1-29 plus an albumin anchor. Receptor binding is identical. The DAC does not make it stronger at the pituitary. It makes it last.
What the human data actually shows
This is not theory built on forum posts. CJC-1295 with DAC has real human pharmacokinetics.
Teichman et al. (2006), published in the Journal of Clinical Endocrinology & Metabolism, dosed healthy adults with single subcutaneous injections. A single shot produced dose-dependent increases in mean GH of 2- to 10-fold that lasted 6 days or more, and IGF-1 rose 1.5- to 3-fold for 9 to 11 days. The estimated half-life came in at 5.8 to 8.1 days. After repeated dosing, IGF-1 stayed above baseline for up to 28 days, and the compound was well tolerated at 30 and 60 mcg/kg.
Read that timeline again. One injection, and IGF-1 is still elevated a week and a half later. That is the selling point of the DAC version, and it is also the source of every concern about it.
The obvious worry is that a permanently elevated GHRH signal would flatten your GH into a tonic, always-on bleed instead of the sharp pulses your body normally produces overnight. Ionescu and Frohman (2006) tested that directly with 20-minute blood sampling in healthy men. The result was more reassuring than expected: GH pulse frequency and amplitude were unchanged one week after a CJC-1295 injection. What changed was the floor. Trough GH concentrations rose roughly 7.5-fold and mean 24-hour GH climbed about 45 percent.
So with-DAC does not erase your pulses. It lifts the entire baseline underneath them. You still pulse, but you never come back down to a true resting level, and IGF-1 tracks that sustained exposure.
With-DAC vs no-DAC at a glance
| Feature | CJC-1295 with DAC | Modified GRF 1-29 (no-DAC) |
|---|---|---|
| Half-life | ~6-8 days (Teichman 2006) | ~30 minutes |
| Dosing frequency | 1-2x per week | 1-3x per day |
| GH release pattern | Pulses preserved on a raised baseline (elevated trough) | Sharp, discrete pulses that return to baseline |
| IGF-1 effect | Sustained elevation for days | Short, pulse-linked spikes |
| Albumin binding | Yes, covalent to Cys34 | No |
| Best use | Convenience, steady IGF-1, minimal injections | Physiologic rhythm, tight GHRP timing, IGF-1 control |
Bottom line: With-DAC trades pulsatility purity for convenience and a raised IGF-1 floor. No-DAC trades convenience for pulses that look like your own biology. Neither is objectively better. They solve different problems.
Why pulsatility is the whole argument
Your body does not release GH in a smooth stream. It fires in bursts, mostly during slow-wave sleep, with long quiet troughs in between. Those troughs matter. The low periods are when somatostatin (your body's GH brake) resets receptor sensitivity. Chronically flooding the system can, in theory, blunt that responsiveness over time.
This is why some researchers prefer the no-DAC route. Modified GRF 1-29 spikes GH and clears within about 30 minutes, letting you come all the way back to baseline before the next dose. The pattern is closer to how a healthy hypothalamus behaves. Walker (2006) made this argument for Sermorelin specifically, favoring analogs that preserve the physiologic feedback loop rather than override it, because the pituitary itself sets the ceiling and protects against runaway GH exposure.
The counterpoint is practical. Preserving perfect pulsatility means injecting one to three times a day, every day, ideally on an empty stomach and away from meals. Miss doses and the theoretical advantage evaporates. With-DAC asks for one or two injections a week and never lets you fall behind. For many protocols, adherence beats elegance.
It is worth noting that with-DAC did not actually abolish pulses in the Ionescu data. It raised the trough. Whether a permanently elevated trough is a feature (steady anabolic signaling) or a flaw (loss of the low-GH recovery windows) is the real debate, and it depends on what you are trying to study.
Why neither one flies solo
Here is the part most comparisons skip. Both CJC-1295 with DAC and Modified GRF 1-29 are almost always paired with a growth hormone-releasing peptide (GHRP) such as Ipamorelin or GHRP-6. Running a GHRH analog alone leaves most of its potential on the table.
The reason is receptor biology. GHRH analogs bind the GHRH receptor. GHRPs bind a completely separate receptor, the ghrelin receptor (GHS-R). They pull different levers on the same somatotroph. GHRH primes the cell and increases the number of cells that respond. A GHRP amplifies the burst and suppresses somatostatin, releasing the brake at the same moment GHRH hits the accelerator. Together they produce a GH pulse larger than the sum of either alone.
Ipamorelin is the usual partner because it is clean. Raun et al. (1998) characterized it as the first selective GH secretagogue: even at doses more than 200-fold above the ED50 for GH release, it did not meaningfully raise ACTH, cortisol, prolactin, FSH, LH, or TSH. That selectivity is why it is preferred over older GHRPs like GHRP-6, which spikes hunger and cortisol.
The pairing logic differs slightly by version:
- No-DAC + GHRP: Both peptides are short-acting, so you time them together, one to three times daily. Each injection creates a coordinated pulse. This is the tightest, most pulse-faithful protocol.
- With-DAC + GHRP: The GHRH signal is always on in the background, so a GHRP dose can trigger a strong pulse at any time. Some run the GHRP separately from the weekly CJC-1295 injection to shape when the biggest bursts land.
Bottom line: Choosing between with-DAC and no-DAC is really a question about your GHRP schedule. If you want pulses on your terms, no-DAC gives you control over timing. If you want a standing GHRH signal and flexible GHRP timing, with-DAC handles the background for you.
Which one fits your protocol
Match the tool to the goal rather than chasing the longer half-life for its own sake.
Reach for CJC-1295 with DAC when:
- Injection frequency is the limiting factor and once- or twice-weekly dosing keeps a protocol on track.
- The objective is sustained IGF-1 elevation, and the Teichman data on multi-week IGF-1 persistence is the point.
- Coordinating multiple daily injections around meals is not realistic.
Reach for Modified GRF 1-29 when:
- Preserving a physiologic pulsatile pattern matters more than convenience.
- Tighter control over IGF-1 exposure is preferred, since the short half-life lets levels fall between doses.
- The plan already involves daily GHRP dosing, so adding the no-DAC GHRH to those same injections costs nothing extra in needles.
For context, Sermorelin sits at the far pulsatile end of this spectrum: native sequence, ~7 minute half-life, the most physiologic and the least durable. Modified GRF 1-29 is the upgraded, slightly longer version of that same philosophy. CJC-1295 with DAC is the opposite design choice, engineered for duration over rhythm.
Reconstitution and dosing notes
Both come as lyophilized powder and need reconstitution with bacteriostatic water. The dosing math is where people go wrong, because a with-DAC weekly dose and a no-DAC per-injection dose are not interchangeable numbers, and a typical Modified GRF 1-29 dose is often in the ~100 mcg range per injection while CJC-1295 with DAC is dosed by body weight and taken far less often. Draw the wrong volume and you are either underdosing or wasting an expensive vial.
Run your specific vial size and target dose through the reconstitution calculator before you draw anything. It converts your mg of peptide and mL of water into exact unit marks on the syringe, which removes the most common source of protocol error.
Both peptides, and Ipamorelin to pair with them, are available from Ascension Peptides with 50% off using code ENHANCED.
The honest summary
CJC-1295 with DAC and Modified GRF 1-29 are the same molecule wearing different clothes. The DAC anchor stretches a 30-minute peptide into a 6-to-8-day one, which buys convenience and steady IGF-1 at the cost of ever returning to a true GH baseline. The no-DAC version keeps the pulses clean and physiologic but demands daily discipline. The human data from Teichman and from Ionescu and Frohman shows the with-DAC version works and preserves pulse frequency; the argument against it is philosophical, about whether a raised trough is what you want. Whichever you choose, pair it with a selective GHRP like Ipamorelin, because a GHRH analog alone is running on one cylinder.
This article is for research and educational purposes only. It is not medical advice. The peptides discussed are not approved by the FDA for the uses described and are intended for laboratory research use only. Consult a qualified healthcare professional before making any decisions related to health or supplementation.