At a glance
- Karakasis 2026 meta-analysis (Metabolism, overweight/obesity RCTs): GLP-1 RAs and incretin co-agonists cut AF risk 18% vs placebo (RR 0.82, 95% CI 0.70 to 0.96, P=0.012, I-squared 0%).
- SELECT subanalysis (Plutzky 2025, n=17,604): once-weekly semaglutide 2.4 mg reduced first AF event vs placebo (HR 0.83, 95% CI 0.70 to 0.99, P=0.040).
- HFpEF/HFmrEF pooled meta-analysis (PMID 41216984, 4 trials, 3,743 patients): incident AF cut 46% (RR 0.54, 95% CI 0.36 to 0.81, P=0.003).
- Post-ablation real-world cohort (Patel 2025, J Cardiovasc Electrophysiol): AF recurrence requiring care HR 0.84 (95% CI 0.78 to 0.91, P<0.0001) on GLP-1 RA vs not.
- Effects appear class-level. No subgroup difference across single, dual, or triple incretin agonists, and no effect modification by magnitude of weight loss or SGLT2 inhibitor co-use.
- No GLP-1 RA carries an AF prevention, rhythm, or recurrence indication in mid-2026. Any AF use is off-label and outside guideline recommendations.
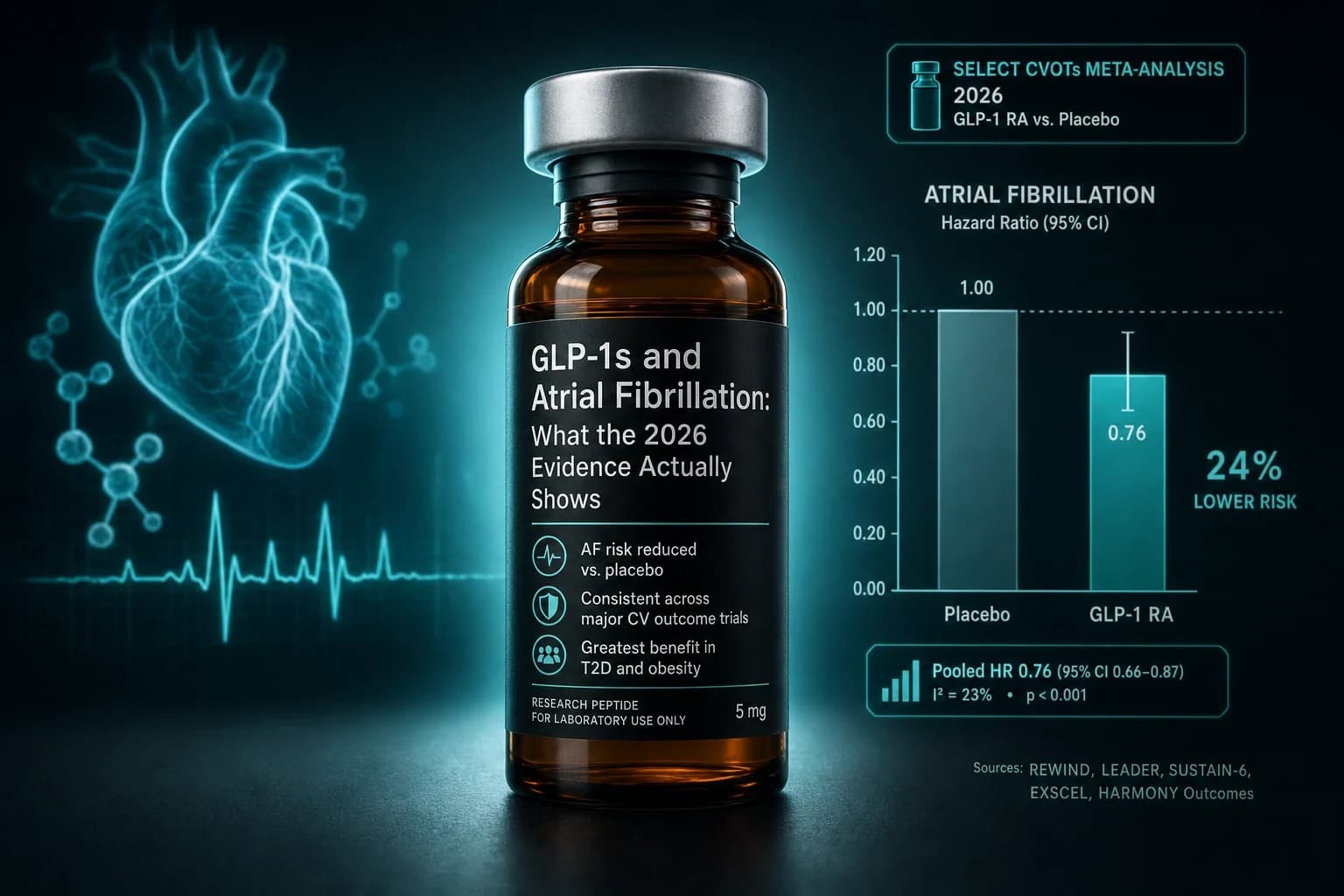
In February 2026, Metabolism published the cleanest meta-analysis the field has on GLP-1 receptor agonists and atrial fibrillation. The pooled risk ratio across randomized trials in overweight and obesity came in at 0.82, with a 95% confidence interval of 0.70 to 0.96 and a P value of 0.012. Heterogeneity was effectively zero. That is an 18 percent relative reduction in incident AF on drug versus placebo, holding consistent across single, dual, and triple incretin agonists (Karakasis et al., Metab Clin Exp 2026, PMID 41349790).
That number sits inside a larger story. Six weeks later, ESC 2025 published a pooled SELECT subanalysis showing a 17 percent reduction in first AF events on semaglutide 2.4 mg in 17,604 patients with established cardiovascular disease and obesity. A separate 2025 meta-analysis restricted to four trials in heart failure with preserved or mildly reduced ejection fraction (n=3,743) found incident AF down 46 percent. Post-ablation real-world data from a 2025 cohort showed AF recurrence requiring care down about 16 percent on GLP-1 RA exposure.
The signal is unusually internally consistent for a secondary endpoint. The clinical interpretation is more careful than the headlines: GLP-1 RAs are not approved for AF, no Phase 3 trial has used AF as a primary endpoint, and the magnitude of the effect appears to track weight loss and adiposity reduction more than direct ion-channel pharmacology. This article maps every important data point and what it does and does not justify.
Bottom line: Across 2024-2026 randomized-trial meta-analyses, the SELECT subanalysis, HFpEF data, and post-ablation real-world cohorts, GLP-1 receptor agonist exposure tracks lower atrial fibrillation incidence and lower post-ablation recurrence. The relative reductions span roughly 17% to 46% depending on the population. No GLP-1 RA carries an AF indication in mid-2026, and the most likely driver is reduced obesity-related atrial remodeling rather than a direct anti-arrhythmic effect.
Why the AF question matters for GLP-1 users
Atrial fibrillation is the most common sustained arrhythmia in adults, and the populations most likely to be on a GLP-1 receptor agonist (obesity, type 2 diabetes, established cardiovascular disease, heart failure with preserved ejection fraction) overlap heavily with the populations most likely to develop new AF or to recur after ablation. Obesity is an independent AF risk factor with a dose-response relationship, and intentional weight loss reduces AF burden and recurrence in dedicated cardiology cohorts. The LEGACY and CARDIO-FIT programs from the late 2010s established that 10 percent or greater sustained weight loss roughly halves recurrent AF in obese patients, which is the kind of magnitude that has been hard for any single pharmacotherapy to match without rhythm-directed mechanism.
That is the prior. Drop in semaglutide 2.4 mg, tirzepatide, retatrutide, the GLP-1 plus amylin combinations, and now the GLP-1 plus glucagon dual agonists, and the question becomes whether the weight-loss-mediated AF benefit is automatic, whether there is an additional drug-specific signal, and whether GLP-1 RAs should be considered as adjuncts in patients who have AF history independent of metabolic indication. The 2026 evidence allows partial answers to all three.
It also matters in the other direction. A small number of case reports have described new-onset AF temporally associated with tirzepatide initiation, and some early observational signals raised whether the rapid heart-rate increase that is well-described for the GLP-1 RA class translates into clinically meaningful arrhythmia risk. The randomized data settle that question on the side of net benefit, not net harm, and this article walks through where each data point lands.
The 2026 Karakasis meta-analysis: the cleanest signal so far
The headline 2026 publication is Karakasis et al., Metab Clin Exp 2026 (PMID 41349790), published in Metabolism: Clinical and Experimental. The authors pooled randomized controlled trials of GLP-1 receptor agonists and their co-agonists (dual GLP-1/GIP and triple GLP-1/GIP/glucagon agents) versus placebo in adults with overweight or obesity. Outcomes were incident atrial fibrillation as reported during the trial.
The pooled relative risk was 0.82, with a 95% confidence interval of 0.70 to 0.96 and a P value of 0.012. The I-squared statistic was zero, meaning the included trials pulled in the same direction with no measurable between-study heterogeneity. That is a quality marker. A zero I-squared on an event-driven cardiovascular endpoint pooled across multiple compounds is uncommon in this field, and it points either to a real class effect or to a shared upstream mediator (weight loss) doing most of the work.
The subgroup analyses are where the article earns its rigor. The authors specifically tested whether the AF reduction differed by class generation (single incretin agonist versus dual or triple), by magnitude of weight reduction, and by SGLT2 inhibitor co-prescription. None of those subgroup tests reached significance for effect modification. In plain language: the AF benefit looks like a class signal that tracks weight loss but is not gated on hitting a specific weight-loss threshold, and it does not appear to be amplified or blunted by SGLT2 inhibitor co-use within the trials examined.
A commentary in the same journal raised data-duplication and uncertainty concerns about the pooled estimate (Metab Clin Exp 2025, S0026-0495(25)00360-9), arguing that some patient-level overlap between included trials could narrow the true confidence interval. That critique is legitimate. The authors' response, and the broader pattern of consistent direction across independent meta-analyses, supports treating the 18 percent reduction as a defensible point estimate with the standard caveats that always apply to secondary-endpoint pooling.
The SELECT subanalysis: a single-trial confirmation in 17,604 patients
The single most-discussed data point is the SELECT trial's pre-specified AF analysis. SELECT randomized 17,604 patients aged 45 and older with established atherosclerotic cardiovascular disease and overweight or obesity but without diabetes to once-weekly semaglutide 2.4 mg or placebo, with a primary MACE endpoint. The AF subanalysis was presented at ESC 2025 by Plutzky and colleagues and published in the European Heart Journal supplement (Plutzky et al., Eur Heart J 2025, supplement 46(Suppl_1):ehaf784.4243).
The risk of a first AF event in the overall SELECT cohort was lower on semaglutide than on placebo: hazard ratio 0.83, 95% CI 0.70 to 0.99, P=0.040. The authors reported a 27 percent reduction in AF recurrence among the subset with a history of AF at baseline. The trial design did not power AF as a primary endpoint and AF was ascertained from investigator-reported adverse events plus adjudicated cardiovascular events, which is the standard but imperfect way to capture asymptomatic or silent AF.
What SELECT adds beyond the meta-analytic estimate is patient-level signal in a single, large, double-blind randomized trial. Karakasis et al. is a pooled estimate that depends on trial-level summary data. SELECT is one trial that contributed to several of those pooled estimates, and the within-trial result lines up with the pooled one within a few percentage points of relative risk reduction. The two should not be averaged. They should be read as the same finding viewed from two angles.
The other point worth making is that SELECT also showed reductions in cardiovascular mortality, MI, and stroke, with HRs around 0.80 across MACE components. That broader pattern is consistent with semaglutide modifying the cardiometabolic substrate that drives AF, not specifically with semaglutide targeting AF as such. For the deeper SELECT walkthrough on hard cardiovascular endpoints, the SELECT cardiovascular MACE evidence breakdown covers the primary trial.
The HFpEF data: a larger relative reduction in a higher-risk substrate
A 2025 meta-analysis published just ahead of the Karakasis paper looked at the narrower question of incident AF in patients with HFpEF or HFmrEF on GLP-1 RA therapy (PMID 41216984). The authors searched through February 2025 and identified four randomized trials (SELECT, FLOW, STEP-HFpEF, STEP-HFpEF DM) reporting incident AF in patients with preserved or mildly reduced ejection fraction, enrolling 3,743 participants total.
The pooled risk ratio was 0.54, with a 95% CI of 0.36 to 0.81 and a P value of 0.003. That is a 46 percent relative reduction, roughly double the magnitude of the all-obesity Karakasis estimate. Heterogeneity was moderate, meaning the trials did not all line up identically, but the direction was consistent. Secondary outcomes showed significantly greater reductions in body weight, systolic blood pressure, and left atrial volume in the treatment group.
There are two plausible reasons the HFpEF magnitude looks larger. The first is selection. HFpEF patients have a much higher baseline AF risk, which means even modest absolute risk reductions translate into larger relative effect sizes. The second is mechanism. HFpEF in obesity is often driven by atrial myopathy, left atrial enlargement, and epicardial adipose tissue expansion. Each of those substrates is plausibly more responsive to a strong GLP-1-driven weight loss than is the AF substrate in a metabolically intact 50-year-old.
For the underlying HFpEF trial reads, the semaglutide HFpEF STEP trial evidence and tirzepatide HFpEF SUMMIT trial evidence cover the parent trials in detail. The AF signal in this population is one of the cleanest secondary endpoints in the entire GLP-1 RA cardiovascular literature.
Post-ablation evidence: the question every electrophysiologist is asking
Patients who undergo catheter ablation for AF have roughly a 30 to 40 percent recurrence rate at one year, and obesity is among the most modifiable predictors of that recurrence. The post-ablation literature on GLP-1 RAs has accumulated quickly across 2024-2026.
The most-cited individual study is Patel et al., J Cardiovasc Electrophysiol 2025 (PMID 40406931), a real-world propensity-matched cohort of obese patients undergoing AF ablation. Over a median follow-up of 1.6 years, GLP-1 RA users had an AF recurrence rate (defined as recurrence requiring hospitalization or outpatient visit) of 7.43 percent versus 8.40 percent on no GLP-1 RA, for a hazard ratio of 0.843 (95% CI 0.780 to 0.911, P<0.0001). The GLP-1 RA group also had a lower rate of progression to permanent AF (HR 0.743, 95% CI 0.610 to 0.905, P=0.003) and lower all-cause mortality (HR 0.700, 95% CI 0.553 to 0.887, P=0.003).
A 2026 random-effects meta-analysis by Shubietah et al. published in Pacing and Clinical Electrophysiology (DOI 10.1111/pace.70262) pooled five post-ablation studies and reported HR 0.78 (95% CI 0.61 to 0.99) for AF recurrence with peri- or post-ablation GLP-1 RA therapy versus no GLP-1 RA. Pairwise analyses at 12 months showed AF recurrence of 28.6 percent on GLP-1 RA versus 32.9 percent off (RR 0.82, 95% CI 0.76 to 0.90).
An earlier 2024 single-study analysis using TriNetX data and propensity matching investigated the same question in a different cohort (PMID 38795099). The authors examined GLP-1 RA use within the year before ablation versus no use, with similar directional findings. That study did not have the same follow-up duration as Patel et al. but contributed to the early signal.
A new 2025 propensity-matched real-world dataset from a separate group (PMID 41446932) reinforced the pattern, with GLP-1 RA use associated with lower AF recurrence, lower progression to permanent AF, fewer heart failure hospitalizations, and lower mortality. The methodological caveat across all these studies is that propensity matching on EHR data cannot control for unmeasured prescribing-related selection. A rigorous randomized ablation trial has not yet completed. Ongoing trials (GOAL-AF, SWGLP-AF) are designed to confirm the recurrence signal under randomization with structured AF burden monitoring.
Side-by-side: the AF datasets that move the conversation
| Source | Study type | Population | Comparator | Primary AF result |
|---|---|---|---|---|
| Karakasis 2026 (PMID 41349790) | Meta-analysis of RCTs | Overweight/obesity adults | Placebo | Incident AF RR 0.82 (95% CI 0.70-0.96), P=0.012, I-sq 0% |
| SELECT AF subanalysis (Plutzky 2025) | Pre-specified single-trial subanalysis | 17,604 ASCVD + obesity, no diabetes | Placebo (semaglutide 2.4 mg) | First AF HR 0.83 (95% CI 0.70-0.99), P=0.040; AF recurrence reduced 27% in baseline-AF subset |
| HFpEF meta-analysis (PMID 41216984) | Meta-analysis of 4 RCTs (SELECT, FLOW, STEP-HFpEF, STEP-HFpEF DM) | 3,743 HFpEF/HFmrEF | Placebo | Incident AF RR 0.54 (95% CI 0.36-0.81), P=0.003 |
| Patel 2025 (PMID 40406931) | Real-world propensity-matched cohort | Obese AF ablation patients, median 1.6 yr | No GLP-1 RA | Recurrence HR 0.843 (95% CI 0.780-0.911), P<0.0001 |
| Shubietah 2026 (DOI 10.1111/pace.70262) | Meta-analysis of 5 post-ablation studies | Mixed obesity/T2D ablation cohorts | No GLP-1 RA | Recurrence HR 0.78 (95% CI 0.61-0.99); 12-mo RR 0.82 |
| Wang 2024 (PMID 38795099) | Real-world TriNetX cohort | AF ablation 2014-2023 | No pre-ablation GLP-1 RA | Reduced recurrence, propensity-matched n=6,031 |
The relative risk reductions cluster in a narrow band: roughly 17 to 22 percent in general-obesity randomized populations, 46 percent in HFpEF-enriched populations, and 15 to 22 percent in real-world post-ablation cohorts. The direction is uniform across designs and across single, dual, and triple incretin classes.
Mechanism: why GLP-1 RAs may calm the atria
The mechanism literature has converged on several plausible pathways, none individually proven as the dominant driver but all biologically consistent with a class-level AF benefit.
Weight loss and reduced atrial volume. The strongest mechanism is the most obvious one. Obesity drives left atrial enlargement and atrial myopathy. Sustained 10 percent or greater weight loss reduces left atrial volume and slows or reverses atrial remodeling. The Karakasis subgroup analysis found no effect modification by weight-loss magnitude, which means weight loss is necessary but the threshold for benefit is not extreme. The HFpEF meta-analysis specifically reported greater left atrial volume reduction on drug.
Epicardial adipose tissue reduction. Epicardial fat, which wraps directly around the atria, is metabolically active and pro-inflammatory. It releases cytokines and bioactive lipids that locally infiltrate atrial tissue and promote fibrosis and electrical heterogeneity. GLP-1 RAs reduce epicardial fat volume in imaging studies, and several mechanism reviews (Front Pharmacol / PMC12999421) position epicardial fat reduction as a leading candidate for the structural piece of the AF benefit.
Blood pressure reduction. GLP-1 RAs lower systolic blood pressure by 3 to 6 mmHg in the obesity trials. Hypertension is a major AF risk factor. Even modest BP reductions sustained over years modify AF substrate.
Glycemic and inflammatory effects. Hyperglycemia and chronic low-grade inflammation both promote atrial fibrosis. GLP-1 RAs reduce HbA1c (in diabetic populations), reduce CRP, and modulate several inflammatory cytokines relevant to atrial remodeling.
Autonomic effects. GLP-1 receptors are expressed on cardiomyocytes and on the vagal and sympathetic afferents that modulate atrial electrophysiology. Class-wide observations of a small resting heart-rate increase suggest measurable autonomic effects. Whether this is net pro-arrhythmic, neutral, or part of the rhythm story is unresolved.
A 2026 review framing the integrated mechanism map argues that GLP-1 RAs are best understood as substrate-modifying agents rather than direct ion-channel anti-arrhythmics (SGLT2 inhibitors and GLP-1 receptor agonists in atrial fibrillation treatment). That framing matches the trial data: the AF benefit emerges over months and tracks weight, blood pressure, and structural cardiac changes, not the kinetics of an acute pharmacologic effect.
What the data do not show
Restraint matters here. The signal is consistent, but the gaps are real.
The trials were not designed with AF as a primary endpoint. SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM were powered for cardiovascular MACE, kidney outcomes, or KCCQ-CSS symptom scores. AF was ascertained as a secondary or adjudicated event. That introduces ascertainment bias risk in both directions and means absolute event rates are modest in the obesity trials.
There is no randomized trial with continuous AF burden monitoring as the primary outcome. The ablation cohorts use chart-review or coding-based recurrence definitions, which under-detect asymptomatic AF. The Apple Watch and ILR-monitoring era of AF burden trials has not yet completed a GLP-1 study.
No GLP-1 RA carries a regulatory indication for AF prevention, rhythm control, or post-ablation recurrence reduction in mid-2026. The American Heart Association and European Society of Cardiology guidelines do not recommend GLP-1 RAs as AF-directed therapy. The case for considering them in eligible patients (overweight or obese, with AF history, and an independent metabolic or cardiovascular indication for GLP-1 RA therapy) rests on extrapolation from the trial data rather than on direct guideline support.
The magnitude of any drug-specific signal above weight loss is unresolved. Some signal-detection work suggests semaglutide may track lower AF rates than liraglutide or dulaglutide in observational comparisons, but the Karakasis subgroup analyses do not support a strong class differentiation. Until a head-to-head randomized trial directly compares GLP-1 RAs against weight-loss-matched comparators, the weight-loss-mediated versus drug-specific question stays open.
Tirzepatide and the dual or triple agonists have less standalone AF data than semaglutide. The SURMOUNT cardiovascular outcomes trial (covered separately as SURPASS-CVOT for the type 2 diabetes population) is still accumulating. Retatrutide TRIUMPH-CVOT is not expected until 2028. For retatrutide, the rhythm data are extrapolated from Phase 2 safety signals and class-level reasoning, not from dedicated rhythm-endpoint analyses.
The rare case reports of new-onset AF temporally associated with tirzepatide initiation (PMID 41425685) do not change the population-level risk-benefit math, but they are a reminder that individual patient outcomes can diverge from population effect estimates. A baseline ECG and routine pulse assessment remain sensible practice when initiating any GLP-1 RA in patients with prior cardiac history.
Practical implications
For an obese patient with paroxysmal AF and an independent metabolic indication for semaglutide or tirzepatide, the AF data are now consistent enough that the cardiac history is not a reason to avoid initiation. In most cases, especially with sustained weight loss above 10 percent, the AF substrate likely improves.
For a patient who has undergone catheter ablation, the post-ablation cohorts and 2026 meta-analysis support GLP-1 RA exposure as one of the modifiable factors that tracks lower recurrence. This still falls under cardiology and metabolic team discussion, not patient-initiated protocol.
For a patient on a GLP-1 RA who develops new AF, the case reports do not establish causation, and the population-level data argue against discontinuation on AF grounds alone. Standard AF workup and rhythm or rate management should follow guideline care.
For a patient using GLP-1 RAs outside FDA-approved indications (which is common in research and biohacking contexts), the AF data should not be over-interpreted as a license to use these agents as rhythm drugs. They are not rhythm drugs. They are metabolic drugs with a downstream rhythm benefit that emerges from sustained weight loss and substrate modification.
The compound-class comparison is shifting fast. The GLP-1 dosing comparison table and the GLP-1 amylin combination pipeline cover the current state of the available agents and the next-wave combinations that will read out across 2026-2027. The reconstitution calculator handles vial-to-dose math for the injectable end.
Sourcing for researchers
If you are running protocols that involve semaglutide, tirzepatide, or retatrutide and want to verify lot-level purity, the injectable side of this class is best sourced through vendors that publish certificates of analysis. Ascension Peptides covers research vials in this class with code ENHANCED for 50% off. For the oral end (orforglipron, oral semaglutide research analogs), Limitless Biotech covers that format with code ENHANCED. Neither sourcing channel replaces a clinician-led cardiovascular workup, and AF is not a research-vial protocol indication. Use these vendors for the metabolic and obesity research where they belong, and pursue rhythm care through a cardiologist or electrophysiologist.
This article is for educational and research purposes only and is not medical advice. No GLP-1 receptor agonist carries an FDA-approved indication for atrial fibrillation prevention, rhythm control, or post-ablation recurrence reduction as of mid-2026. The data summarized above derive from secondary-endpoint analyses of obesity and cardiovascular outcomes trials, from post-ablation observational cohorts subject to residual confounding, and from one HFpEF-enriched meta-analysis. Atrial fibrillation is a serious arrhythmia that carries stroke, heart failure, and mortality risk. Diagnosis, anticoagulation decisions, rhythm or rate control selection, and ablation timing must be individualized by a cardiologist or electrophysiologist working from the patient's full clinical picture. Do not start, switch, or stop any therapy on the basis of this article. Consult a qualified clinician before acting on any information here.


