At a glance
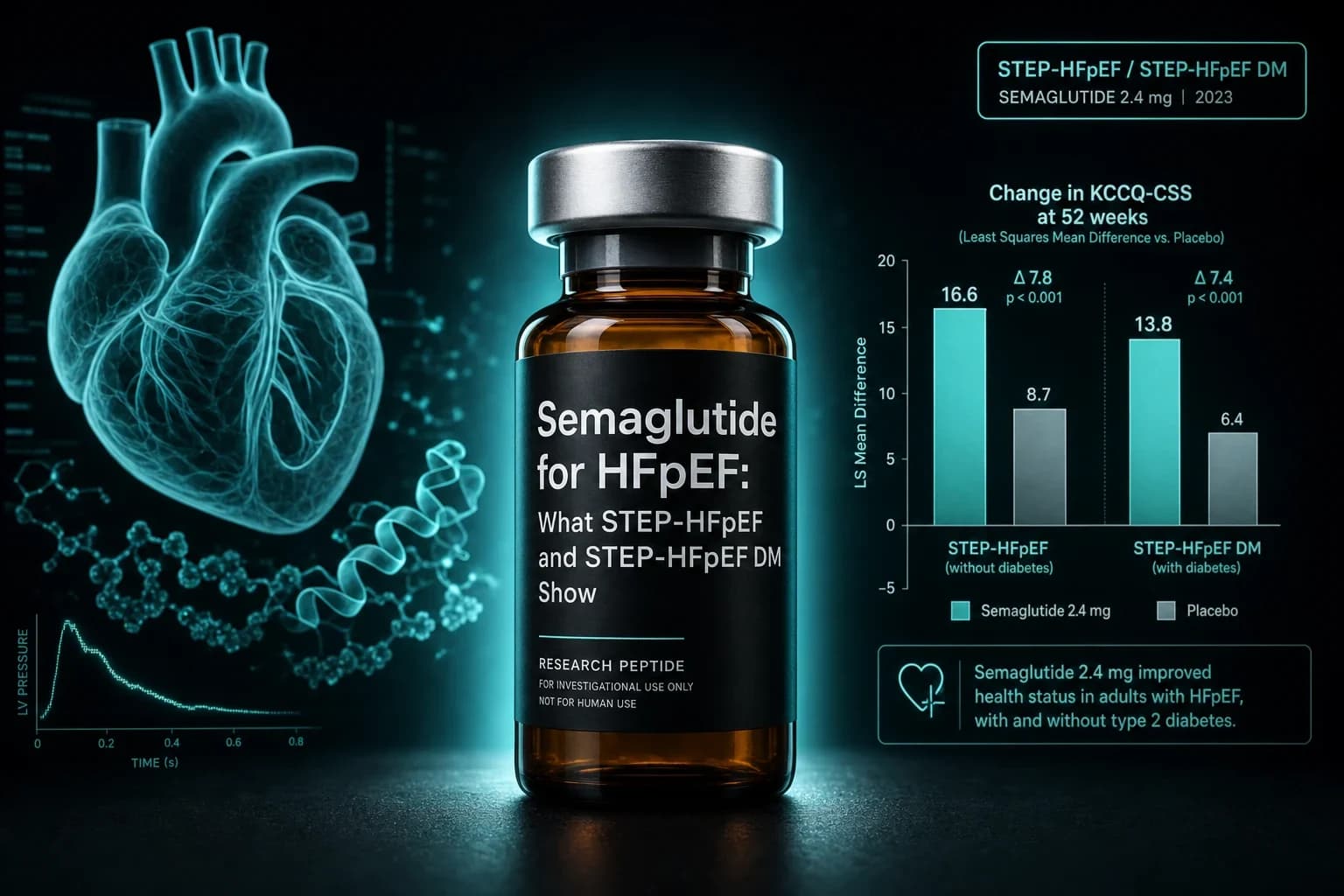
- STEP-HFpEF (n=529, no diabetes, 52 weeks): KCCQ-CSS improved 16.6 vs 8.7 points, treatment difference 7.8 (95% CI 4.8 to 10.9, P<0.001)
- STEP-HFpEF DM (n=616, with type 2 diabetes, 52 weeks): KCCQ-CSS 13.7 vs 6.4, treatment difference 7.3 points (95% CI 4.1 to 10.4, P<0.001)
- Pooled SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM (n=3,743 with HF history): HR 0.69 for CV death or worsening HF (95% CI 0.53 to 0.89, P=0.0045)
- Weight reduction was -13.3% vs -2.6% in the no-diabetes trial and -9.8% vs -3.4% in the type 2 diabetes trial
- No Phase 3 hard-outcome trial in HFpEF yet exists. Semaglutide is not approved for heart failure as of June 2026
Why STEP-HFpEF matters
HFpEF used to be the heart failure phenotype with no good drug story. Beta-blockers and ACE inhibitors lifted survival in HFrEF for decades while patients with preserved ejection fraction got watchful waiting and diuretic titration. SGLT2 inhibitors changed that in 2021. STEP-HFpEF and STEP-HFpEF DM changed it again by showing that the obesity-related phenotype responds to GLP-1 receptor agonism at a magnitude no HFpEF drug had ever produced on patient-reported outcomes.
That is the framing readers searching for "semaglutide HFpEF" usually want and rarely get. The drug did not heal hearts. It treated obesity-driven heart failure by treating the obesity, and that path produced symptom and exercise gains that look unlike anything else in the field. The trials are real, the effect sizes are large, the limitations are specific, and the hard-outcome data are still pending. This article walks through each trial in turn.
Bottom line: STEP-HFpEF and STEP-HFpEF DM are Phase 3 randomized trials of semaglutide 2.4 mg in obesity-related HFpEF. Both hit dual primary endpoints on KCCQ-CSS and body weight. A pooled Lancet 2024 analysis suggests fewer cardiovascular death or worsening HF events, though semaglutide is not approved for heart failure.
The obesity HFpEF phenotype
Heart failure with preserved ejection fraction is a clinical syndrome, not a single disease. The obesity-driven phenotype, which the STEP-HFpEF program targeted, has a recognizable signature. BMI is high, often 35 to 40. Pericardial restraint and visceral adiposity raise filling pressures. Inflammation, measured by hsCRP, is elevated. Exercise tolerance is poor, and the limit is often hemodynamic rather than ischemic. Diuretic dependence is common. KCCQ-CSS scores cluster low.
The hypothesis behind STEP-HFpEF was that weight loss in this group would unload the heart mechanically, reduce systemic inflammation, and translate to symptom and function gains. That hypothesis is what the trials tested. They did not test whether semaglutide repairs cardiac muscle, restores diastolic relaxation independent of weight, or alters HFpEF biology in lean patients. Those are separate questions, and the answers are not in.
STEP-HFpEF (no diabetes): Kosiborod NEJM 2023
STEP-HFpEF randomized 529 adults across 96 sites in 13 countries to once-weekly semaglutide 2.4 mg or placebo for 52 weeks (Kosiborod et al., NEJM 2023, PMID 37622681). Entry criteria required NYHA II to IV symptoms, LVEF 45% or higher, BMI 30 or higher, KCCQ-CSS below 90, and 6-minute walk distance of 100 meters or more. Patients with type 2 diabetes were excluded; that population had its own trial.
The dual primary endpoints were change in KCCQ-CSS and percentage change in body weight at week 52. Confirmatory secondary endpoints included 6-minute walk distance, hsCRP, and a hierarchical composite combining death, HF events, KCCQ-CSS change, and 6-minute walk change.
What the primary endpoints showed
| Endpoint at 52 weeks | Semaglutide 2.4 mg | Placebo | Estimated treatment difference |
|---|---|---|---|
| KCCQ-CSS change | +16.6 points | +8.7 points | +7.8 points (95% CI 4.8 to 10.9, P<0.001) |
| Body weight change | -13.3% | -2.6% | -10.7 percentage points (95% CI -11.9 to -9.4, P<0.001) |
| 6-minute walk distance | +21.5 m | +1.2 m | +20.3 m (95% CI 8.6 to 32.1, P<0.001) |
| hsCRP ratio (week 52 / baseline) | 0.57 | 0.92 | Ratio 0.61 (95% CI 0.51 to 0.72, P<0.001) |
The KCCQ-CSS gain is the number to anchor on. A 7.8-point treatment difference exceeds the 5-point threshold typically called clinically important in heart failure trials. Both SGLT2 inhibitor HFpEF trials, EMPEROR-Preserved and DELIVER, produced low single-digit KCCQ-CSS treatment differences in the same patient-reported endpoint. Spironolactone in TOPCAT produced no significant KCCQ improvement. The semaglutide effect on symptoms is the largest reported for any pharmacotherapy in HFpEF.
Adverse events
Serious adverse events were 13.3% on semaglutide versus 26.7% on placebo, driven by fewer HF-related events in the active arm. Gastrointestinal disorders were more common on semaglutide as expected. There was no excess of acute kidney injury, no excess of pancreatitis, and no signal for unexpected harm. The benefit-to-risk in this 52-week window favored semaglutide.
STEP-HFpEF DM: Kosiborod NEJM 2024
STEP-HFpEF DM ran the same design in the population the first trial excluded: 616 adults with obesity, HFpEF, and type 2 diabetes, randomized to semaglutide 2.4 mg or placebo for 52 weeks (Kosiborod et al., NEJM 2024, PMID 38587233). The hypothesis was that the symptom and function gains would carry over despite the well-known blunting effect of type 2 diabetes on GLP-1 weight loss.
They did.
What the primary endpoints showed
| Endpoint at 52 weeks | Semaglutide 2.4 mg | Placebo | Estimated treatment difference |
|---|---|---|---|
| KCCQ-CSS change | +13.7 points | +6.4 points | +7.3 points (95% CI 4.1 to 10.4, P<0.001) |
| Body weight change | -9.8% | -3.4% | -6.4 percentage points (95% CI -7.6 to -5.2, P<0.001) |
| 6-minute walk distance | Significant gain vs placebo | (smaller than no-DM trial) | Confirmatory secondary positive |
| NT-proBNP | Reduction vs placebo | (smaller than no-DM trial) | Confirmatory secondary positive |
Two contrasts with STEP-HFpEF are worth naming directly. Weight loss was smaller (-9.8% vs -13.3%), as expected when type 2 diabetes coexists. The KCCQ-CSS treatment difference held at 7.3 points, almost identical to the 7.8 points in the no-diabetes trial. That uncoupling of weight from symptom benefit, which became one of the program's most-discussed findings, suggested mechanisms beyond pure mechanical unloading.
Subgroup signal: HbA1c does not predict benefit
A prespecified analysis stratified STEP-HFpEF DM by baseline HbA1c (Verma et al., Lancet Diabetes Endocrinol 2025, PMID 39848268). The KCCQ-CSS treatment difference was consistent across baseline glycemic burden. Symptom benefit did not require glycemic improvement. That finding rules out one mechanistic alternative and tightens the case that semaglutide's HFpEF effect tracks more closely with weight loss, inflammation reduction, and possibly direct GLP-1 receptor signaling than with HbA1c change.
Note: The KCCQ-CSS gains in STEP-HFpEF (7.8 points) and STEP-HFpEF DM (7.3 points) are the largest reported for any pharmacotherapy in obesity-related HFpEF. The trials were powered for symptom and weight, not mortality, and neither was designed to detect a hospitalization signal at 52 weeks.
Pooled hard-outcome analysis: Petrie Lancet 2024
KCCQ scores answer the symptom question. They do not answer the hospitalization or survival question. To address that, the investigators pooled participant-level data across four semaglutide trials with prespecified heart failure endpoints: SELECT (cardiovascular outcomes in obesity, no diabetes), FLOW (kidney outcomes in type 2 diabetes), STEP-HFpEF, and STEP-HFpEF DM (Petrie et al., Lancet 2024, PMID 39222642). The combined sample with a history of HFpEF or HFmrEF was 3,743.
The results, summarized:
| Endpoint | Semaglutide | Placebo | Hazard ratio |
|---|---|---|---|
| CV death or worsening HF event | 5.4% (103/1914) | 7.5% (138/1829) | 0.69 (95% CI 0.53 to 0.89, P=0.0045) |
| Worsening HF event alone | 2.8% (54/1914) | 4.7% (86/1829) | 0.59 (95% CI 0.41 to 0.82, P=0.0019) |
| Cardiovascular death alone | 3.1% (59/1914) | 3.7% (67/1829) | 0.82 (95% CI 0.57 to 1.16, P=0.25) |
That is the strongest hard-outcome signal semaglutide has generated in HFpEF. Read carefully: the pooled analysis is not a single Phase 3 outcome trial. Three of the four contributing studies had primary endpoints elsewhere. The combined HFpEF cohort is heterogeneous. Worsening HF events include both hospitalization and urgent ambulatory visits with intravenous diuretic. The cardiovascular death signal alone is not significant. None of that makes the 0.69 hazard ratio for the composite endpoint go away, but it does mean the signal is hypothesis-strengthening rather than confirmatory.
A dedicated HFpEF outcomes trial would settle the question. As of June 2026, no such trial has reported.
Semaglutide vs tirzepatide in HFpEF
Readers comparing options usually want the head-to-head, which does not exist. SUMMIT randomized tirzepatide in obesity-related HFpEF and produced concordant symptom and weight effects, covered in detail in the tirzepatide SUMMIT trial breakdown. Cross-trial comparison is not a substitute for a head-to-head, but the magnitudes are roughly comparable on KCCQ-CSS, with tirzepatide producing larger weight loss in line with its non-HFpEF benchmarks.
| Trial | Drug | Population | KCCQ-CSS treatment difference | Weight loss treatment difference |
|---|---|---|---|---|
| STEP-HFpEF (n=529) | Semaglutide 2.4 mg | Obesity HFpEF, no T2D | +7.8 pts | -10.7 percentage points |
| STEP-HFpEF DM (n=616) | Semaglutide 2.4 mg | Obesity HFpEF + T2D | +7.3 pts | -6.4 percentage points |
| SUMMIT (n=731) | Tirzepatide 5/10/15 mg | Obesity HFpEF (mixed T2D status) | +6.9 pts | -11.6 percentage points |
The numbers favor neither drug decisively for HFpEF symptoms. Both produced clinically meaningful KCCQ gains. Tirzepatide produced larger weight loss in the SUMMIT-comparable subgroup, consistent with what SURMOUNT-5 showed for obesity broadly. The decision between them in clinical use is not driven by HFpEF data alone, and the choice is not free of comorbidity, tolerance, and access constraints, which is why the GLP-1 dosing comparison is usually the more useful starting point than this trial-by-trial breakdown.
Mechanism: weight loss is part of the story, not all of it
If the STEP-HFpEF benefit were pure mechanical unloading, KCCQ-CSS gains would scale tightly with kilograms lost. They do not. Subgroup analyses across both trials show that the symptom benefit accrued even in patients with smaller weight loss, and the type 2 diabetes cohort gained nearly as many KCCQ points on roughly half the weight loss.
Three mechanisms are plausible:
- Mechanical unloading. Less visceral and pericardial fat reduces filling pressures. This is real and matters.
- Anti-inflammatory effect. hsCRP fell by roughly 40% in STEP-HFpEF. Inflammation is mechanistically linked to HFpEF physiology, and weight-independent CRP reduction may explain part of the uncoupling.
- Direct GLP-1 receptor effect on cardiomyocytes and vascular tissue. Preclinical work supports GLP-1 receptor signaling in the heart, but the human relevance is uncertain.
These are not mutually exclusive, and the trials were not designed to apportion contributions. What the data do support is that "semaglutide treats HFpEF by causing weight loss" is too narrow. The mechanism almost certainly includes a weight-independent component, and Roche's diuretic-use pooled analysis pushed in the same direction by showing reduced loop diuretic dependence on semaglutide (Shah et al., Eur Heart J 2024, DOI 10.1093/eurheartj/ehae322).
What the trials do not answer
A short list of questions that STEP-HFpEF and STEP-HFpEF DM do not settle:
- Hard outcomes in HFpEF specifically. The pooled Lancet analysis points to a 31% relative reduction in CV death or worsening HF events. That signal needs a dedicated Phase 3 outcomes trial to be confirmatory.
- Lean HFpEF. Both trials required BMI 30 or higher. Whether semaglutide helps HFpEF in non-obese patients is unknown.
- Long-term durability. The 52-week window catches the bulk of weight loss but not the long horizon HF clinicians manage. Open-label extension data and the planned SUMMIT extension will help, but neither is a dedicated outcomes trial.
- Discontinuation effects. Stopping semaglutide typically regains most weight within a year. Whether HFpEF symptoms also recur is plausible and not directly tested.
- HFrEF. Both trials excluded LVEF below 45%. The pooled analysis included HFmrEF patients (LVEF 40 to 49%), but HFrEF is its own story. STEP-HFrEF has not been done.
Warning: Semaglutide is not FDA-approved for heart failure as of June 2026. The label covers type 2 diabetes (Ozempic, Rybelsus), chronic weight management (Wegovy), and cardiovascular outcomes in obesity without diabetes via the SELECT extension. HFpEF use is off-label and is a clinical decision, not a research-purposes-only practice.
Practical context for the research community
Three points worth naming, since this is where readers usually land after the trial data:
- The STEP-HFpEF KCCQ gain is roughly three times the threshold for "clinically meaningful." Whether that translates to fewer hospitalizations and longer life is the open question, but the symptom-and-function story is unusually strong by HFpEF standards.
- Diabetes status modulates the magnitude but not the direction. STEP-HFpEF DM patients gained nearly as much on KCCQ for roughly half the weight loss, which weakens the simplest "it is all weight loss" explanation.
- The semaglutide-vs-tirzepatide question for HFpEF cannot be settled with cross-trial comparison. SUMMIT and STEP-HFpEF used overlapping but distinct populations and outcomes, and the dose-response curves differ. The relevant cross-comparison for clinicians is the oral vs injectable bioavailability tradeoff and the SOUL oral-semaglutide cardiovascular data if oral is on the table.
If you are reconstituting research-grade semaglutide for protocol use, the reconstitution chart and the reconstitution calculator cover the unit math. Research-grade semaglutide is available from Ascension Peptides with 50% off using code ENHANCED. None of this substitutes for clinical care of heart failure.
What changes if a dedicated HFpEF outcomes trial reports
Two scenarios. If a Phase 3 HFpEF outcomes trial confirms the pooled hazard ratio, semaglutide becomes the first GLP-1 to carry a heart failure indication, alongside SGLT2 inhibitors. If the trial fails to confirm, the symptom and function data still stand, and obesity-related HFpEF becomes a textbook example of a phenotype that responds to weight loss without necessarily responding to weight-loss drugs at the mortality level. Neither outcome would erase the existing 7.8-point KCCQ benefit. The clinical positioning would shift, but the patient-reported part of the story would not.
The relevant trial to watch is the planned semaglutide HFpEF outcomes study, expected to read out by late 2027 or early 2028. Until then, the strongest available evidence is what STEP-HFpEF, STEP-HFpEF DM, and the pooled Lancet analysis already published.
Bottom line: STEP-HFpEF and STEP-HFpEF DM are the largest, most rigorous RCTs of any drug class in obesity-related HFpEF. The symptom and function benefits are large and replicated. The hard-outcome signal is suggestive but not confirmatory. Semaglutide is not a heart failure drug by label, and treating HFpEF with semaglutide is a clinical decision that the trials inform but do not finalize.
This article is for research and educational purposes only. It is not medical advice. Heart failure is a serious condition that requires evaluation and care from a licensed clinician. Discuss any decision involving semaglutide or other GLP-1 receptor agonists with a qualified physician.


