At a glance
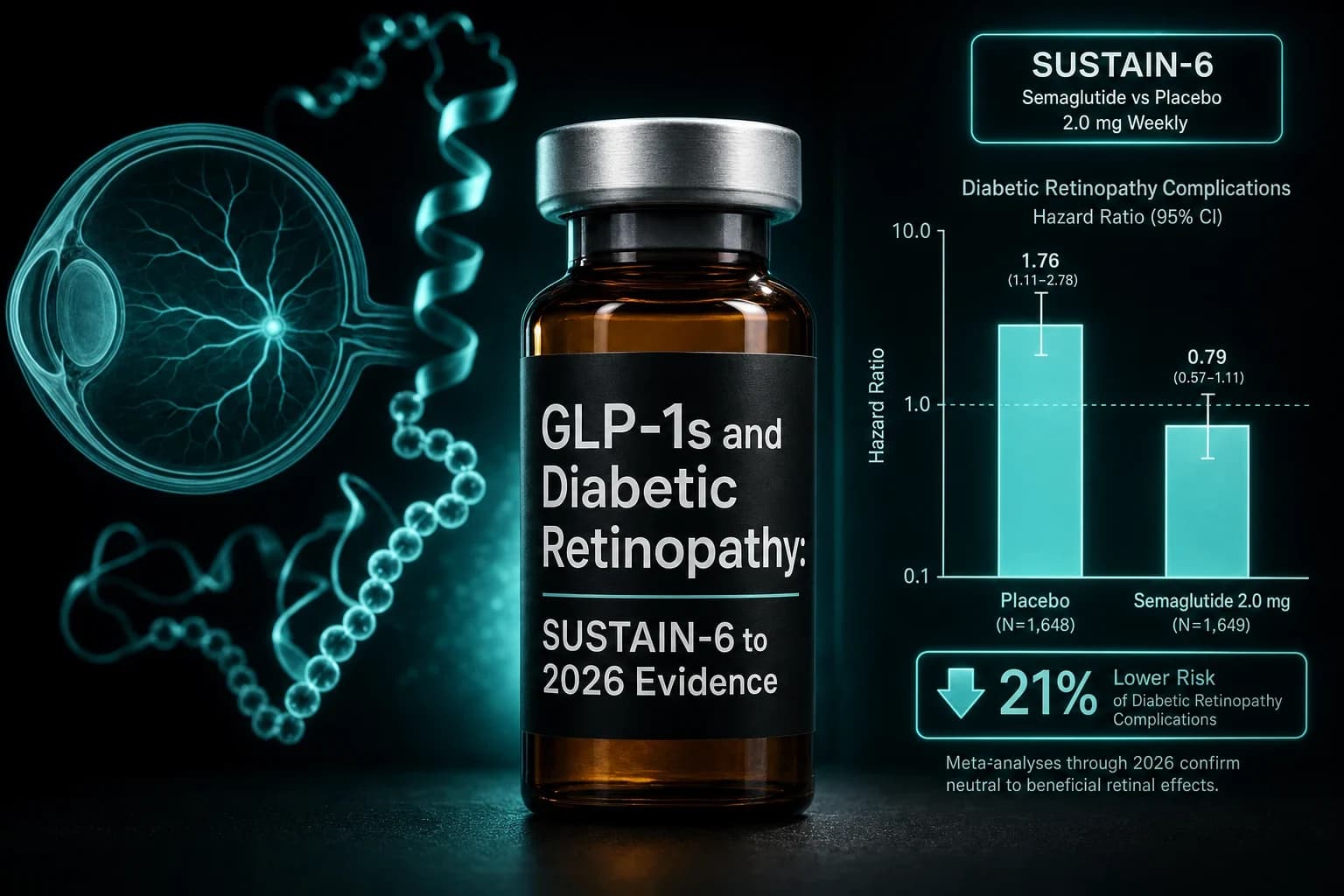
- SUSTAIN-6 (Marso 2016, PMID 27633186) showed semaglutide carried a retinopathy-complication hazard ratio of 1.76 (3.0% vs 1.8%) over 2 years.
- Vilsbøll 2018 (PMID 29178519) tied most of that signal to the speed of HbA1c drop in patients with prior retinopathy on insulin, not the drug itself.
- The 800,390-user OHDSI cohort (Cai 2025, PMID 41192935) found no increase in proliferative DR or treatment-requiring DR/DME versus other GLP-1s or non-GLP-1s.
- Tirzepatide cut diabetic-retinopathy diagnoses across 173,846 matched patients in a 2026 Ophthalmology cohort (Yeh, PMID 41577258).
- Buckley 2025 Diabetologia found tirzepatide doubled new-onset PDR (1.1% vs 0.5%) yet lowered any-new retinopathy in DR-free patients.
The SUSTAIN-6 trial finished its readout in 2016 and handed diabetes endocrinologists a number they still cannot ignore: semaglutide users had a 76 percent higher risk of retinopathy complications than placebo users over two years. That single hazard ratio shaped the warning that now ships on every box of Ozempic, Rybelsus, and Wegovy, and it shaped the bigger question the field has been arguing about ever since. Is the eye signal caused by the drug, or by the speed at which the drug fixes long-standing high blood sugar?
A decade of follow-up studies, including the 800,390-user OHDSI network analysis published in 2025 and the first dedicated tirzepatide cohorts in 2025 and 2026, point in a clear direction. The signal is real, the mechanism is glycemic correction more than the molecule, and the absolute risk depends almost entirely on what the retina looked like before the first injection.
Bottom line: Most of the SUSTAIN-6 retinopathy signal traces to rapid HbA1c reduction in patients with pre-existing diabetic retinopathy on insulin. Large population data find no broad increase in proliferative DR or treatment-requiring DR/DME for semaglutide, and tirzepatide cohorts now show a net reduction in DR diagnoses. The exception is patients with moderate or worse non-proliferative DR at baseline, where titration should be slower and an eye exam should come first.
What SUSTAIN-6 actually measured
SUSTAIN-6 was a two-year cardiovascular outcomes trial of subcutaneous semaglutide 0.5 mg or 1.0 mg weekly versus placebo in 3,297 adults with type 2 diabetes and high cardiovascular risk (Marso et al., NEJM 2016, PMID 27633186). The primary endpoint was a composite of cardiovascular death, non-fatal MI, and non-fatal stroke. Semaglutide met its non-inferiority test and crossed the line for superiority, which is the result that mattered for the label.
The retinopathy finding was a pre-specified secondary safety endpoint, not the primary outcome. Retinopathy complications were defined narrowly: vitreous haemorrhage, blindness, or any condition treated with intravitreal agents or photocoagulation. Those events happened in 50 patients (3.0 percent) on semaglutide and 29 patients (1.8 percent) on placebo. The hazard ratio was 1.76 (95% CI 1.11 to 2.78, P = 0.02). Routine retinopathy, which is the broader umbrella that includes microaneurysms and background changes, was not statistically different between groups.
Two design facts shape how to read this. SUSTAIN-6 enrolled a cardiovascular-risk-enriched population, which means more long-standing diabetes, more existing microvascular disease, and more insulin use than a general T2D clinic would see. Baseline HbA1c was 8.7 percent, which is high. And the drop in HbA1c during the first 16 weeks was the largest in the trial. The Vilsbøll 2018 subgroup analysis (PMID 29178519) reported that excess retinopathy risk concentrated in patients who already had retinopathy at baseline, were on insulin, and saw the steepest HbA1c reductions over those first four months. In patients with no baseline retinopathy, the signal disappeared.
The mechanism is glycemic correction, not the drug
The same pattern shows up in non-GLP-1 data and has shown up for thirty years. The Diabetes Control and Complications Trial randomised 1,441 adults with type 1 diabetes to intensive or conventional glycemic control. Early worsening of retinopathy at the six- or twelve-month visit occurred in 13.1 percent of intensive-treatment patients versus 7.6 percent on conventional control (DCCT, Ophthalmology 1998, PMID 9682700). The strongest predictors of early worsening were a higher baseline HbA1c and a steeper drop in the first six months. By eighteen months, the worsening had reversed in nearly every case, and the same intensive-control arm went on to a 76 percent reduction in long-term retinopathy incidence.
That is the framing that matters for any GLP-1 user with diabetes. Rapid glycemic correction transiently destabilises retinal microvasculature in eyes that already had ischemic or proliferative changes. The damage is most likely in the first six to twelve months and is usually reversed if the macular and retinal status is monitored. Insulin, pancreas transplant, bariatric surgery, and now potent GLP-1 receptor agonists all produce the same short-term effect because they all produce the same outcome: a fast HbA1c drop.
Note: Early worsening is not the same as a permanently higher risk of blindness. The DCCT showed that even patients with measurable early worsening went on to dramatically lower long-term retinopathy progression versus conventional control. The risk is a titration window, not a verdict.
The large 2024 to 2026 cohort data on semaglutide
After SUSTAIN-6, the field needed to know whether the signal held outside the trial population. The largest analysis to date was an OHDSI network study covering 14 databases and 800,390 new semaglutide users with type 2 diabetes from December 2017 through December 2023 (Cai et al., BMJ Open Diabetes Research & Care 2025, PMID 41192935). Across every meaningful comparison, semaglutide users showed no increased risk of proliferative DR or treatment-requiring DR/DME versus other GLP-1 agonists or non-GLP-1 second-line diabetes drugs. A few comparisons actually trended toward reduced PDR (versus glipizide) and reduced treatment-requiring DR/DME (versus dulaglutide and sitagliptin), consistent with the long-term retinopathy benefit you would expect from better glucose control.
FAERS pharmacovigilance data have produced more mixed signals, which is what FAERS is built to do. A 2024 disproportionality analysis examined ocular adverse events across GLP-1 agonists in the FDA Adverse Event Reporting System and reported elevated reporting odds ratios for several ophthalmic events including diabetic retinopathy, blurred vision, and visual impairment (Bouayed et al., 2024, PMID 39425661). The honest read on FAERS is that it can flag a signal worth investigating but cannot generate incidence rates or causal estimates. It catches reports, not denominators.
The review literature has tracked the same evolution. A 2022 perspective in Eye London surveyed the SUSTAIN program and concluded that the most parsimonious explanation for the retinopathy signal was the magnitude and speed of HbA1c reduction in a higher-risk subgroup, not a direct retinal toxicity (Sharma et al., Eye London 2022, PMID 34373613). A more recent ophthalmology-focused review of the broader class flagged the same point alongside the NAION question, which is a separate optic neuropathy covered in the semaglutide and NAION evidence article (Tjernström et al., 2025, PMID 39883468).
Tirzepatide is not a smaller version of semaglutide
The first dedicated tirzepatide retinopathy cohorts arrived in 2025 and 2026, and they did not replicate the SUSTAIN-6 pattern. The biggest is a TriNetX multicenter U.S. cohort of 173,846 propensity-score-matched adults with type 2 diabetes (Yeh et al., Ophthalmology 2026, PMID 41577258). Tirzepatide use was associated with fewer diabetic-retinopathy diagnoses, fewer DR-related complications, and fewer ophthalmic interventions than lifestyle intervention alone over the analysed window.
That headline result hides a more interesting nuance. A separate Diabetologia real-world cohort matched 3,435 tirzepatide-exposed adults with 3,434 unexposed controls for sex, diabetes duration, baseline retinopathy status, HbA1c, screening frequency, and other glucose-lowering medications (Buckley et al., Diabetologia 2025, DOI 10.1007/s00125-025-06466-8). New-onset proliferative diabetic retinopathy occurred in 1.1 percent of tirzepatide-exposed versus 0.5 percent of unexposed patients, and tirzepatide was significantly associated with new-onset PDR in multivariate analysis. Yet in the subgroup with no retinopathy at initiation, tirzepatide was associated with reduced odds of any new retinopathy.
The result is the SUSTAIN-6 pattern restated. Patients with no baseline retinopathy do better. Patients with baseline retinopathy carry a higher short-term risk of progression to a sight-threatening stage, especially when their glycemic correction is steep. The dual GIP/GLP-1 mechanism does not appear to change the rule.
What the evidence base actually says, in one table
| Study | Design | N | Comparator | Retinopathy effect | What it means |
|---|---|---|---|---|---|
| Marso 2016 (SUSTAIN-6) | RCT, 2 years | 3,297 | Placebo | HR 1.76 (1.11 to 2.78) for retinopathy complications | Originating signal; high-risk T2D, insulin users, prior DR |
| Vilsbøll 2018 (subgroup) | Pre-specified subgroup of SUSTAIN-6 | 3,297 | Placebo | Excess risk concentrated in those with prior DR, insulin use, steepest HbA1c drop in first 16 weeks | Mechanism is glycemic correction, not direct retinal toxicity |
| DCCT 1998 | RCT, 6.5 years (T1D) | 1,441 | Conventional control | Early worsening 13.1% vs 7.6%; reversed by 18 months; long-term DR cut 76% | Class effect of fast glucose lowering; window is short |
| Cai 2025 (OHDSI) | Multi-database cohort | 800,390 new semaglutide users | Other GLP-1s, SGLT-2 inh, DPP-4, glipizide | No increase in PDR or treatment-requiring DR/DME | Largest population signal: net flat to favorable |
| Yeh 2026 (TriNetX) | Multicenter cohort | 173,846 matched | Lifestyle only | Fewer DR diagnoses, complications, ophthalmic interventions | Tirzepatide-favorable at population scale |
| Buckley 2025 | Matched real-world cohort | 6,869 | Tirzepatide-unexposed | New-onset PDR 1.1% vs 0.5%; lower new DR in DR-free patients | Same pattern as SUSTAIN-6: baseline DR matters |
Who actually needs an eye exam before starting
The decision is not whether to start a GLP-1 receptor agonist. It is whether to start it before or after a dilated eye exam, and how aggressively to titrate. The risk stratification below tracks the evidence base.
| Baseline status | Eye exam before start? | Titration approach | What to watch |
|---|---|---|---|
| No diabetes (obesity indication) | Not required | Standard | NAION and routine yearly exam |
| T2D, no known retinopathy, HbA1c under 8.0% | Recommended within 12 months | Standard | Routine 12-month dilated exam |
| T2D, no known retinopathy, HbA1c above 9.0% | Yes, before titration past 0.5 mg | Slow titration | 3- to 6-month dilated exam during first year |
| Mild non-proliferative DR | Yes, before start | Slow titration | 3- to 6-month exam, sooner if visual symptoms |
| Moderate or severe non-proliferative DR | Yes, treat or stabilise first | Discuss with ophthalmology before starting | 3-month exam during first year |
| Proliferative DR, untreated | Treat first, then start | Hold until retina is stabilised | Pre- and post-treatment retinal imaging |
This is the same monitoring schedule the American Diabetes Association already recommends for any patient on an insulin-equivalent rapid glucose-lowering regimen. The GLP-1 receptor agonist class fits the rule it did not create.
Tip: If you are starting a GLP-1 for type 2 diabetes and your last dilated retinal exam was more than 12 months ago, book one before titrating past the starting dose. The cost is one appointment. The downside of skipping it is a small but real probability of catching early worsening only after symptoms appear.
How to read the FOCUS trial when it lands
FOCUS is the only dedicated, randomised ophthalmic trial for semaglutide in diabetes. It enrolled approximately 1,500 patients with type 2 diabetes and a baseline HbA1c between 7 and 10 percent, randomised them to subcutaneous semaglutide 1.0 mg weekly or placebo, and is following them for five years with standardised retinal imaging. Trial completion is targeted for early 2027.
What FOCUS can tell us is whether semaglutide changes the trajectory of retinopathy independent of the HbA1c-correction effect. If the trial confirms that the signal disappears once you adjust for baseline retinopathy and the magnitude of HbA1c reduction, the field will land where it already appears to be heading: rapid glycemic correction is the relevant variable, the GLP-1 receptor agonist is the vehicle, and the titration window is the place to monitor. If FOCUS finds a residual drug-specific signal even after adjustment, the eye-exam recommendation above tightens further.
Where semaglutide and tirzepatide differ in practice
Across the published cohorts, the pattern is consistent enough to summarise.
- Both drugs produce the same early-worsening risk window in patients with pre-existing retinopathy, especially those undergoing a steep HbA1c reduction in the first 6 months.
- Both drugs produce net-favorable long-term retinopathy outcomes in patients without baseline retinopathy or with mild background changes.
- Tirzepatide has, in two independent 2025 to 2026 cohorts, a more favorable diabetic-retinopathy profile at population scale than semaglutide, plausibly because the dual GIP/GLP-1 mechanism produces a larger glycemic effect per unit of insulin sparing in the early titration phase.
- Both drugs are separate from the NAION question, which involves the optic nerve rather than the retina and is covered in the semaglutide and NAION evidence guide.
If a patient is choosing between the two for type 2 diabetes and has moderate non-proliferative DR at baseline, the retinopathy evidence currently favors tirzepatide, but neither should be started without an eye exam.
How this changes practical decisions
For the obesity indication, in adults without diabetes, the diabetic-retinopathy literature does not apply. Type 2 diabetes is where the entire signal lives, because the underlying disease is what damages the retina. Semaglutide for obesity in non-diabetic patients carries a different risk profile, mostly centered on NAION and the routine GI tolerability questions covered in the STEP and SURMOUNT comparison and the GLP-1 side-effect overviews.
In type 2 diabetes patients with the kind of baseline characteristics SUSTAIN-6 enrolled (HbA1c 8 to 10 percent, longstanding diabetes, insulin use, prior microvascular disease) the recommendation is unchanged from the standard of care: dilated eye exam before titrating past the starting dose, repeat exams at three to six months during the first year, and a slower titration if baseline retinopathy is present. The trial data does not tell anyone to avoid the drug. It tells them to look at the retina first.
Patients on or considering compounded semaglutide or compounded tirzepatide, the retinopathy stratification logic is the same. The drug is the same molecule. The titration schedule is what differs in practice, because compounded protocols sometimes escalate faster than the brand-name label. A faster escalation in someone with baseline DR is exactly the configuration the trial data warns about. Injectable semaglutide and tirzepatide reference vials are available from Ascension Peptides with code ENHANCED for 50% off, and the dosing math for slow titration is laid out in the tirzepatide reconstitution guide and the reconstitution calculator.
Bottom line for readers
The SUSTAIN-6 retinopathy signal is real and was correctly placed on the semaglutide label. The mechanism is overwhelmingly the speed of HbA1c reduction in patients with pre-existing retinopathy, not the drug class. The largest population cohorts to date find no excess risk of proliferative or treatment-requiring DR in unselected semaglutide users, and tirzepatide cohorts trend favorably at population scale. The published nuance, repeated across SUSTAIN-6, the DCCT, and Buckley 2025, is that patients with moderate or worse baseline retinopathy carry a real short-term progression risk that is best managed with a dilated eye exam before titration and a slower escalation in the first six months. Everything else in this article is a footnote on that single decision.
This article is for research and educational purposes only and is not medical advice. Diabetic retinopathy is a serious, potentially sight-threatening complication of diabetes that requires evaluation and management by a qualified ophthalmologist or retina specialist. The studies cited are real and published; the evidence base on GLP-1 receptor agonists and diabetic retinopathy continues to evolve, and the FOCUS trial will provide the first randomised, ophthalmology-endpoint data when it completes. Do not start, switch, or stop semaglutide, tirzepatide, or any glucose-lowering therapy on the basis of this article. Anyone with type 2 diabetes, pre-existing retinopathy, recent vision change, sudden loss of vision in one eye, or scheduled GLP-1 receptor agonist titration should consult their prescribing clinician and a qualified eye-care professional about individualised eye-exam timing and titration pace before acting on any information here.