At a glance
- FDA removed tirzepatide from official shortage list in late 2024; compounded tirzepatide legal access under 503A has been constrained since then
- 503A compounders may still produce tirzepatide for individual patient prescriptions where commercial product is clinically inappropriate (allergies, dose customization)
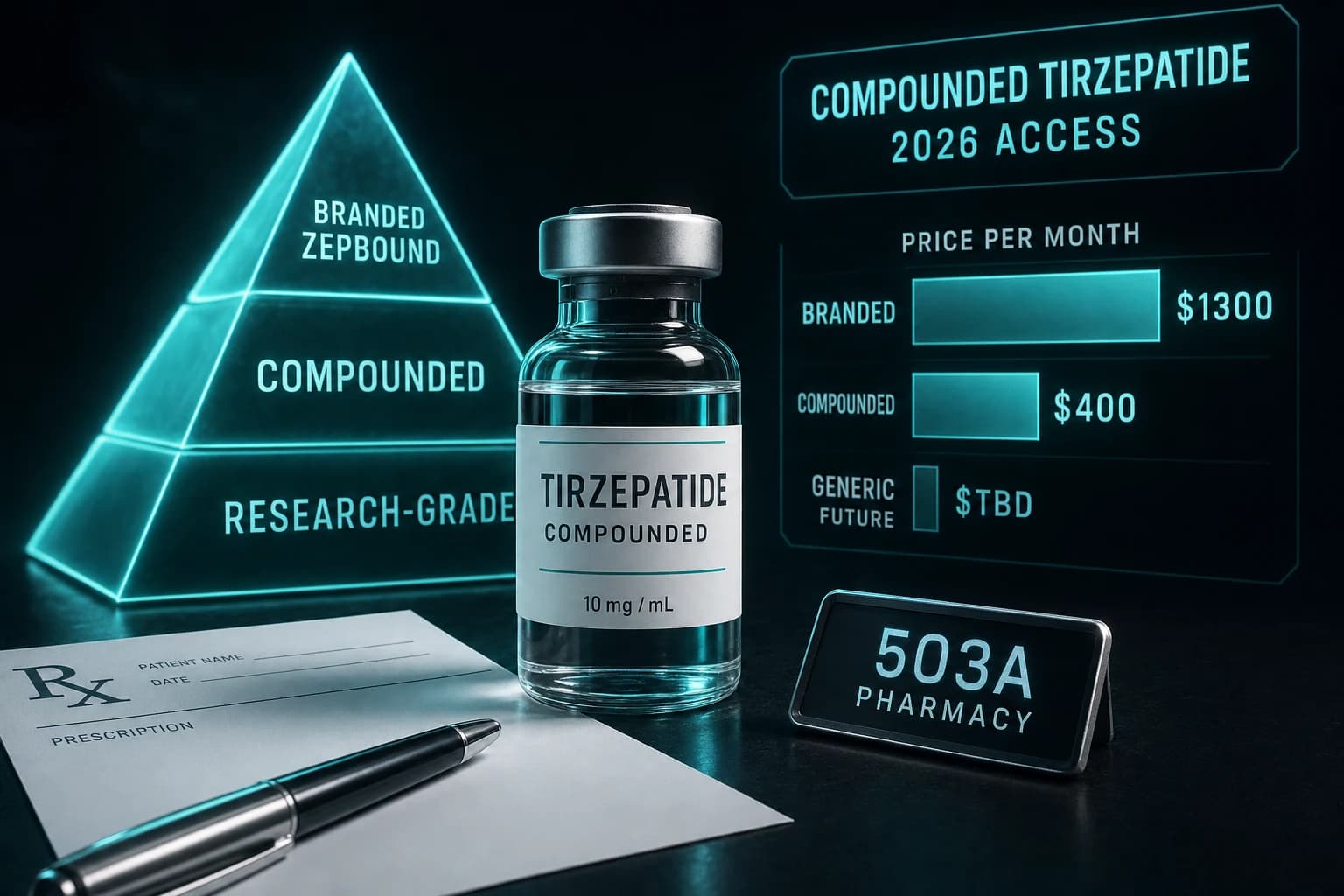
- Compounded tirzepatide pricing typically runs $300-$500/month versus $1,000-$1,400 for branded Zepbound (cash pay), or $500-$650 with manufacturer coupon
- Quality and dose-accuracy concerns persist; the FDA has flagged inconsistent labeling and dosing on some telehealth-marketed compounded tirzepatide products
- Patients should verify 503A pharmacy accreditation, dose specifications, and clinician-prescription pathway before assuming compounded access is straightforward
The compounded tirzepatide market in 2026 is more complicated than it was in 2024. When the FDA had tirzepatide on its shortage list (2022-2024), 503A compounding pharmacies could legally produce tirzepatide based on bulk drug substance for individual patient prescriptions. When the shortage was officially resolved in October 2024, the legal basis for routine compounded tirzepatide narrowed substantially. The compound has not disappeared from the compounding pharmacy landscape, but the access pathway is more constrained than it was, and the FDA has been more active in enforcement.
This article covers the current legal status of compounded tirzepatide, the practical access pathways that remain, pricing reality versus branded Zepbound, quality and dose-accuracy concerns to verify, and how the compounded segment is likely to evolve through 2026-2027.
The shortage status timeline
Compounded tirzepatide's regulatory history is tied directly to FDA shortage classification:
| Period | Tirzepatide shortage status | 503A compounding implication |
|---|---|---|
| Pre-2022 | Not approved for chronic weight management | Limited compounding demand |
| 2022 | Approved as Zepbound for weight management | Demand surge began |
| 2022-Oct 2024 | On FDA shortage list | Broad 503A compounding permitted |
| Oct 2024 | Removed from shortage list | 503A access narrowed |
| Late 2024 - 2025 | Off shortage list but high demand | Compounded availability under enforcement scrutiny |
| 2026 | Off shortage, demand continues | 503A access for clinically-justified individual prescriptions only |
When a drug is on the FDA shortage list, 503A compounding pharmacies have broad legal latitude to produce bulk-substance-derived versions because the commercial supply cannot meet demand. When the shortage is resolved, the legal basis for routine 503A compounding narrows to specific clinical justifications (allergies to branded formulation excipients, dose customization needs that commercial product cannot accommodate, and similar individual patient cases).
The October 2024 shortage resolution was a major shift. The volume of compounded tirzepatide production fell substantially in late 2024 - early 2025. The market has remained active for clinically-justified prescriptions but is no longer the broad-access channel it was at peak shortage.
Current legal access pathways
In May 2026, three pathways for compounded tirzepatide remain legally viable:
1. Clinician-justified individual prescriptions. A licensed clinician can write a prescription specifying compounded tirzepatide for an individual patient where the commercial product is clinically inappropriate. Common justifications include allergies to commercial formulation excipients, dose customization needs (specific doses not available in commercial pens), or specific clinical situations requiring custom formulations.
2. 503B outsourcing facility production. 503B outsourcing facilities operate under different rules than 503A pharmacies. They can produce larger-batch compounded products under cGMP compliance. Whether 503B facilities can produce tirzepatide depends on their specific registration and the FDA's enforcement position on bulk drug substance use.
3. Patient-specific 503A compounding with documented clinical reasoning. The narrower path that remains for 503A pharmacies producing tirzepatide. Documentation requirements are more rigorous than during the shortage period.
What is no longer broadly available: routine 503A compounded tirzepatide for general weight management prescriptions where commercial Zepbound is clinically appropriate.
For broader regulatory context, see the compounding pharmacy peptide access guide 2026 and the FDA 503A peptide compounding review July 2026.
Pricing reality
The compounded vs branded tirzepatide pricing gap remains substantial:
| Channel | Monthly cost (2026 baseline) | Notes |
|---|---|---|
| Branded Zepbound (cash pay) | $1,000-$1,400/month | Direct Lilly pricing |
| Branded Zepbound (manufacturer coupon, eligible) | $500-$650/month | Patient-specific eligibility |
| Compounded tirzepatide (503A, clinician-prescribed) | $300-$500/month | Variable by pharmacy and dose |
| Research-grade retail tirzepatide | $80-$150 per 10mg vial | Multi-month supply per vial |
The compounded price advantage versus cash-pay branded is approximately 60-70% off. Versus branded with manufacturer coupon, the compounded discount is more modest (20-40%). For patients without insurance or coupon eligibility, the compounded option remains meaningfully cheaper. For patients with good insurance coverage of branded Zepbound, the math may favor branded.
Research-grade retail tirzepatide pricing reflects the separate regulatory channel (research-use disclosures, not for human consumption). This is not directly comparable to compounded or branded prescription products.
For the broader GLP-1 pricing comparison, see the generic semaglutide patent expiry timeline 2026.
Quality and dose-accuracy concerns
The FDA has flagged compounded GLP-1 quality issues several times through 2024-2026:
Dose accuracy. Compounded tirzepatide preparations have been observed with actual peptide content varying from labeled dose by more meaningful margins than commercial product. Most reputable 503A pharmacies are within typical compounding accuracy ranges, but variability exists.
Salt form differences. Some compounded tirzepatide has been produced as tirzepatide acetate or other salt forms different from the branded mesylate salt. The biological equivalence at therapeutic doses is presumed but not formally established.
Labeling clarity. Compounded products have used labeling that conflated tirzepatide acetate with tirzepatide and produced patient confusion about doses and pharmacokinetics.
Mixing additional compounds. Some compounded tirzepatide products combine tirzepatide with other compounds (B12, NAD+, lipotropics) without clear clinical justification. These combinations have not been studied for safety or efficacy.
Bottom line: Quality varies. PCAB-accredited 503A pharmacies with documented dose validation are the safer subset. Telehealth-marketed compounded tirzepatide should be verified carefully for pharmacy credentials, dose specification, and additive content.
How to evaluate a compounded tirzepatide source
Five practical verification questions:
1. Is the dispensing pharmacy PCAB-accredited? PCAB accreditation indicates quality system commitment beyond minimum 503A requirements. Not all 503A pharmacies are PCAB-accredited; the ones that are have demonstrated additional quality systems.
2. What salt form is the tirzepatide? Branded Zepbound is tirzepatide mesylate. Compounded preparations may be different salt forms. Ask the pharmacy specifically and document the answer.
3. What is the verified peptide content? The pharmacy should be able to provide content verification for the lot dispensed. This is the equivalent of a COA for the compounded preparation.
4. Are additional compounds included? Compounded tirzepatide should generally be tirzepatide alone, not combined with other compounds like B12, NAD+, or lipotropics. If the formulation includes additives, ask for the clinical justification.
5. What is the clinical prescribing justification? With the FDA shortage status resolved, the legal basis for compounded tirzepatide requires individual clinical justification. The prescribing clinician should document this rationale.
For our broader vendor evaluation framework applicable to compounding pharmacies and research peptide vendors, see the best legit peptide vendors 2026 ranking.
What might change through 2026-2027
Three regulatory and market developments to watch:
1. The July 2026 PCAC vote. The Pharmacy Compounding Advisory Committee will vote on the 503A bulks list in July 2026. The committee's recommendations on tirzepatide bulk drug substance availability will influence ongoing compounding access. See the FDA 503A peptide compounding review article.
2. Possible Lilly enforcement actions. Lilly has periodically taken enforcement actions against compounding pharmacies and telehealth platforms producing or marketing compounded tirzepatide. Continued enforcement pressure may further constrain access.
3. Generic tirzepatide timeline. Tirzepatide's US composition-of-matter patent expires approximately 2036-2037. Generic competition will not affect the 2026-2027 compounded tirzepatide market materially.
Compounded tirzepatide versus other compounded GLP-1s
For context, the compounded GLP-1 landscape in 2026 includes several compounds with different status:
| Compound | FDA shortage status | 503A compounding status |
|---|---|---|
| Tirzepatide | Off shortage (Oct 2024) | Narrowed; individual clinical justification |
| Semaglutide | Off shortage (Feb 2025) | Narrowed; similar individual justification |
| Liraglutide | Off shortage | Limited compounding demand |
| Retatrutide | Not approved | Not compoundable |
The semaglutide situation parallels tirzepatide's: shortage resolved, broad compounding access narrowed, individual-justification pathway remaining. For semaglutide-specific coverage, see the Wegovy HD 7.2 mg STEP UP trial guide.
Sourcing context
For prescription compounded tirzepatide through licensed 503A pharmacies, the access pathway is via clinician prescription as described above. The compounding pharmacy peptide access guide 2026 walks through the prescription process.
For research-grade tirzepatide vials (the research-use channel, not prescription), Ascension Peptides ships injectable tirzepatide with public per-batch COAs and 50% off using code ENHANCED. The tirzepatide reconstitution chart covers research dose-by-volume math.
FAQ
Is compounded tirzepatide still legal in 2026?
Yes, but the legal basis has narrowed since the October 2024 FDA shortage resolution. 503A compounding pharmacies can still produce tirzepatide for individual patient prescriptions where the commercial product is clinically inappropriate. Routine compounded tirzepatide for general weight management (where commercial Zepbound is clinically appropriate) is no longer broadly compoundable.
How much does compounded tirzepatide cost?
Typically $300-$500/month through licensed 503A pharmacies in 2026. Branded Zepbound cash-pay runs $1,000-$1,400/month; with manufacturer coupon for eligible patients, approximately $500-$650/month. The compounded discount is meaningful versus cash-pay branded but more modest versus coupon-eligible branded.
Is compounded tirzepatide safe?
In principle, yes, when produced by PCAB-accredited 503A pharmacies with documented quality systems. The FDA has flagged dose accuracy and labeling concerns at some telehealth-marketed compounded tirzepatide products. Patients should verify pharmacy credentials, dose specifications, and additive content before accepting.
What is the difference between branded and compounded tirzepatide?
Both contain tirzepatide as the active ingredient. Branded Zepbound is tirzepatide mesylate produced by Lilly under FDA approval. Compounded tirzepatide may use the same or different salt form, is produced by a 503A or 503B pharmacy under compounding regulations, and is prepared for individual patient prescriptions rather than commercial sale.
Will compounded tirzepatide disappear?
Probably not entirely, but it will likely become more constrained. With FDA shortage resolved and enforcement active, the broad compounded tirzepatide market that existed during 2022-2024 has narrowed. Patients with specific clinical justifications can still access compounded tirzepatide, but the practical volume is lower than peak shortage.
Can I get compounded tirzepatide via telehealth?
Yes, in many states, but the regulatory landscape has tightened. See the telehealth peptide prescription legality state-by-state 2026 article for state-by-state variation. Compounded GLP-1 telehealth has faced particular state-level scrutiny in 2025-2026.
When will generic tirzepatide be available?
Tirzepatide's US composition-of-matter patent expires approximately 2036-2037. Generic launches are unlikely before late-decade, with biosimilars potentially earlier under the BPCIA pathway but still several years out. The 2026-2027 compounded tirzepatide market is the main alternative-pricing channel until generic launches.
Further reading
- Tirzepatide reconstitution chart 10mg & 15mg
- Tirzepatide vs Semaglutide 2026 head-to-head
- Compounding pharmacy peptide access guide 2026
- Telehealth peptide prescription legality state-by-state 2026
- FDA 503A peptide compounding review July 2026
- Generic semaglutide patent expiry timeline 2026
- GLP-1 dosing comparison 2026
- Wegovy HD 7.2 mg STEP UP trial guide
- Best legit peptide vendors 2026
This article is for educational and informational purposes only. Tirzepatide is FDA-approved as Mounjaro for type 2 diabetes and Zepbound for chronic weight management and obstructive sleep apnea. Compounded tirzepatide preparations are produced under 503A compounding regulations for individual patient prescriptions. None of the content above constitutes medical advice. Patients should consult a qualified clinician for individual decisions about tirzepatide therapy.