At a glance
- Jensterle 2019 RCT (n=30, 16 weeks): liraglutide 3.0 mg raised LH and FSH and total testosterone, while TRT raised testosterone but suppressed gonadotropins
- Gregorič 2025 RCT (n=25, 24 weeks): semaglutide 1 mg improved sperm morphology while TRT injection worsened sperm concentration and total sperm number
- Trifirò 2025 controlled pilot (n=83, 2 months): tirzepatide raised total and free testosterone more than transdermal TRT in obese men with metabolic hypogonadism
- Able 2024 TriNetX cohort (3,094 men per arm, propensity-matched): non-diabetic men prescribed semaglutide for weight loss had 4.5-fold higher new erectile dysfunction incidence
- No GLP-1 RA is FDA-approved for hypogonadism. The functional-hypogonadism reversal signal is real, but the early-treatment ED signal in non-diabetic men is also real
The question this article actually answers
Three randomized or controlled trials have now compared a GLP-1 receptor agonist directly against testosterone replacement therapy in obese men with low testosterone. Liraglutide first (Jensterle et al., Endocrine Connections 2019, PMID 30707677). Semaglutide next (Gregorič et al., Diabetes Obes Metab 2025, PMID 39511836). Tirzepatide most recently, in a controlled pilot (Trifirò et al., Reprod Biol Endocrinol 2025, PMID 40604795). None of these are huge phase 3 cardiovascular outcome trials. Together they cover roughly 138 men across three GLP-1 receptor agonists, all of them with obesity-driven low testosterone, all of them randomized or allocated against a TRT comparator that was the standard of care for this phenotype.
The reader question is not "do GLP-1 receptor agonists move testosterone." That answer is yes, repeatedly, in every published study. The reader question is whether the testosterone movement is large enough, durable enough, and accompanied by enough functional benefit to make GLP-1 monotherapy a reasonable alternative to TRT plus gonadorelin or HCG for a man whose biggest problem is that he is 35 kg overweight and his total testosterone is 280 ng/dL with normal-low LH. That is the actual decision in the clinic, and the actual decision behind most "should I run semaglutide before I start TRT" forum threads.
Bottom line: In obese men with functional hypogonadism, GLP-1 receptor agonists raise testosterone by treating the upstream cause (visceral adiposity and the inflammatory suppression of LH pulse amplitude). TRT raises testosterone by replacing the downstream hormone and shutting off the pituitary signal. Both work for the lab number. They are not the same intervention, and they do not produce the same fertility, body-composition, or HPTA outcome.
Why obesity drops testosterone in the first place
Obesity-driven low testosterone is a discrete clinical phenotype, not just "low T plus extra weight." The mechanism is well-mapped: visceral adipose tissue overexpresses aromatase, which converts testosterone to estradiol, raises circulating estradiol, and applies central negative feedback to the hypothalamus. LH pulse amplitude drops. Leydig cell stimulation drops with it. Add the inflammatory cytokine load of metabolic syndrome (TNF-alpha, IL-6) and the central kisspeptin-GnRH circuit gets further suppressed, which is why the kisspeptin libido and fertility research is on the same axis as this one. Insulin resistance lowers SHBG, which means total testosterone underestimates the free testosterone deficit. The result is a man with low total T, low-normal LH, elevated estradiol, low SHBG, and a clinical syndrome that maps cleanly to "functional" or "secondary" hypogonadism.
A 2026 Andrology review by Jensterle and Janež (Jensterle and Janež, Andrology 2026) argues that this is the exact phenotype the field has been treating wrong for a decade. Conventional TRT in a man with obesity-driven low T fixes the lab number but does not touch the upstream cause. The pituitary is now suppressed by the exogenous testosterone load on top of the obesity load. Sperm parameters often drop further. Visceral fat falls only modestly. A man on TRT for obesity-driven low T is now permanently on TRT, with a baseline testicular volume that has shrunk and a sperm count that is much harder to recover.
Italian endocrine society guidance and several US andrology consensus documents now flag functional hypogonadism as the place where weight loss should precede testosterone replacement when feasible. GLP-1 receptor agonists matter here because they are the first weight-loss class to produce 15 to 21% sustained body weight reduction in non-bariatric outpatients, which is enough magnitude to actually flip the aromatase-LH-Leydig pathway in trial-relevant timeframes.
The Jensterle 2019 RCT: liraglutide vs TRT, 16 weeks
The first head-to-head was Jensterle's prospective randomized open-label trial (PMID 30707677). Thirty obese men with functional hypogonadism (mean age 46.5 ± 10.9 years, BMI 41.2 ± 8.4 kg/m^2) who had failed lifestyle measures were randomized to liraglutide 3.0 mg subcutaneous daily or 50 mg of 1% transdermal testosterone gel daily for 16 weeks.
Lab numbers came in roughly tied for testosterone but split apart on the HPTA. Total testosterone rose by 5.9 ± 7.2 nmol/L in the TRT arm and 2.6 ± 3.5 nmol/L in the liraglutide arm. The headline difference: LH and FSH rose in the liraglutide arm and fell in the TRT arm, which is the predicted result of liraglutide reversing the upstream suppression versus TRT applying exogenous negative feedback. The liraglutide arm lost 7.9 ± 3.8 kg of body weight. The TRT arm lost 0.9 ± 4.5 kg.
| Outcome at 16 weeks | Liraglutide 3.0 mg | Transdermal TRT |
|---|---|---|
| Total testosterone change | +2.6 ± 3.5 nmol/L | +5.9 ± 7.2 nmol/L |
| LH | Significant rise | Suppressed |
| FSH | Significant rise | Suppressed |
| Body weight | -7.9 ± 3.8 kg | -0.9 ± 4.5 kg |
| AMS symptom score | Improved | Improved |
The conclusion the authors drew is the one most often missed in subsequent coverage: liraglutide and TRT produced equivalent improvements in androgen-deficiency symptoms (AMS score) and libido despite the testosterone delta favoring TRT. The reason is that the liraglutide arm's improvement was driven by weight loss, restored gonadotropin signaling, and the metabolic-syndrome rollback that goes with 8 kg of weight off the visceral compartment. The TRT arm's improvement was driven by the testosterone delivery itself. Two paths, similar symptom outcome at 16 weeks, very different long-term physiology.
The Gregorič 2025 RCT: semaglutide vs TRT, 24 weeks, with sperm endpoints
Gregorič and colleagues extended the question to sperm parameters and longer follow-up (PMID 39511836). Twenty-five obese men with type 2 diabetes and functional hypogonadism (mean age 50, BMI 35.9 kg/m^2) were randomized to semaglutide 1 mg weekly or intramuscular testosterone undecanoate 1000 mg every 10 to 12 weeks for 24 weeks.
Sperm endpoints are the part of this trial that matters most. Semaglutide improved sperm morphology over 24 weeks. TRT injection significantly reduced sperm concentration and total sperm number, which is the predicted spermatogenesis cost of exogenous testosterone suppressing intratesticular testosterone via LH downregulation. Both arms raised total testosterone and improved symptoms of hypogonadism. Semaglutide produced significantly greater body weight reduction.
| Outcome at 24 weeks | Semaglutide 1 mg/week | TRT undecanoate |
|---|---|---|
| Total testosterone | Increased | Increased |
| Sperm morphology | Improved | Unchanged or worse |
| Sperm concentration | Maintained | Significantly reduced |
| Total sperm number | Maintained | Significantly reduced |
| Body weight | Significantly greater loss | Modest loss |
| Hypogonadism symptoms | Improved | Improved |
The clinical translation: a man trying to preserve fertility while addressing low testosterone has a genuinely different decision than a man who is past family-building. The Gregorič data is the first randomized direct comparison that quantifies that distinction in trial-grade terms. The mechanism for the divergence is straightforward. TRT suppresses LH, which suppresses intratesticular testosterone production, which suppresses spermatogenesis. Semaglutide does not touch the HPTA directly. It removes the upstream metabolic suppression by removing the visceral fat, and the testicle resumes work. This is the cleanest version of the "treat the cause, not the lab value" argument the field has made for a decade.
Tip: If fertility preservation is on the table, the Gregorič 2025 RCT is the strongest published evidence to bring to a clinic conversation. The sperm-morphology and total-sperm-number numbers came from a 24-week paired RCT, not a registry or a retrospective cohort, which is meaningfully stronger evidence than most of the GLP-1 reproductive-health literature.
The Trifirò 2025 tirzepatide pilot: dual-agonism extends the signal
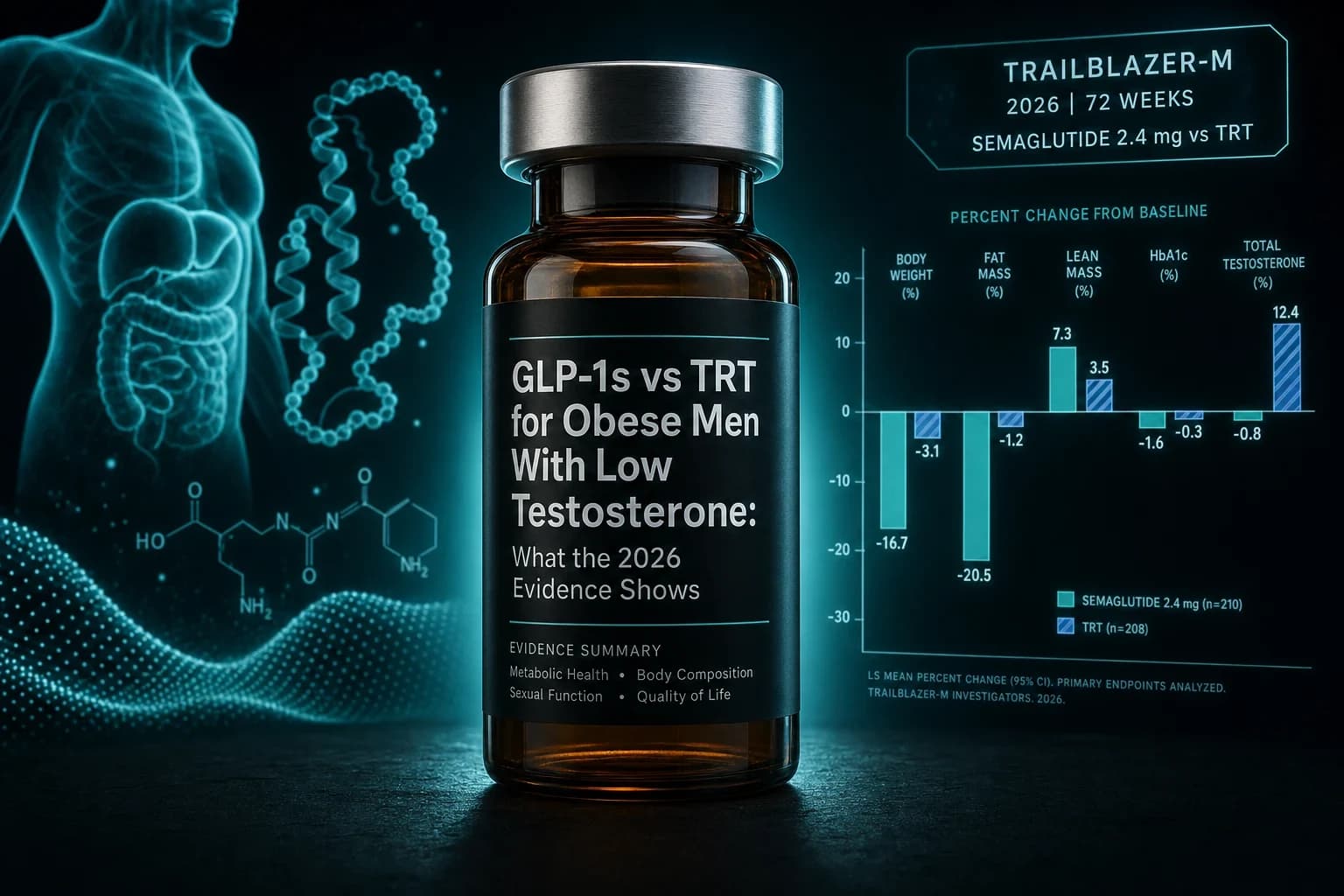
Tirzepatide's GIP plus GLP-1 mechanism produces more weight loss than semaglutide in head-to-head trials (Aronne et al., N Engl J Med 2025, SURMOUNT-5). The Trifirò pilot (PMID 40604795) asked whether the larger weight loss translates into a larger testosterone response. Eighty-three obese men with metabolic hypogonadism were allocated to one of three groups: tirzepatide titrated from 2.5 mg to 5 mg weekly plus lifestyle, transdermal testosterone plus lifestyle, or lifestyle alone. Outcomes at two months included testosterone, LH, FSH, SHBG, estradiol, IIEF-5 erectile function, body composition, and eating-behavior questionnaires.
At two months, tirzepatide plus lifestyle produced larger increases in both total and free testosterone than transdermal TRT plus lifestyle and substantially larger increases than lifestyle alone. Tirzepatide also produced larger improvements in BMI, waist circumference, and fat mass than the TRT arm. The IIEF-5 erectile function score improved in the tirzepatide arm, consistent with the testosterone rise plus the metabolic and vascular improvements that come with rapid visceral fat reduction.
The pilot is small, short (two months), and non-randomized. The body of the paper is honest about that. What it adds is mechanistic continuity. A GLP-1 monoagonist (semaglutide) at 24 weeks and a GIP plus GLP-1 dual agonist (tirzepatide) at two months both reverse the testosterone deficit in this phenotype, both outperform transdermal TRT on body composition, and tirzepatide pushes the testosterone delta further than transdermal TRT in this short window. Whether retatrutide's triple agonism stretches that signal further is an open question. The retatrutide TRIUMPH-1 phase 3 topline program does not include male-fertility endpoints to date.
The flip side: the Able 2024 TriNetX erectile dysfunction signal
The signal that complicates the optimistic reading is Able 2024 (PMID 38778151). Using the TriNetX research network, the authors identified non-diabetic men aged 18 to 50 with BMI greater than 30 who were prescribed semaglutide for weight loss after June 2021. Men with prior ED, prior PDE5 inhibitor use, prior testosterone prescription, prior radical prostatectomy, or other relevant exclusions were removed. After propensity matching, semaglutide-exposed men had a significantly higher incidence of new erectile dysfunction diagnosis or new PDE5 inhibitor prescription (1.47% vs 0.32%; relative risk 4.5; 95% CI 2.3 to 9.0) compared with matched non-exposed obese men. New testosterone deficiency diagnoses were also more frequent in the semaglutide arm.
This is the result most published commentary has rounded to "Ozempic causes ED" or "Ozempic causes low T," and both formulations overstate the database. What the data supports more precisely: in the early months of a non-diabetic weight-loss exposure to semaglutide, healthcare-encounter-recorded ED diagnoses and PDE5 prescriptions rise. The absolute event rate is low. The hazard ratio is real. The mechanism is not nailed down in the paper. Plausible drivers include rapid weight loss in itself altering libido and sexual function, GI side effects suppressing libido during titration, the well-known dehydration and reduced volume status during titration affecting erectile hemodynamics, and the underlying baseline differences a TriNetX propensity match cannot fully erase.
The Trifirò pilot, by contrast, showed IIEF-5 improvement on tirzepatide at two months. The Jensterle and Gregorič RCTs both showed improved sexual function and AMS or libido symptoms on GLP-1 monotherapy. The reconciliation that fits all four results: in obese men with established functional hypogonadism, GLP-1 receptor agonists improve sexual function alongside testosterone normalization. In non-hypogonadal younger obese men exposed to semaglutide for weight loss, there is an early-treatment incidence of new ED diagnosis that exceeds matched comparators. These are not contradictory findings. They are findings from different patient phenotypes.
| Study | Population | Comparator | Result |
|---|---|---|---|
| Jensterle 2019 (PMID 30707677) | n=30, obese hypogonadal men, BMI 41 | Transdermal TRT | Liraglutide raised LH, FSH, TT; equivalent symptom improvement |
| Gregorič 2025 (PMID 39511836) | n=25, T2D + obese + hypogonadal | TRT undecanoate IM | Semaglutide improved sperm morphology; TRT reduced sperm count |
| Trifirò 2025 (PMID 40604795) | n=83, obese metabolic hypogonadism | Transdermal TRT or lifestyle | Tirzepatide had larger TT, FT, body-composition response |
| Able 2024 (PMID 38778151) | TriNetX, non-diabetic obese men 18-50 | Matched obese, no semaglutide | 4.5-fold higher new ED diagnosis on semaglutide |
| Giagulli 2015 (PMID 26447645) | T2D obese, overt hypogonadism on TRT | TRT plus lifestyle plus metformin | Adding liraglutide further improved erectile function (IIEF-5) |
What this means for the man considering TRT
The practical question is whether to start TRT, start a GLP-1 receptor agonist, or stack them. The published trials do not let anyone answer that question for an individual patient, but they do let the field define which phenotype maps to which decision.
A man with a BMI above 32, a waist circumference above 102 cm, a total testosterone in the 200 to 350 ng/dL range, an LH in the low-normal or normal range, and an estradiol that is high relative to total testosterone is the Jensterle, Gregorič, and Trifirò phenotype. The trial data favor a GLP-1 receptor agonist trial before TRT in this phenotype, because the upstream cause is treatable and the testicle can come back. The fertility and HPTA preservation argument is strongest here.
A man with a normal BMI, a normal estradiol, a low LH, and a primary testicular issue (Klinefelter, post-radiation, prior anabolic steroid use with HPTA suppression that has not recovered, or testicular trauma) is not the phenotype these trials address. GLP-1 receptor agonists do not fix primary hypogonadism. The decision in this phenotype runs through TRT plus the HCG or gonadorelin protocols covered in the gonadorelin TRT article, not through metabolic weight loss.
A man somewhere in the middle, with both metabolic and primary contributors, is the population where the Giagulli 2015 study (PMID 26447645) is most relevant. Giagulli added liraglutide to lifestyle, metformin, and existing TRT in obese T2D men with overt hypogonadism, and erectile function on the IIEF-5 improved further than TRT alone. The combination approach is not contradicted by the Gregorič sperm data because the sperm cost of TRT is largely independent of whether a GLP-1 is added on top. If fertility is on the table, the GLP-1-first sequence is the safer move regardless of phenotype.
Warning: None of these published trials enrolled men under 35 with a normal BMI, normal estradiol, and primary testicular hypogonadism. Generalizing the Jensterle, Gregorič, and Trifirò findings to that phenotype would be a misuse of the data. The trials answer a specific clinical question about obesity-driven secondary hypogonadism, not the general question of "do GLP-1 receptor agonists fix low testosterone."
The body composition overlay
GLP-1 receptor agonists drive 15 to 21% body weight reduction in non-diabetic obese populations and 9 to 18% in T2D populations. Roughly 75% of the loss is fat mass and 25% is lean mass in DXA substudies of SURMOUNT-1 and STEP. The GLP-1 muscle loss research review covers the lean-mass detail. The relevance to a man making the TRT versus GLP-1 decision is that the lean-mass loss on GLP-1 monotherapy is the strongest argument for either keeping resistance training intense throughout the weight loss phase or, in selected cases, considering TRT plus GLP-1 stacking after the metabolic phenotype has corrected.
Tirzepatide's body-composition advantage (larger fat-mass loss for similar lean-mass loss) in SURMOUNT-1 maps onto the Trifirò testosterone advantage at two months. Whether the magnitude difference persists at 12 and 24 months is unstudied. The tirzepatide vs semaglutide SURMOUNT-5 head-to-head covers the weight-loss comparison in detail but does not stratify by male hormone outcomes. The combined picture: tirzepatide produces more weight loss, more visceral fat loss, more testosterone response in the early phase, and the same lean-mass concern as semaglutide.
The fertility window
The GLP-1 fertility long-term effects research review covers the female fertility side. On the male side, the published literature is small but directionally consistent. Semaglutide preserved or improved sperm parameters in Gregorič 2025. Liraglutide raised LH and FSH in Jensterle 2019, which is the upstream signal for spermatogenesis. Tirzepatide raised LH in the Trifirò pilot. None of these trials produced data on pregnancy outcomes in partners of treated men, because the trial durations and sample sizes were not designed for that endpoint. The systematic reviews flagged the field as data-poor on conception outcomes, and the ENDO 2026 Endocrine Society session on this framed the area as an open research question.
Practical translation: a man who wants to conceive in the next 6 to 12 months and has obesity-driven low testosterone has a stronger case for GLP-1 monotherapy than for TRT, by the available trial data. A man who is firmly past the conception window has fewer reasons to favor one over the other on fertility grounds, and the choice falls back to body composition, symptom outcome, and side-effect profile.
Side effects and the dose-context
GLP-1 side effects are well-characterized: GI symptoms (nausea, constipation, occasional vomiting) during titration, dose-dependent and time-limited. The semaglutide titration schedule (0.25 mg, 0.5 mg, 1.0 mg, 1.7 mg, 2.4 mg) is standard, and the tirzepatide schedule (2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg) is parallel. For dosing math by vial concentration, the reconstitution calculator handles the conversion.
On the testosterone side, the side-effect profile is also well-characterized: erythrocytosis with hematocrit drift, estradiol elevation, acne, sleep apnea worsening, and the HPTA suppression covered above. The shared decision in the clinic comes down to two different long-term commitments with very different reversibility profiles. A six-month GLP-1 trial is reversible. A multi-year TRT course produces durable testicular atrophy and durable HPTA suppression that often requires HCG, hMG, or clomiphene to undo. That reversibility asymmetry favors trying the GLP-1 first when the phenotype is obesity-driven.
The compounded-tirzepatide and compounded-semaglutide supply context is covered in the compounded tirzepatide 2026 legal access and supply guide and the generic semaglutide patent expiry timeline. Both are relevant because cost pressure is one of the biggest reasons men in this phenotype skip the GLP-1 trial and go straight to TRT.
Where the evidence is still thin
Three RCT or controlled cohorts is not the same as the SELECT, SURMOUNT, or FLOW evidence base for cardiovascular and renal endpoints. The total enrolled sample across Jensterle, Gregorič, and Trifirò is roughly 138 men. None of the trials ran beyond 24 weeks. None enrolled men under 30. None recruited men with primary testicular hypogonadism. The IIEF, AMS, and ADAM symptom-scale outcomes are subjective. The sperm count and morphology endpoints in Gregorič 2025 were measured in only one of the three trials. None of the GLP-1 receptor agonists carries a regulatory indication for hypogonadism, and none is likely to in the near term, because the regulatory pathway for a new "men with obesity-driven low T" indication is not commercially priority for the sponsors when the same drugs are already approved for the broader obesity indication that captures these patients anyway.
What the field needs next: longer RCTs with sperm count, motility, and morphology as pre-specified endpoints; sub-studies of the existing SURMOUNT and STEP populations stratified by baseline testosterone; dedicated trials in the post-anabolic-steroid recovery phenotype (where the HPTA suppression cause is different but the metabolic overlay is often similar); and the obvious negative-control trial of GLP-1 receptor agonists in non-obese men with primary hypogonadism, to confirm the directional argument that the testosterone effect runs entirely through the visceral fat and metabolic-syndrome pathway.
Access and supply
GLP-1 receptor agonists for the obesity-driven hypogonadism use case are off-label for that indication everywhere. Compounded semaglutide and compounded tirzepatide are the access routes most patient forums discuss when insurance coverage is denied. The compounded tirzepatide access guide, the telehealth peptide prescription legality state-by-state guide, and the best legit peptide vendors review for 2026 cover the practical access routes. Injectable semaglutide and tirzepatide reference vials are available from Ascension Peptides with code ENHANCED for 50% off.
For the oral route, the oral semaglutide Rybelsus vs orforglipron comparison is the cleanest read on bioavailability and dose math. The head-to-head testosterone trials above all used subcutaneous formulations and have not been replicated with oral GLP-1 receptor agonists.
What an honest physician conversation sounds like
The trial data is the evidence base for a specific clinical conversation, not a marketing pitch. The honest physician version reads roughly as follows: "Your testosterone is low. Your BMI is in the obesity range. The mechanism is your visceral fat raising estradiol and your inflammatory load suppressing your LH pulse amplitude. There are two paths. One is testosterone replacement, which will fix the number quickly, suppress your sperm count and testicular function as a side effect, and commit you to indefinite injections to maintain. The other is a GLP-1 receptor agonist, which will take six months to produce comparable testosterone numbers, will preserve or improve your sperm count, will produce 10 to 15% body weight reduction as a bonus, and is reversible if you tolerate it poorly or want to stop. If fertility is on the table, the trial evidence favors the second path. If you are past family-building and want fast symptom relief, the first path has decades of safety and dosing data behind it. The combination is reasonable in selected cases."
That is the conversation the Jensterle, Gregorič, Trifirò, and Able papers, taken together, support. It is not the conversation the broader internet is having about either class of drug, and it is the reason this article exists.
This article is for educational and research purposes only and is not medical advice. No GLP-1 receptor agonist is FDA-approved for the treatment of hypogonadism, low testosterone, infertility, or erectile dysfunction. Testosterone replacement therapy is a regulated prescription medication with its own indications, contraindications, and monitoring requirements that belong to an endocrinologist or qualified prescribing clinician, not to a general-audience review article. The trials summarized above enrolled small numbers of men with a specific clinical phenotype (obesity-driven functional hypogonadism), and generalizing the findings to primary testicular hypogonadism, post-anabolic-steroid HPTA recovery, age-related testosterone decline, or any other clinical phenotype would be a misuse of the data. The Able 2024 TriNetX signal of increased erectile dysfunction incidence on semaglutide in non-diabetic men is a real published finding and should be discussed with a prescriber before any GLP-1 receptor agonist is started for any indication. Do not start, switch, stop, or self-source semaglutide, tirzepatide, liraglutide, or testosterone replacement therapy on the basis of this article. Consult a qualified endocrinologist or men's health clinician about your individual circumstances before acting on any information here.