At a glance
- He L 2022 JAMA Intern Med (76 RCTs, n=103,371): GLP-1 RAs raised composite gallbladder/biliary disease risk RR 1.37 (95% CI 1.23-1.52).
- Weight-loss indication subgroup (13 trials): RR 2.29 (95% CI 1.64-3.18) vs RR 1.27 in trials for diabetes or other conditions.
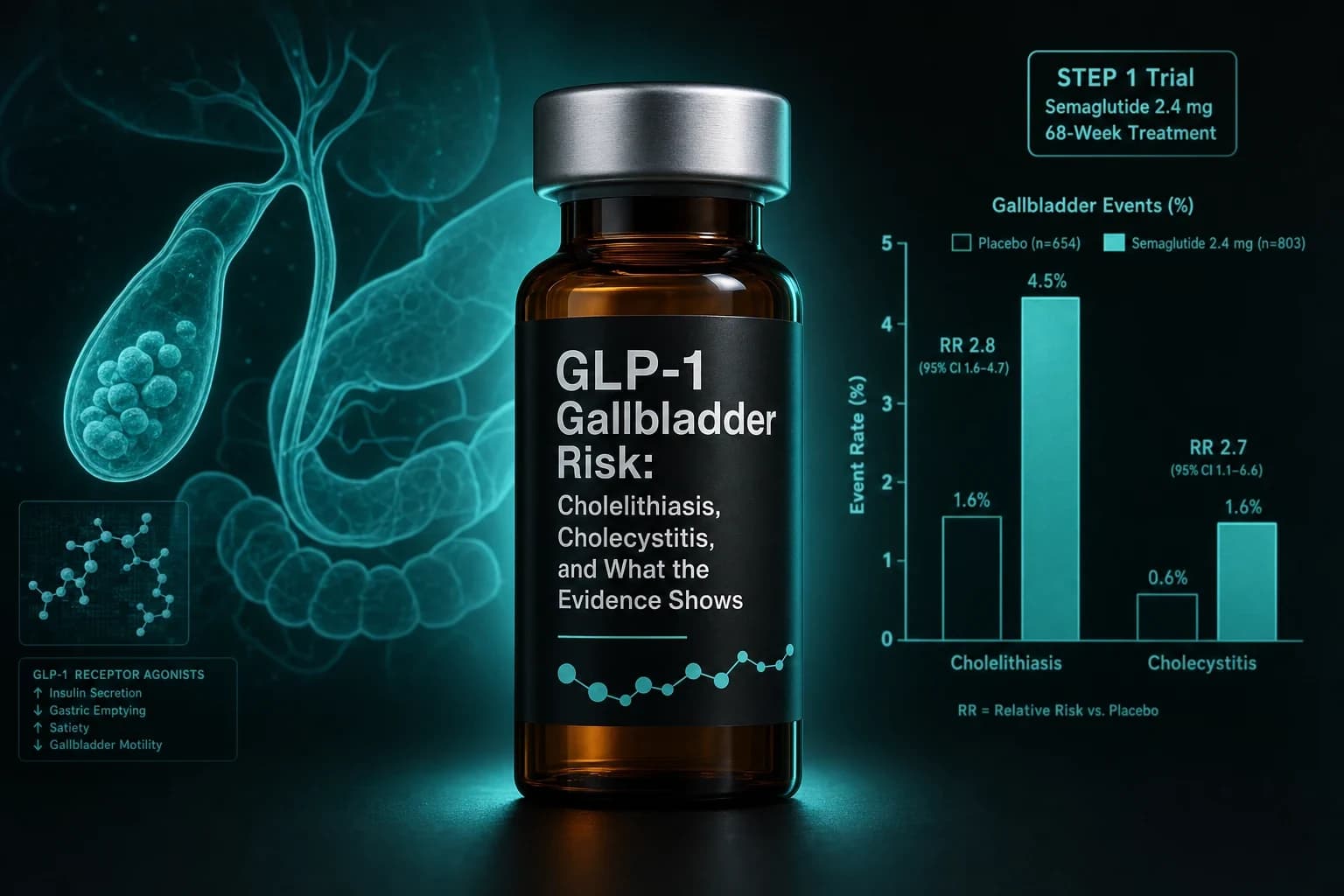
- STEP 1 (Wilding 2021, PMID 33567185): cholelithiasis 1.6% on semaglutide 2.4 mg vs 0.7% on placebo over 68 weeks; all gallbladder events 2.6% vs 1.2%.
- Gong 2025 J Diabetes Investig (PMID 39569606, 12 RCTs, n=12,351): tirzepatide RR 1.52 for gallbladder/biliary disease and RR 1.67 for cholelithiasis vs comparators.
- Absolute risk is modest: He estimated roughly 27 extra gallbladder/biliary cases per 10,000 GLP-1-treated person-years, concentrated in higher-dose weight-loss use.
The one GLP-1 safety signal that keeps replicating
For most of the GLP-1 safety conversation, the headline alarm changes shape from cohort to cohort. Pancreatitis looked huge in 2023 and shrank in the 2024 to 2026 active-comparator literature (Sodhi et al., JAMA 2023, PMID 37796527; see our GLP-1 pancreatitis evidence breakdown). The thyroid C-cell signal from rodents has not replicated in human cohorts (semaglutide thyroid cancer review). The NAION ophthalmology story is one positive cohort plus a stack of mixed cohorts.
Gallbladder disease is the safety signal that has not softened. The 76-trial meta-analysis from He L and colleagues at Peking Union Medical College Hospital reported a 37 percent relative increase in gallbladder or biliary disease across 103,371 randomized patients, with a 129 percent increase in the weight-loss-indication subset (He L et al., JAMA Intern Med 2022, DOI 10.1001/jamainternmed.2022.0338). The STEP 1 obesity registration trial put cholelithiasis at 1.6 percent on semaglutide 2.4 mg versus 0.7 percent on placebo over 68 weeks (Wilding et al., NEJM 2021, PMID 33567185). A 2025 meta-analysis of 12 tirzepatide RCTs put the relative risk for gallbladder or biliary disease at 1.52 and for cholelithiasis at 1.67 (Gong et al., J Diabetes Investig 2025, PMID 39569606). The FDA's pharmacovigilance team published 36 cases of acute cholecystitis on GLP-1 RAs that lacked gallbladder warnings on label, with 21 of 36 on exenatide (Woronow et al., JAMA Intern Med 2022, PMID 36036939). A 2025 FAERS disproportionality analysis identified 1,829 GLP-1-RA primary-suspect reports and significant positive signals on all three signal-detection methods (Wang et al., Front Pharmacol 2025, PMID 40697657).
Bottom line: Across randomized trials, pharmacovigilance databases, and dedicated meta-analyses, GLP-1 receptor agonists modestly increase the absolute incidence of gallstones, cholecystitis, and biliary disease. The relative effect is larger at higher doses, longer durations, and in obesity-indication use. The absolute event rate is still single-digit percentages over a year of treatment, and the clinical implication is risk awareness and early symptom triage, not blanket avoidance.
This piece walks through what the He 2022 meta-analysis actually reported, how the STEP and SURMOUNT registration trials line up, what the dedicated tirzepatide data add, what the FDA pharmacovigilance system has caught, what the mechanism appears to be, and how to read this against a real GLP-1 protocol. For broader safety context, see the GLP-1 pancreatitis risk guide, the pre-surgery aspiration guide, and the GLP-1 dosing comparison.
Why gallbladder is on every GLP-1 label
Gallbladder warnings appeared on GLP-1 labels long before the 2022 meta-analysis. Liraglutide carried a gallbladder disease label statement based on LEADER and the SCALE obesity trials. Semaglutide picked up the same language in SUSTAIN and STEP. Tirzepatide added it after SURMOUNT and SURPASS. The label posture is consistent: increased reporting of cholelithiasis and cholecystitis, warning to evaluate for gallbladder disease if symptoms develop, no contraindication in patients with prior cholelithiasis.
Three things keep gallbladder on the label across this class:
- The mechanism is biologically plausible at the receptor. GLP-1 receptors are expressed on the gallbladder and biliary tree, and acute GLP-1 receptor activation slows gallbladder emptying in mechanistic studies, which is exactly the physiology that promotes bile stasis and stone formation.
- The signal replicates across trials. Most weight-management GLP-1 RCTs report a small absolute excess of gallbladder events versus placebo even when no formal hypothesis test is pre-specified.
- The signal scales with rapid weight loss. Rapid weight loss from any cause, including bariatric surgery and very-low-calorie diets, is itself a well-established gallstone risk factor. The weight-loss-indication GLP-1 trials reproduce this in placebo-controlled randomized data.
The He 2022 meta-analysis is the single piece of evidence that consolidated this from "individual trial signals" into "class-level RCT-grade effect."
What the He L 2022 meta-analysis actually showed
He L, Wang J, Ping F and colleagues at Peking Union Medical College Hospital pooled 76 randomized trials of GLP-1 receptor agonists versus placebo or active comparators across diabetes, obesity, NAFLD, and cardiovascular outcome populations. The combined sample was 103,371 patients with a mean age of 57.8 years.
The primary composite endpoint was any gallbladder or biliary disease. The secondary endpoints split that composite into cholelithiasis, cholecystitis, biliary disease, and biliary cancer.
The summary effects (He L et al., JAMA Intern Med 2022, DOI 10.1001/jamainternmed.2022.0338):
| Endpoint | Relative risk (95% CI) | Interpretation |
|---|---|---|
| Gallbladder or biliary disease (composite) | 1.37 (1.23-1.52) | 37% relative increase across all trials |
| Cholelithiasis | 1.27 (1.10-1.47) | Gallstone formation specifically |
| Cholecystitis | 1.36 (1.14-1.62) | Gallbladder inflammation |
| Biliary disease (non-stone) | 1.55 (1.08-2.22) | Cholangitis, sludge, ductal events |
| Weight-loss indication (13 trials) | 2.29 (1.64-3.18) | High-dose, longer-duration use |
| Diabetes or other (63 trials) | 1.27 (1.14-1.45) | Lower-dose chronic use |
The dose-response and duration-response patterns matter for protocol design. Higher-dose trials and longer-duration trials had numerically larger relative risks, although the dose-by-RR and duration-by-RR interactions did not reach formal statistical significance in the He analysis. The indication subgroup difference (RR 2.29 weight loss vs RR 1.27 diabetes-and-other) is the more reliable read.
The absolute number is what stops this from being a class veto. He estimated approximately 27 additional gallbladder or biliary disease cases per 10,000 GLP-1-RA-treated person-years. Against a baseline acute cholecystitis incidence in the general adult population of roughly 200 to 250 cases per 100,000 per year and gallstone prevalence around 10 to 15 percent in adult Western populations, a 27-per-10,000 absolute excess is a real but bounded effect.
What the STEP and SURMOUNT obesity trials reported
The He meta-analysis aggregated trial data, but the per-trial obesity numbers are worth seeing on their own.
STEP 1, the 68-week semaglutide 2.4 mg obesity registration trial, randomized 1,961 adults with BMI 30 or higher (or 27 plus a weight-related comorbidity) to semaglutide or placebo on top of lifestyle support (Wilding et al., NEJM 2021, PMID 33567185). On the published gallbladder side:
- Cholelithiasis: 1.6 percent on semaglutide 2.4 mg vs 0.7 percent on placebo
- All gallbladder-related adverse events: 2.6 percent on semaglutide vs 1.2 percent on placebo
- Acute cholecystitis: roughly 0.6 percent on semaglutide vs 0.2 percent on placebo
- The semaglutide arm lost 14.9 percent of body weight at 68 weeks vs 2.4 percent on placebo
In raw counts, the gallbladder excess is small per trial. It is the consistency of the pattern across STEP 1, STEP 3, STEP 4, and STEP 5 that made it land on the Wegovy product monograph as a labeled risk.
SURMOUNT-1 randomized 2,539 adults with obesity to tirzepatide 5, 10, or 15 mg or placebo for 72 weeks (Jastreboff et al., NEJM 2022, PMID 35658024). The gallbladder readout in SURMOUNT-1 was less dramatic than STEP 1: cholelithiasis was roughly 0.6 to 1.1 percent across tirzepatide doses versus 0.8 percent on placebo, with no clear dose response on cholelithiasis itself. Cholecystitis ran modestly higher on tirzepatide than placebo at the highest dose (around 0.6 percent vs 0.2 percent) but the absolute event counts were too small to draw a strong inference from a single trial.
The single-trial signal in obesity is small. The pattern that makes gallbladder disease a labeled class effect is the consistency across trials, populations, and analyses.
Tirzepatide specifically: the 2025 meta-analyses
Two dedicated tirzepatide meta-analyses sharpened the dual-agonist picture.
Du and colleagues pooled nine tirzepatide RCTs across SURPASS and SURMOUNT (n=9,871) and reported that the composite of gallbladder or biliary disease was significantly associated with tirzepatide vs placebo or basal insulin (Du et al., Front Endocrinol 2023, PMID 37908750). Pancreatitis was not significantly increased in this analysis, consistent with the broader GLP-1 pancreatitis literature.
Gong and colleagues expanded the search to 12 tirzepatide RCTs (n=12,351) and reported sharper results (Gong et al., J Diabetes Investig 2025, PMID 39569606):
| Endpoint | RR (95% CI) | Notes |
|---|---|---|
| Gallbladder or biliary disease (composite) | 1.52 | Significantly elevated vs comparators |
| Cholelithiasis | 1.67 | Gallstones specifically |
| Cholecystitis | Trended higher | Did not reach significance in subgroup |
| Pancreatitis | Not significant | Consistent with class-wide pancreatitis pattern |
The Gong result is roughly in the same neighborhood as the He composite for the full GLP-1 class (RR 1.37) but slightly higher for cholelithiasis specifically. The natural reading is that tirzepatide produces a gallbladder signal at least as strong as semaglutide, not the lower-risk profile that early SURMOUNT-1 single-trial numbers might have suggested.
The mechanism for the dual GIP/GLP-1 agonist is not meaningfully different from the GLP-1-mono mechanism. Adding GIP receptor activation does not appear to offset the GLP-1-mediated gallbladder hypomotility effect.
What the FDA pharmacovigilance signal adds
Pharmacovigilance does not establish causation. It does flag class-wide adverse event reporting patterns that registration trials may have missed at their sample sizes.
The Woronow paper from the FDA Division of Pharmacovigilance reviewed FAERS reports from 2005 to 2016 and identified 36 cases of acute cholecystitis associated with GLP-1 receptor agonists where the labeled gallbladder language did not exist at the time of reporting (Woronow et al., JAMA Intern Med 2022, PMID 36036939). Twenty-one of the 36 cases were on exenatide, the oldest molecule in the class. Median time to event was around 5 weeks of GLP-1 exposure, suggesting that the gallbladder events cluster in the early treatment window rather than only after months of weight loss.
The 2025 update from Wang and colleagues used FAERS data through Q2 2024 and applied three disproportionality metrics (reporting odds ratio, proportional reporting ratio, Bayesian confidence propagation neural network) to the entire database. They identified 1,829 GLP-1-RA primary-suspect reports involving 1,651 patients with cholecystitis or cholelithiasis (Wang et al., Front Pharmacol 2025, PMID 40697657). All three signal-detection methods produced positive signals across the class. The median onset time was 182 days, with the majority of cases in patients aged 45 or older and a female predominance.
The two FAERS analyses together produce a coherent picture: the gallbladder signal exists at the regulatory database level, scales with cumulative class exposure (older drugs have more reports), and presents with a wide onset window that includes both early-exposure events (weeks) and later events (six months).
Why gallbladder events happen on GLP-1s: three contributors
The mechanism behind GLP-1-associated gallbladder disease is multifactorial. Three components are well characterized at the physiology level. None of them require speculative pathway claims.
1. GLP-1 receptor activation slows gallbladder emptying. GLP-1 receptors are expressed on biliary epithelium and gallbladder smooth muscle. Acute GLP-1 receptor agonist administration reduces postprandial gallbladder ejection fraction in mechanistic human studies. Slower emptying means longer dwell time for bile, which favors cholesterol crystallization and stone formation.
2. Rapid weight loss is itself a gallstone risk factor. The relationship between rapid weight loss and gallstones is well documented in the bariatric surgery and very-low-calorie diet literature. The intensity of cholesterol mobilization during rapid lipolysis raises biliary cholesterol saturation, and reduced caloric intake reduces postprandial cholecystokinin release, which is the main driver of gallbladder emptying. Both effects favor sludge and stone formation. He's weight-loss-indication subgroup (RR 2.29) versus diabetes subgroup (RR 1.27) lines up with this mechanism: the bigger the weight loss, the bigger the relative effect.
3. CCK-mediated emptying is reduced. GLP-1 receptor activation appears to attenuate the cholecystokinin signaling that normally triggers postprandial gallbladder contraction. The net effect is the same as the direct receptor mechanism: less postprandial emptying, more bile stasis.
Two of these three mechanisms (rapid weight loss and CCK attenuation) are downstream of the GLP-1 receptor binding. The direct receptor effect on the gallbladder is the part that explains why patients with no significant weight loss on lower-dose diabetes-indication GLP-1 RA use still show a measurable, smaller excess of gallbladder events.
Risk stratification table
The He data and the per-trial obesity readouts together support a simple stratification.
| Risk profile | Approximate relative risk vs no GLP-1 | Notes |
|---|---|---|
| Lower-dose GLP-1 RA for type 2 diabetes (e.g., semaglutide 0.5 or 1 mg, dulaglutide 0.75 or 1.5 mg) | ~1.2 to 1.3 | Smallest weight loss, smallest absolute excess |
| Semaglutide 2.4 mg or tirzepatide weight-loss dosing | ~1.5 to 2.3 | Largest weight loss, largest relative effect |
| Pre-existing cholelithiasis (asymptomatic) | Higher absolute, similar relative | No formal contraindication; symptom monitoring matters more |
| Patient with prior cholecystectomy | Not at risk for stones | Could still develop biliary tree or sphincter of Oddi events; absolute risk small |
| Patient with very rapid early loss (>1.5% body weight per week) | Higher absolute | Loss rate, not target dose, is the proximate driver |
| Older age plus female sex | Higher absolute baseline | Background gallstone risk pulls absolute event rate up |
This table is not a license to skip the patient-specific risk conversation. It is the structure that conversation should follow.
What this means in practice
Several practical implications fall out cleanly from the evidence above:
- Symptom triage matters. The clinical risk to manage is not asymptomatic gallstones (which are common at baseline) but symptomatic biliary disease, especially acute cholecystitis. Right upper quadrant pain that persists more than a couple of hours, post-prandial pain that radiates to the right shoulder, fever, or jaundice all warrant urgent evaluation. The Woronow data suggest events cluster in the first weeks of treatment as well as later in the loss curve, so early-cycle symptoms should be taken seriously.
- Rate of loss is a modifiable variable. Slower titration and protein-adequate diets are associated with lower gallstone risk in the broader rapid-weight-loss literature. Whether protocol modifications meaningfully change GLP-1 RA gallbladder event rates has not been directly tested in a randomized trial, but the mechanism is consistent.
- Prior cholecystectomy removes the gallstone-and-cholecystitis risk specifically. It does not change pancreatitis or other class effects.
- Indication and dose drive most of the risk. A patient on tirzepatide 15 mg for obesity has a meaningfully different gallbladder risk profile from a patient on dulaglutide 0.75 mg for diabetes. The class label flattens this; the data do not.
- Imaging is not routine. No major guideline supports routine pre-treatment ultrasound. The cost-benefit math on screening an asymptomatic adult considering semaglutide does not favor universal imaging. Symptom-driven workup is the default.
For the people running compounded or research-grade GLP-1 protocols, the same risk-stratification logic applies. The mechanism does not depend on the supply chain.
Where to source research-grade GLP-1 compounds
Researchers working with semaglutide, tirzepatide, and retatrutide can find these injectables from Ascension Peptides with 50% off using code ENHANCED. Source quality and purity verification through an independent certificate of analysis sit at the foundation of any safety conversation: known mass, known identity, known purity. The gallbladder mechanism is the same whether the molecule comes from a brand-name pen or a research vial, so risk awareness matters at any source.
Frequently Asked Questions
Does Ozempic cause gallstones?
Yes, modestly, at the population level. Across 76 RCTs and 103,371 patients, GLP-1 receptor agonists raised gallbladder or biliary disease risk by 37 percent overall (He L et al., JAMA Intern Med 2022, DOI 10.1001/jamainternmed.2022.0338). In STEP 1, cholelithiasis ran 1.6 percent on semaglutide 2.4 mg versus 0.7 percent on placebo over 68 weeks (Wilding et al., NEJM 2021, PMID 33567185). The relative effect is larger at weight-loss doses than at diabetes doses, and the absolute excess works out to roughly 27 extra gallbladder events per 10,000 person-years.
Is tirzepatide safer for the gallbladder than semaglutide?
Not based on the dedicated meta-analyses. Gong 2025 pooled 12 tirzepatide RCTs (n=12,351) and reported a composite gallbladder/biliary risk RR of 1.52 with cholelithiasis RR 1.67 (Gong et al., J Diabetes Investig 2025, PMID 39569606). That is at least as high as the GLP-1 class average. Earlier single-trial readouts from SURMOUNT-1 looked lower because the obesity trial was modest in size and the event counts were small. The larger pooled analyses do not support the dual-agonist being gallbladder-protective.
Why does this happen mechanistically?
Three contributors. First, GLP-1 receptor activation slows gallbladder emptying, increasing bile dwell time. Second, rapid weight loss from any cause increases cholesterol mobilization into bile and reduces postprandial gallbladder emptying, both of which favor stone formation. Third, GLP-1 RA appears to attenuate cholecystokinin signaling, which is the normal trigger for postprandial gallbladder contraction. The He weight-loss subgroup running RR 2.29 versus the diabetes subgroup at RR 1.27 is consistent with weight loss being a large component of the effect.
Should I get a gallbladder ultrasound before starting?
No major guideline recommends routine pre-treatment imaging in asymptomatic adults. The 27-per-10,000 absolute excess does not justify universal screening, and most pre-existing gallstones are asymptomatic and remain so. The relevant clinical move is symptom awareness, not imaging.
What symptoms should I watch for?
Right upper quadrant pain that lasts more than a couple of hours, especially after a meal. Pain that radiates to the right shoulder blade or upper back. Fever, chills, or jaundice. Persistent nausea after the typical GLP-1 nausea window has passed. The FDA pharmacovigilance data (Woronow et al., 2022, PMID 36036939; Wang et al., 2025, PMID 40697657) suggest events occur both in the early treatment window and out past six months, so a sudden GI presentation at any point in therapy is worth taking seriously.
Does the risk go away after stopping?
The labeled risk is associated with active treatment. Once stones have formed, they do not spontaneously dissolve, so the long-term consequence of a GLP-1-associated stone is the same as any other gallstone: it may stay silent, may eventually trigger symptoms, or may resolve with eventual cholecystectomy. Whether stopping the drug changes the future trajectory of an asymptomatic stone has not been directly studied.
Is this a reason to avoid GLP-1s?
For most people, no. The absolute excess is small and the cardiometabolic benefit at therapeutic weight-management doses is large. The risk is real and labelled, and it is one of the safety items worth discussing before starting, especially in someone with a personal or family gallstone history. For broader class safety, see the GLP-1 pancreatitis risk article and the pre-surgery aspiration guide.
This article is for educational and research purposes only and is not medical advice. Gallbladder and biliary disease can be serious and requires evaluation by a qualified clinician. All risk estimates, trial percentages, and safety details are drawn from published clinical research and regulatory pharmacovigilance databases. Consult a qualified healthcare professional before making any decision about GLP-1 therapy or about gallbladder symptoms during therapy.


