At a glance
- REIMAGINE 2 (Buse et al., Lancet Diab Endocrinol 2026): CagriSema 2.4/2.4 mg cut HbA1c 1.91 points and drove 14.2% weight loss over 68 weeks in 2,728 adults with T2D on metformin.
- Head-to-head vs semaglutide 2.4 mg alone, CagriSema won on HbA1c (1.91 vs 1.75 points) and on weight (14.2% vs 10.2%).
- REIMAGINE 3 (Rosenstock, Lancet 2026, PMID 42251856): add-on to basal insulin dropped HbA1c from 8.8% toward 6.5% in 274 adults with no severe hypoglycemia.
- REIMAGINE 1 (Frias, Lancet Diab Endocrinol 2026, PMID 42251860) tested CagriSema in drug-naive T2D for 40 weeks across 42 sites in six countries.
- CagriSema is not FDA approved for any indication. Novo Nordisk filed for weight management in December 2025 based on REDEFINE 1 and REDEFINE 2; the T2D file remains a REIMAGINE readout in review.
Novo Nordisk brought three Phase 3 CagriSema readouts to ADA 2026 in New Orleans. Two published in The Lancet Diabetes & Endocrinology the same week, one in The Lancet. The story most of the coverage led with was the head-to-head in REIMAGINE 2: cagrilintide plus semaglutide beat semaglutide 2.4 mg alone on both HbA1c and body weight in adults with Type 2 diabetes on metformin. The story that got less attention is that REIMAGINE 3 delivered a similar signal on top of basal insulin, and REIMAGINE 1 anchored the drug-naive population that Novo will need for a diabetes label.
CagriSema is the fixed-dose combination of cagrilintide, a long-acting amylin analogue, and semaglutide, the GLP-1 receptor agonist most clinicians already know from Ozempic and Wegovy. Both are once-weekly subcutaneous. The efficacy hypothesis is that amylin and GLP-1 hit different satiety pathways and different glycemic mechanisms, so the combination should outperform either agent alone. REIMAGINE 2 tested that head-to-head at matched doses. It is now the cleanest Phase 3 data in the amylin-GLP-1 combination space.
This walkthrough covers what the three REIMAGINE trials actually showed, how CagriSema compares to tirzepatide's SURPASS numbers and Novo's own semaglutide select cardiovascular data, what the safety table looks like, and where the regulatory picture sits as of July 2026. For the obesity-focused CagriSema story, the REDEFINE 1 Phase 3 guide is the sibling piece; this one stays inside the T2D lane.
What cagrilintide adds to semaglutide at the mechanism level
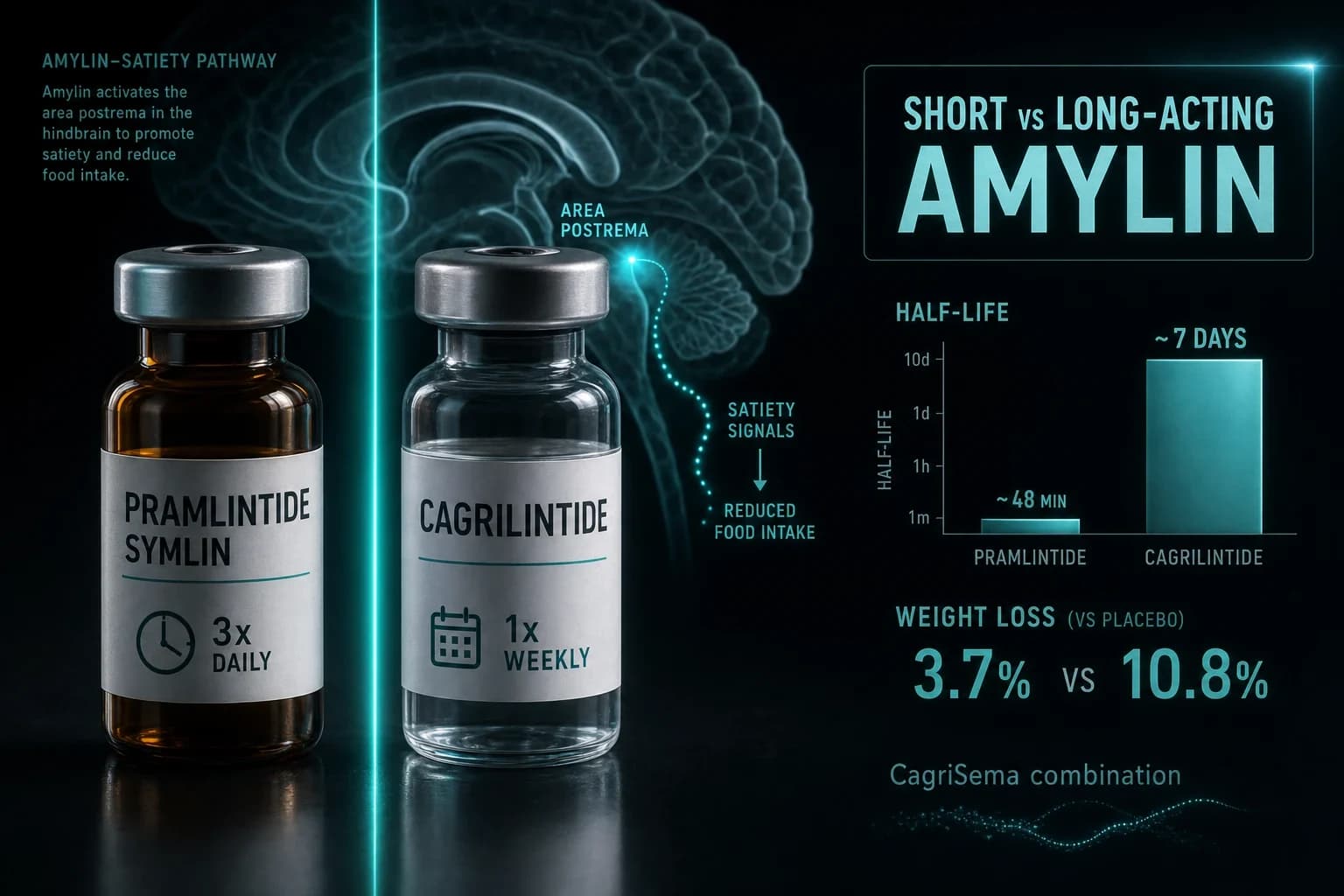
Cagrilintide is not a rebadged GLP-1. It is an analogue of amylin, the pancreatic beta-cell hormone that is co-secreted with insulin and modulates satiety, gastric emptying, and postprandial glucagon suppression. Native amylin has a plasma half-life of about 13 minutes. Cagrilintide is engineered to run about a week per subcutaneous injection, matching semaglutide's dosing schedule. That is the whole point of the coformulation.
The mechanistic case for adding cagrilintide to semaglutide, developed most clearly by Le Roux and colleagues in the Phase 2 T2D combination trial (Frias et al., Lancet 2023, PMID 37364590), rests on two ideas. First, amylin receptors in the area postrema drive satiety through a pathway that is separate from GLP-1 receptor signaling, so the two agents together produce more appetite suppression per unit dose than either alone. Second, amylin blunts postprandial glucagon, which addresses the residual glucagon liability that GLP-1 monotherapy does not fully close. Recent tracer work by Lutz and colleagues (Cell Metabolism 2025, PMC12270663) showed that cagrilintide lowers bodyweight through brain amylin receptors 1 and 3, which is the receptor-level anchor the field was missing.
For a wider view of what else is moving in this space, see the GLP-1 + amylin combination pipeline 2026 guide, the petrelintide amylin monotherapy Phase 2 evidence, and the eloralintide amylin receptor agonist Phase 2 evidence. CagriSema is the most advanced combination asset in the class. Petrelintide is the most advanced monotherapy contender. Eloralintide is the most receptor-selective contender inside Lilly.
REIMAGINE 2: the head-to-head that made the ADA session
REIMAGINE 2 is the trial that carries the class-level story. It was a 68-week, randomized, double-blind, parallel-group Phase 3 study run in 30 countries by Buse and colleagues (Lancet Diabetes Endocrinol 2026), registered as NCT06065540. Novo Nordisk enrolled 2,728 adults with Type 2 diabetes inadequately controlled on metformin with or without an SGLT2 inhibitor, BMI 25 or higher.
Randomization was to one of six arms: cagrilintide 2.4 mg plus semaglutide 2.4 mg, cagrilintide 1.0 mg plus semaglutide 1.0 mg, semaglutide 2.4 mg, cagrilintide 2.4 mg, semaglutide 1.0 mg, or matched placebo. All doses were once-weekly subcutaneous. Titration ran through the first 16 weeks. The primary endpoint was HbA1c change from baseline to week 68. Body weight change was a co-primary. Mean baseline HbA1c was 8.2%.
| Endpoint (week 68) | Placebo | Semaglutide 2.4 mg | Cagrilintide 2.4 mg | CagriSema 2.4/2.4 mg |
|---|---|---|---|---|
| Mean HbA1c change (points) | approximately -0.4 | -1.75 | approximately -1.0 | -1.91 |
| Mean body weight change | approximately -2.5% | -10.2% | approximately -8.5% | -14.2% |
| Composite HbA1c ≤ 6.5% + ≥10% weight loss | low single digits | approximately 30% | approximately 20% | 57% |
| Achieved ≥20% weight reduction | rare | mid-single-digit range | rare | approximately 24% |
Two features of this table matter more than the individual numbers.
First, the composite endpoint. Fifty-seven percent of the CagriSema 2.4/2.4 arm hit both an HbA1c at or below 6.5% and at least 10% weight loss. That is roughly double the rate on semaglutide 2.4 mg alone in the same trial. For clinical decision making in a T2D patient with obesity, that composite is the single most decision-relevant number the trial produced. It captures the idea that CagriSema does not force a tradeoff between glycemic control and weight management the way older T2D drugs did.
Second, the HbA1c superiority over semaglutide 2.4 mg (1.91 vs 1.75 points from a baseline near 8.2%) is real but small. If the target is an HbA1c near 6.5%, both arms get there on average. The larger delta is in weight, where CagriSema added about four percentage points over semaglutide 2.4 mg. Some editorial writing on the same trial has argued that the HbA1c delta, while statistically significant, is close to the noise floor for clinically meaningful glycemic effect.
Bottom line: REIMAGINE 2 gives the amylin-GLP-1 combination hypothesis its cleanest Phase 3 win in T2D. CagriSema beats semaglutide 2.4 mg on HbA1c and on weight. The HbA1c delta is modest. The weight and composite deltas are not.
REIMAGINE 1: drug-naive T2D and the placebo comparator
REIMAGINE 1 is the shorter, smaller trial designed to satisfy the drug-naive-population question a diabetes label will ask. Frias and colleagues (Lancet Diabetes Endocrinol 2026, PMID 42251860) ran a 40-week, randomized, double-blind, placebo-controlled Phase 3a study across 42 sites in six countries. Adults with T2D inadequately controlled on diet and exercise alone were randomized to CagriSema 2.4 mg/2.4 mg, CagriSema 1.0 mg/1.0 mg, or placebo. The primary endpoint was HbA1c change at week 40.
The design contrast with REIMAGINE 2 matters. REIMAGINE 1 tested the combination against placebo in an easier population (no background metformin, no baseline SGLT2 inhibitor). REIMAGINE 2 tested it against active semaglutide 2.4 mg in a harder, more real-world population. The drug-naive win in REIMAGINE 1 sets the label case. The active-comparator win in REIMAGINE 2 sets the positioning case.
At the ADA 2026 presentation, the CagriSema 2.4/2.4 mg arm reported HbA1c reduction that reached roughly the same 1.9-point magnitude as REIMAGINE 2 despite the shorter duration, and body weight reduction in the low-teens percent range from a baseline of 101 kg. Formal peer-reviewed numbers are in the Lancet paper published June 7, 2026. The 1.0/1.0 mg dose provided a proportional lower response, consistent with the dose-titration data from the earlier Phase 2 co-administration trial (Frias et al., Lancet 2023, PMID 37364590).
REIMAGINE 3: add-on to basal insulin
REIMAGINE 3 is the smallest of the three (n = 274) and the one that answers the question most endocrinology practices actually see. When a patient with T2D on basal insulin still is not at goal, what happens if CagriSema goes on top? Rosenstock and colleagues (Lancet 2026, PMID 42251856) ran the placebo-controlled Phase 3, published in The Lancet the same week as the REIMAGINE 1 and 2 papers.
The topline numbers from the ADA presentation and the Lancet paper were direct. Mean baseline HbA1c ran approximately 8.8%. Mean HbA1c on CagriSema 2.4/2.4 mg fell to approximately 6.5% at the primary endpoint, a change of roughly 2.3 points. Body weight fell by up to about 12% on the highest dose. Placebo produced a smaller improvement on both endpoints. Critically, no participant experienced a severe hypoglycemic episode over the trial, a result that matters given that background basal insulin was continued and titrated to a fasting glucose target.
Clinical logic here is different from REIMAGINE 2. A T2D patient on basal insulin is often trying to avoid intensification with prandial insulin or a sulfonylurea because those drugs add hypoglycemia and weight. CagriSema at REIMAGINE 3's numbers moves the patient toward an HbA1c goal while dropping body weight, without triggering the hypoglycemia signal you would see with prandial insulin. That is the case Novo will make for the basal-insulin add-on positioning, and it is the more interesting positioning case commercially. The springermedicine ADA 2026 summary is a useful non-paywalled reference to the same data.
Tip: For a T2D patient already on a weekly semaglutide 2.4 mg without adequate response, REIMAGINE 2 is the data that supports switching to CagriSema. For a T2D patient on basal insulin with residual HbA1c and weight burden, REIMAGINE 3 is the data that supports adding CagriSema on top rather than adding prandial insulin.
How CagriSema stacks against tirzepatide and the retatrutide pipeline
Cross-trial comparison is imperfect. The populations, backgrounds, and durations differ across the SURPASS, STEP, TRIUMPH, and REIMAGINE programs. Read the table as class-context, not head-to-head.
| Trial | Compound | Dose | Population | Duration | HbA1c change | Weight change | Reference |
|---|---|---|---|---|---|---|---|
| REIMAGINE 2 | CagriSema | 2.4/2.4 mg wk | T2D on metformin | 68 wk | -1.91 pts | -14.2% | Buse Lancet Diab Endocrinol 2026 |
| REIMAGINE 2 (comparator) | Semaglutide | 2.4 mg wk | Same trial arm | 68 wk | -1.75 pts | -10.2% | Same |
| SURPASS-2 | Tirzepatide | 5, 10, 15 mg wk | T2D on metformin | 40 wk | -2.30 pts (15 mg) | -12.4% (15 mg) | Frias NEJM 2021, PMID 34170647 |
| SUSTAIN-7 | Semaglutide | 1.0 mg wk | T2D on metformin | 40 wk | -1.8 pts | -6.5 kg | Pratley Lancet Diab Endocrinol 2018, PMID 29397376 |
| TRANSCEND-T2D-1 | Retatrutide | 12 mg wk | T2D on metformin | 40 wk | reported at ADA 2026 | -16.8% | Retatrutide TRANSCEND-T2D-1 evidence |
The read across the row is that tirzepatide 15 mg still holds the deepest single-agent HbA1c drop reported to date in a similar population, and retatrutide 12 mg leads on weight loss in T2D. CagriSema sits between them, closer to tirzepatide on weight than semaglutide 2.4 mg alone was and closer to semaglutide on HbA1c than tirzepatide 15 mg. The mechanism is different from both. See the Retatrutide vs tirzepatide vs semaglutide 2026 guide for the wider ranking. For a class explainer on dosing options, the GLP-1 dosing comparison 2026 guide is the sibling piece.
Commercial positioning is the tighter question. It is whether the amylin-GLP-1 combination mechanism opens a differentiated case versus the GLP-1/GIP dual and GLP-1/GIP/glucagon triple. Novo will argue that CagriSema is the only Phase 3 amylin-mechanism entrant, and that the composite HbA1c-plus-weight benefit is the T2D obesity case. Lilly will argue that tirzepatide already covers the population well and that retatrutide is the deeper weight solution. Both arguments will be reflected in the payer conversations that follow the 2026 filings.
Safety, tolerability, and hypoglycemia
The safety table across the three REIMAGINE trials was class-typical for a GLP-1-containing regimen, with a few CagriSema-specific notes.
- Gastrointestinal adverse events were the most common in the active arms, mostly mild-to-moderate nausea, vomiting, and diarrhea, concentrated during the titration window. The rate ran higher in the CagriSema 2.4/2.4 mg arm than in semaglutide 2.4 mg alone in REIMAGINE 2, consistent with adding a second appetite-suppressing agent.
- Injection-site reactions were reported at higher rates in cagrilintide-containing arms than in semaglutide alone in the earlier Phase 2 trial (Frias Lancet 2023, PMID 37364590), and the Phase 3 rates followed the same pattern.
- Severe hypoglycemia was absent in REIMAGINE 3 despite background basal insulin, which is the most policy-relevant single safety signal in the file.
- Discontinuation rates due to adverse events ran modestly higher on CagriSema 2.4/2.4 mg than semaglutide 2.4 mg alone, driven mostly by GI tolerability, and were manageable with titration adjustments in most participants.
- Class-level flags carried over from the semaglutide component: pancreatitis, gallbladder disease, retinopathy in patients with pre-existing diabetic retinopathy (see the SUSTAIN-6 retinopathy evidence guide), and the boxed thyroid C-cell tumor warning based on rodent data. The cagrilintide amylin-analogue component does not remove or reduce these flags.
For semaglutide's broader cardiovascular story, see the SELECT trial cardiovascular MACE evidence. REIMAGINE 2 was not powered for cardiovascular outcomes; a CVOT for CagriSema is not currently reported.
Warning: The combination adds tolerability burden versus semaglutide 2.4 mg alone. Real-world adherence outside the trial titration schedule is an open question. Do not assume the trial GI dropout rates translate cleanly to open-label practice.
Regulatory status and access as of July 2026
CagriSema is not FDA approved for any indication. Novo Nordisk filed with the FDA for weight management in December 2025 based on the obesity Phase 3 program (REDEFINE 1 and REDEFINE 2). The T2D filing follows the REIMAGINE readouts; timeline guidance from Novo has pointed to a late 2026 to 2027 submission window depending on how the FDA sorts the label breadth question.
Compounded CagriSema is not a category. Because cagrilintide is not on the FDA 503A bulks list, compounding pharmacies cannot legally produce cagrilintide preparations for patient use in the United States even under a shortage exemption. Compounded semaglutide operates in a separate regulatory space: it is available through some telehealth channels while the branded semaglutide shortage designation lasts. If you are already using compounded semaglutide for T2D and want to know what the CagriSema data implies for you, the honest answer is that no compounded amylin analogue is legally available in the US, and off-label attempts to reproduce the REIMAGINE 2 combination outside of an approved trial or an approved commercial product should not proceed.
For access to legitimate semaglutide sourcing through licensed providers, see the compounded semaglutide online overview and the Yucca Health telehealth review. If you are considering a semaglutide switch based on REIMAGINE 2's active-comparator data, that is a physician conversation, not a self-directed protocol change.
Limitations worth stating plainly
Three constraints deserve to sit alongside the numbers.
First, the CagriSema 2.4/2.4 mg dose is the top of the trial dose ladder. In real-world use, patients who cannot tolerate the top dose will land at 1.0/1.0 mg or an intermediate dose, and the efficacy will scale down. REIMAGINE 2's 1.0/1.0 arm reported roughly proportional numbers. Do not read the headline 14.2% weight loss as what an average T2D patient will experience.
Second, REIMAGINE 2 is a 68-week trial. The GLP-1 field is still working out what happens on years 3 through 5 of continuous therapy: weight regain on discontinuation, dose maintenance requirements, and long-term cardiovascular and cancer risks. See the stopping GLP-1s and weight regain research for the maintenance question. CagriSema has no dedicated long-term maintenance readout yet.
Third, the composite endpoint of HbA1c 6.5% or lower plus 10% or greater weight loss is a novel construct in T2D trials, and its regulatory weight depends on how the FDA sorts it in the label conversation. The FDA has historically preferred separate primary endpoints in T2D. If the CagriSema label is granted on separate primaries, the composite becomes a marketing point rather than a labeled claim, which changes how prescribers see it.
What REIMAGINE means for the T2D pipeline
Two shifts follow from these readouts.
First, GLP-1 monotherapy is no longer the default best-in-class for combined glycemic and weight goals. REIMAGINE 2's head-to-head vs semaglutide 2.4 mg puts a specific number on the value of adding an amylin analogue: roughly 0.16 HbA1c points and 4 percentage points of weight. That is not a small delta commercially. The tirzepatide vs semaglutide SURMOUNT-5 head-to-head established the same shift for the GLP-1/GIP dual mechanism in obesity; REIMAGINE 2 does it for the GLP-1/amylin combination in T2D.
Second, the amylin pathway is now a validated Phase 3 target for T2D, not a mechanistic curiosity. The petrelintide and eloralintide monotherapy Phase 2 programs will now be read against REIMAGINE 2's active-comparator win. Roche's petrelintide runs solo. Lilly's eloralintide runs as a companion or comparator inside the tirzepatide franchise. Whether either monotherapy can approach CagriSema's combination number in T2D is the open question through 2027.
For a wider view of the class ranking, the retatrutide vs tirzepatide vs semaglutide 2026 comparison is the sibling piece, and the pramlintide vs cagrilintide amylin explainer covers the amylin-class background.
Bottom line
CagriSema is not going to be a niche T2D drug if the REIMAGINE 2 numbers survive an FDA advisory conversation. A 14.2% weight loss with a 1.91-point HbA1c drop at 68 weeks in a metformin-background population is a headline commercial number for T2D obesity. The head-to-head vs semaglutide 2.4 mg is the most important single result because it converts the combination hypothesis from theory to a labeled positioning claim. REIMAGINE 3 fills in the basal-insulin add-on story that most endocrinology practices care about.
The two things worth watching next are the FDA action on the weight management filing already submitted in December 2025, and the T2D submission that follows the REIMAGINE readouts. Novo Nordisk has a clear commercial path if the labels arrive. Whether the tolerability burden of the combination affects real-world persistence at anything like the trial titration schedule is the question the label alone will not answer.
Related reading on the site
- Cagrilintide compound page
- Semaglutide compound page
- Cagrilintide dosage chart
- Semaglutide dosage chart
- CagriSema REDEFINE 1 obesity Phase 3 guide
- Pramlintide vs cagrilintide amylin explainer
- Petrelintide amylin monotherapy Phase 2 evidence
- Eloralintide amylin receptor agonist Phase 2 evidence
- GLP-1 + amylin combination pipeline 2026
- Retatrutide TRANSCEND-T2D-1 Phase 3 diabetes evidence
- Retatrutide vs tirzepatide vs semaglutide 2026
- Tirzepatide vs semaglutide SURMOUNT-5 head-to-head
- GLP-1 dosing comparison 2026
- Semaglutide SELECT cardiovascular MACE evidence
- GLP-1 diabetic retinopathy SUSTAIN-6 evidence
- Stopping GLP-1s and weight regain research
- Reconstitution calculator
- Compounded semaglutide online
- Yucca Health telehealth GLP-1 review
This article is for educational and research purposes only and is not medical advice. CagriSema (cagrilintide plus semaglutide) is not approved by the FDA, EMA, or MHRA for any indication as of July 2026. Novo Nordisk submitted CagriSema to the FDA for chronic weight management in December 2025 based on the REDEFINE 1 and REDEFINE 2 obesity trials; a Type 2 diabetes filing based on the REIMAGINE program has not been publicly confirmed at time of writing. Cross-trial comparisons between REIMAGINE, SURPASS, STEP, and TRIUMPH programs are context, not head-to-head. GLP-1 receptor agonists carry class-level risks including gastrointestinal adverse events, pancreatitis, gallbladder disease, worsening of pre-existing diabetic retinopathy, and a boxed thyroid C-cell tumor warning based on rodent data; adding cagrilintide does not remove these flags. Compounded cagrilintide and compounded CagriSema are not legally available in the United States. Any change to diagnosis, monitoring, or treatment of Type 2 diabetes or obesity should involve a licensed clinician familiar with your medical history and current medications.