At a glance
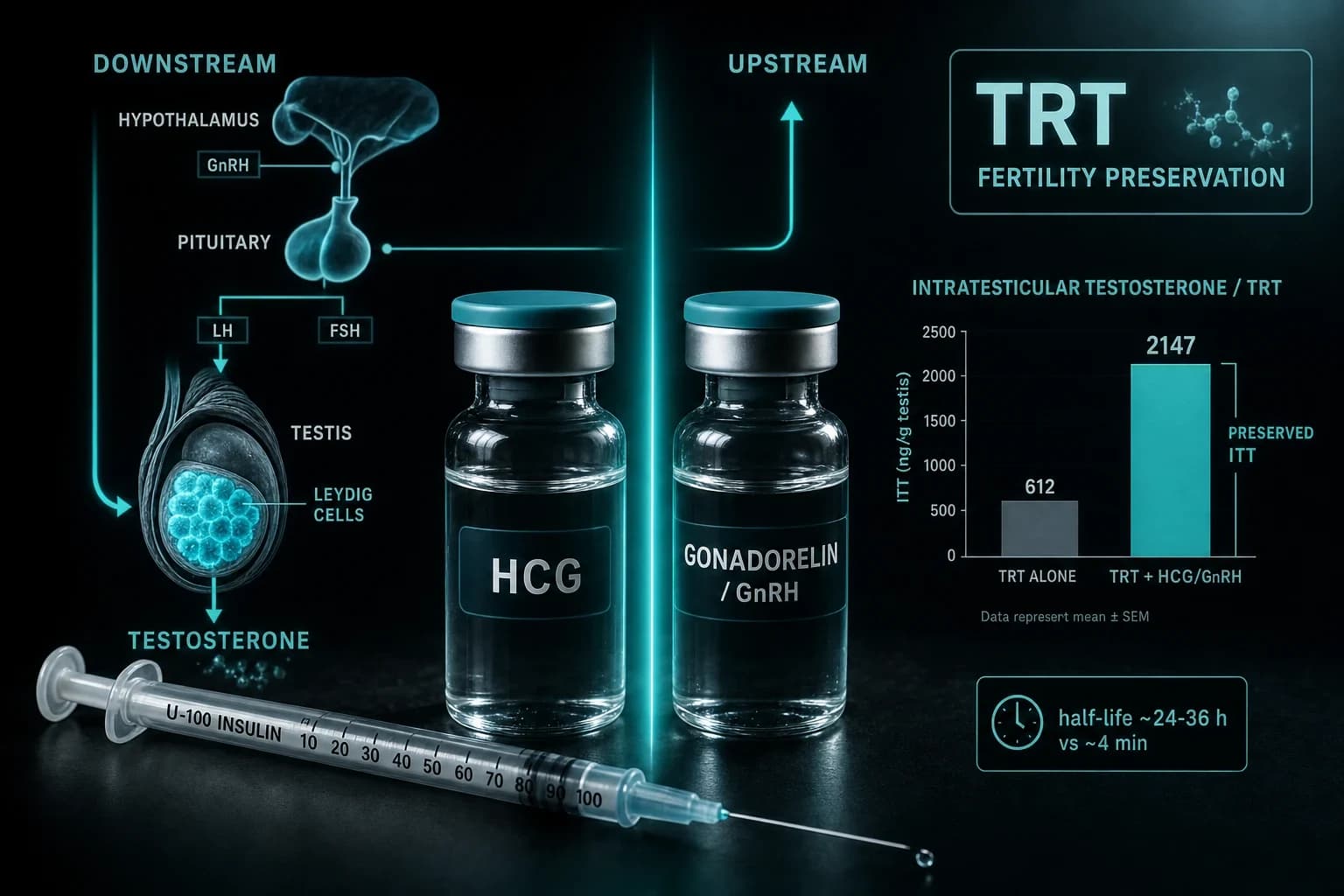
- TRT suppressed intratesticular testosterone by 94% in healthy men; hCG at 250 IU every other day held it near baseline (Coviello 2005)
- hCG has a ~24-36 hour half-life and is dosed 2-3x weekly; gonadorelin's half-life is 2-4 minutes and must be pulsed
- hCG acts downstream on Leydig cells and bypasses the pituitary; gonadorelin acts upstream and needs an intact, responsive pituitary
- On TRT + 500 IU hCG every other day, 0 of 26 hypogonadal men went azoospermic and 9 fathered pregnancies (Hsieh 2013)
- Continuous GnRH shuts the axis down; only pulsed delivery keeps it running (Belchetz 1978), which is gonadorelin's core dosing trap
Testosterone replacement fixes your blood work and quietly switches off your testicles. The same injection that pushes serum testosterone to the top of the range tells your pituitary to stop sending the two signals (LH and FSH) that keep sperm production and testicular volume alive. In one controlled study, exogenous testosterone crushed intratesticular testosterone by 94% (Coviello et al. 2005). That is the collapse men are trying to prevent.
Two compounds get used to keep that machinery online: hCG and gonadorelin. People treat them as interchangeable. They are not. They act at opposite ends of the same hormonal chain, they run on wildly different clocks, and choosing the wrong one is how researchers waste money and lose fertility anyway. Here is exactly where each one plugs in.
The axis you are trying to protect
Testicular function runs on a three-stop relay. The hypothalamus releases GnRH in short pulses. Those pulses hit the pituitary, which fires out luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH tells the Leydig cells in the testes to make testosterone locally; FSH drives the Sertoli cells that support sperm. The testosterone concentration inside the testis (intratesticular testosterone, or ITT) runs roughly 100 times higher than the level in your blood, and spermatogenesis depends on that gradient.
Exogenous testosterone breaks the relay at the top. Your brain reads the high serum level, assumes the job is done, and silences GnRH. LH and FSH fall to near zero, the Leydig cells go quiet, ITT collapses, and the testes shrink. Your blood testosterone looks great while the factory inside the testicle shuts its doors. Both hCG and gonadorelin exist to keep that factory open, but they knock on completely different doors.
HCG: a downstream stand-in for LH
Human chorionic gonadotropin is a hormonal impersonator. Its beta subunit is close enough to LH that it binds the same LH/CG receptor on Leydig cells, so it walks straight up to the testicle and does LH's job for it. It skips the hypothalamus and the pituitary entirely. Whatever is happening upstream, hCG still reaches the receptor.
That downstream position is its biggest practical advantage. It also carries a long fuse: hCG has a circulating half-life around 24 to 36 hours, versus roughly 20 minutes for native LH. One dose keeps stimulating Leydig cells for more than a day, which is why 2 to 3 injections per week (or every other day at low doses) is enough to hold the line.
The dose-response data is unusually clean. In Coviello et al. (2005), 29 healthy men got 200 mg testosterone enanthate weekly plus placebo or hCG at 125, 250, or 500 IU every other day. Placebo dropped ITT by 94%. Adding hCG restored it in a straight line with dose: 250 IU every other day landed ITT about 7% below baseline, and 500 IU pushed it 26% above baseline. A separate GnRH-antagonist model found ITT climbed dose-dependently on even smaller amounts, from 15 to 125 IU daily (Roth et al. 2010).
The fertility endpoint that matters most comes from Hsieh et al. (2013). Twenty-six hypogonadal men ran testosterone replacement alongside 500 IU hCG every other day. None became azoospermic during treatment, and 9 of the 26 contributed to a pregnancy. That is direct evidence for the exact scenario TRT users care about: keep the testosterone, keep the sperm.
Bottom line: hCG works because it ignores the broken part of the axis. It reaches past a suppressed pituitary and stimulates the testicle directly, with a long enough half-life to make twice-weekly dosing viable.
Gonadorelin: an upstream nudge to the pituitary
Gonadorelin is synthetic GnRH, the same decapeptide your hypothalamus releases. It does not touch the testicle. It binds GnRH receptors on the pituitary and asks that gland to release its own LH and FSH. So it sits one full step upstream of hCG: instead of doing the testicle's job, it tries to restart the natural signal that drives the testicle.
That design has a hard dependency baked in. Gonadorelin only works if the pituitary is intact and able to respond. If the pituitary itself is damaged (surgery, a tumor, radiation), gonadorelin has nothing to talk to and does nothing. hCG has no such requirement, because it operates below the pituitary entirely.
Then there is the clock. Gonadorelin's plasma half-life is roughly 2 to 4 minutes after intravenous delivery. Each dose is gone almost as fast as it arrives. That is not a flaw to engineer around; it is the entire point of how GnRH signaling works, and it is where most people get gonadorelin badly wrong.
Pulsatile vs continuous: the mistake that castrates
The single most important fact about GnRH signaling was established in monkeys almost fifty years ago. Belchetz et al. (1978) gave animals GnRH two ways. Delivered as a pulse once per hour, it kept LH and FSH flowing normally. Delivered as a constant infusion at the same total dose, it did the opposite: the pituitary desensitized and gonadotropin output shut down. Same molecule, same amount, opposite result. The pattern is the message.
This is not a lab curiosity. It is why GnRH agonists like leuprolide are used to chemically castrate men with prostate cancer. Flood the pituitary with continuous GnRH-like signal and it downregulates, then goes silent. Gonadorelin dosed the wrong way risks steering toward that same suppression instead of away from it.
Real pulsatile GnRH therapy solves this with a programmable pump that delivers a micro-dose every 90 to 120 minutes, mimicking the natural rhythm. At-home subcutaneous gonadorelin (typically one or two injections a day) is a rough approximation of that pump. Each shot produces a brief LH pulse and then clears, which does at least respect the pulsatile requirement, but it delivers far fewer pulses than the physiology asks for.
When it is done properly, pulsatile GnRH is powerful. In men with congenital hypogonadotropic hypogonadism (an intact pituitary starved of its hypothalamic signal), a pulsatile gonadorelin pump produced sperm at a median of 6 months versus 14 months for cyclical gonadotropin injections, with a 90% versus 83.3% success rate (Zhang et al. 2019). Note the population: those men had a working pituitary and a missing brain signal. That is gonadorelin's home turf, and it is not the same situation as a TRT user actively suppressing his own axis.
HCG vs gonadorelin at a glance
| Feature | HCG | Gonadorelin |
|---|---|---|
| Axis level | Downstream (testis) | Upstream (pituitary) |
| Molecular target | LH/CG receptor on Leydig cells | GnRH receptor on pituitary gonadotrophs |
| What it mimics | Luteinizing hormone (LH) | GnRH |
| Half-life | ~24-36 hours | ~2-4 minutes (IV) |
| Dosing frequency | 2-3x per week (or every other day) | Pulsed, ideally every 90-120 min; often 1-2x daily sub-q |
| Requires intact pituitary | No | Yes |
| Raises intratesticular testosterone | Directly | Indirectly, via released LH |
| Fertility evidence on TRT | Coviello 2005, Hsieh 2013 | Zhang 2019 (in CHH, not TRT) |
| Risk of desensitization | Low | High if dosed continuously |
So which one actually preserves fertility on TRT?
The published TRT fertility evidence sits almost entirely with hCG. Coviello proved it holds ITT in the normal range against full testosterone suppression, and Hsieh showed men on TRT plus hCG kept making sperm and fathered children. That is the specific question a TRT user is asking, answered directly.
Gonadorelin's strongest fertility data comes from hypogonadotropic hypogonadism, where the axis is quiet because the hypothalamic signal never arrives. Replace that missing pulse with a pump and the pituitary responds beautifully. But a TRT user is in a different fight. His exogenous testosterone is still actively hammering the hypothalamus with negative feedback. Subcutaneous gonadorelin is then trying to force brief pulses through a system that the testosterone is simultaneously trying to shut off. hCG avoids that tug-of-war completely by working below the level where the suppression happens.
So why did gonadorelin get popular for TRT at all? Largely supply and cost. When compounded hCG became harder to source in the United States, many clinics substituted gonadorelin because compounding pharmacies could produce it cheaply and it ships easily. Convenience and price drove that switch, not head-to-head fertility data on TRT.
Bottom line: For preserving fertility and testicular size on TRT, hCG has the direct human evidence and the simpler dosing. Gonadorelin is a reasonable upstream tool when the pituitary is intact and you can dose frequently, but on TRT it is fighting the current, and its TRT-specific fertility data is thin.
Where kisspeptin fits in the chain
If gonadorelin is one step upstream of hCG, kisspeptin is one step above that. It is a hypothalamic neuropeptide that drives the GnRH neurons themselves, effectively turning on the master switch rather than replacing any single downstream hormone. In healthy men, intravenous kisspeptin-54 raised LH from 4.2 to 10.8 U/L (roughly a 2.6-fold jump) along with FSH and testosterone (Dhillo et al. 2005).
Kisspeptin is investigational. There are no established at-home fertility protocols and no TRT preservation data behind it. It matters here only because it completes the map: kisspeptin drives the hypothalamus, gonadorelin drives the pituitary, and hCG drives the testis. Understanding those three tiers is what stops people from stacking redundant compounds or picking the wrong one for a damaged link.
Dosing realities
hCG in the research literature clusters around 250 to 500 IU, two to three times per week, run alongside TRT. It ships as a lyophilized powder and has to be reconstituted before use, so getting the concentration right is not optional. Run your vial and target dose through the reconstitution calculator before you draw a syringe, because a math error here is the difference between 250 IU and 2,500 IU.
Gonadorelin means more needles for less certainty. Its minutes-long half-life forces frequent dosing (commonly once or twice daily subcutaneously in the TRT context), and that schedule is still a coarse imitation of the every-90-minute rhythm the physiology actually wants. More injections, a narrower margin for dosing error, and less TRT-specific outcome data. That is the trade you are accepting for staying upstream.
Injectable hCG and gonadorelin are both available from Ascension Peptides with 50% off using code ENHANCED. Compare the full mechanism profiles on the hCG and gonadorelin pages, or browse the wider peptide library to see where each sits on the axis.
How to choose
Pick hCG if your priority is preserving testicular function and fertility on TRT with the strongest human evidence and the fewest injections. It is the default for a reason.
Pick gonadorelin if your pituitary is intact, you specifically want to keep the whole upstream axis firing rather than bypass it, and you can commit to frequent, correctly pulsed dosing. Its best-documented wins come from pump-driven protocols, not once-daily convenience.
Rule gonadorelin out entirely if the pituitary itself is the broken link. It has nothing to signal. hCG is the only one of the two that still works when the pituitary is offline.
These are hormones with real clinical uses and real ways to go wrong. The pulsatile-versus-continuous trap alone can turn a fertility protocol into a suppression protocol. Anyone weighing fertility preservation on TRT should be doing it with a clinician who can run LH, FSH, testosterone, and a semen analysis, not guessing from a forum thread.
Disclaimer: This article is for research and educational purposes only and is not medical advice. hCG, gonadorelin, and kisspeptin are hormones with clinical applications and meaningful risks. Nothing here is a recommendation to use, dose, or self-administer any compound. Consult a qualified physician before making any decision about testosterone replacement, fertility preservation, or hormonal therapy.