At a glance
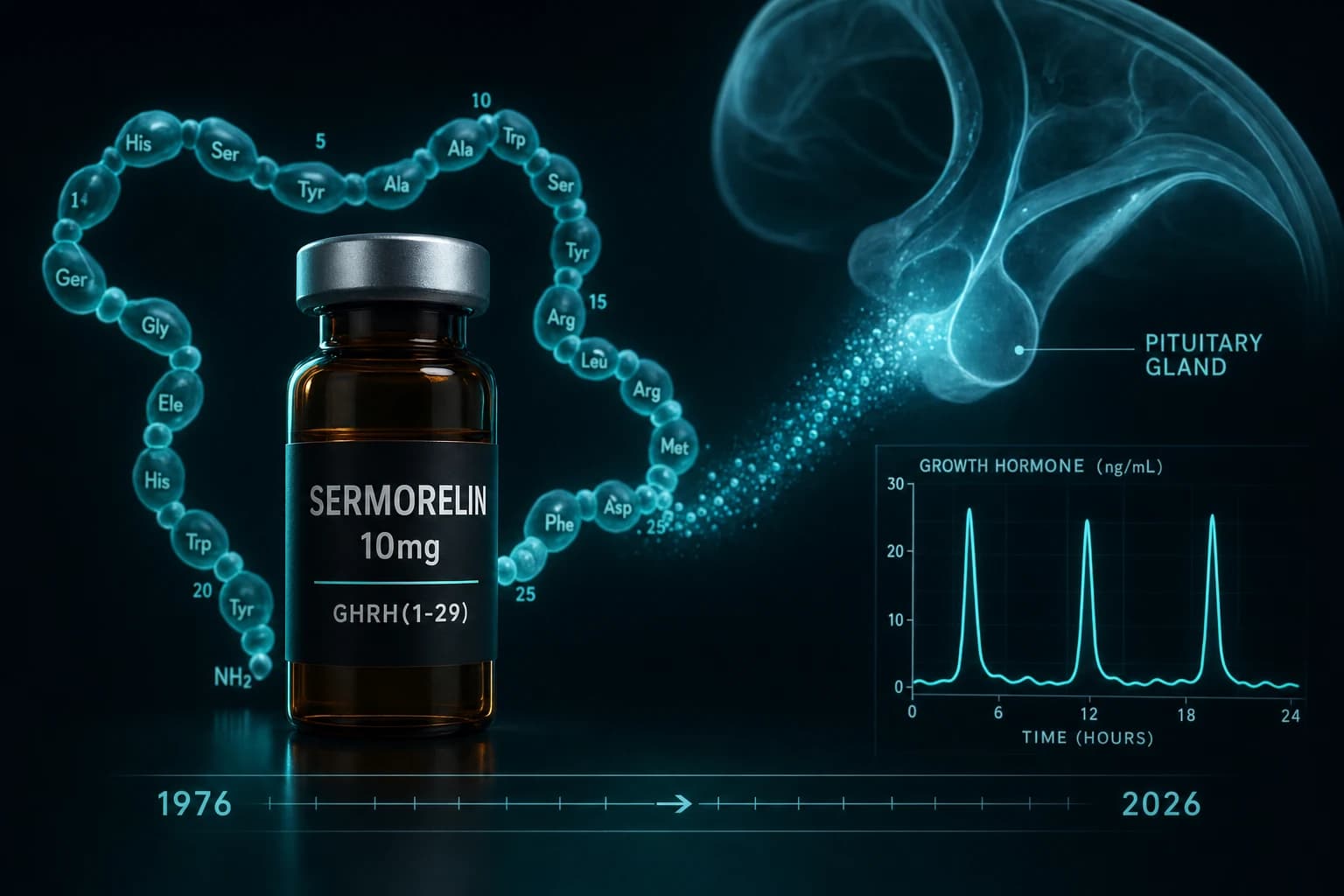
- Sermorelin is GHRH(1-29)NH2, the shortest fully active fragment of human GHRH
- Plasma half-life is roughly 11 to 12 minutes (Evans et al. 1993, PMID 8329825)
- Twice-daily 1 mg GHRH(1-29) restored 24-h GH and IGF-1 in old men over 14 days (Corpas et al. 1992, PMID 1379256)
- Geref earned FDA approval in 1997 for pediatric GHD; the manufacturer discontinued it in 2008 for commercial reasons, not safety
- Sermorelin remains compoundable under section 503A and has more direct adult human data than most modern GHRH analogs
A 29-amino-acid fragment, FDA-approved twice over, and now back through compounding
Sermorelin is the shortest fully active piece of human growth hormone-releasing hormone. Endogenous GHRH is 44 amino acids long. The first 29 carry essentially all of the receptor activity, which is why a 1980s synthesis project chose that fragment, capped it as an amide (GHRH(1-29)NH2), and turned it into a clinical drug. Geref reached FDA approval in 1997 for pediatric growth hormone deficiency, then was pulled by the manufacturer in 2008 for commercial reasons rather than safety concerns (FDA Federal Register 2013).
Most peptide content treats sermorelin as a faded predecessor to CJC-1295. That framing skips the part that matters for research: sermorelin has more direct adult human data, on more endpoints, across more independent labs, than any other GHRH analog in current circulation. The clinical record predates Reddit by 15 years.
This guide covers what three decades of GHRH(1-29) research actually show, where sermorelin sits next to CJC-1295 and tesamorelin, and what the literature does not establish.
What sermorelin is, in plain pharmacology
Sermorelin acetate is the acetate salt of GRF(1-29)NH2: tyrosine-alanine-aspartate-alanine-isoleucine-phenylalanine-threonine-asparagine-serine-tyrosine-arginine-lysine-valine-leucine-glycine-glutamine-leucine-serine-alanine-arginine-lysine-leucine-leucine-glutamine-aspartate-isoleucine-methionine-serine-arginine. The amide cap on the C-terminal arginine is required for full activity at the GHRH receptor.
The mechanism is the GHRH receptor pathway, not direct GH agonism. Sermorelin binds GHRHR on pituitary somatotrophs, activates Gs-coupled signaling, raises intracellular cAMP, and amplifies endogenous GH pulse amplitude. Because release stays under hypothalamic somatostatin control, the system retains negative feedback. That is the mechanistic reason sermorelin does not produce the supraphysiologic GH peaks that exogenous rhGH does (Walker 2006, PMID 18046908).
In practical terms: sermorelin asks the pituitary to do its native job. rhGH replaces the job entirely.
Pharmacokinetics: half-life is the central design constraint
The pharmacokinetic profile of GHRH(1-29)NH2 was characterized in healthy adults by Evans et al. 1993 (PMID 8329825). Maximal GH release in that study occurred at 1 to 2 mcg/kg intravenously. Plasma clearance was rapid, with serum levels falling near baseline within minutes of an IV bolus. Reported plasma half-life across subsequent literature converges on roughly 11 to 12 minutes.
That short half-life is the engineering problem the entire GHRH-analog field has been trying to solve since.
| Compound | Structure | Plasma half-life | Dosing context |
|---|---|---|---|
| Endogenous GHRH(1-44) | Native, 44 aa | ~7 minutes | Hypothalamic, pulsatile |
| Sermorelin (GHRH 1-29) | Native sequence, 29 aa, amide | ~11 to 12 minutes | Once or twice daily SC in published trials |
| Modified GRF (1-29) | Position 2/8/15/27 substitutions | ~30 minutes | Pre-CJC-1295 research analog |
| CJC-1295 (no DAC) | Same as modified GRF (1-29) | ~30 minutes | Functionally equivalent to modified GRF |
| CJC-1295 with DAC | Modified GRF plus DAC linker, albumin-bound | ~5 to 8 days | Once-weekly profile |
| Tesamorelin | N-terminal modification, 44 aa core | ~30 to 38 minutes (SC) | Daily SC, FDA-approved for HIV-LD |
Two implications fall out of this table.
First, sermorelin's short half-life is not a flaw. It is a feature for matching native pulsatility. The hypothalamus does not deliver GHRH continuously; it pulses every two to three hours. A short-acting analog given before sleep approximates the largest endogenous nocturnal pulse. CJC-1295 with DAC, by contrast, produces a sustained "bleed" that flattens the pulse architecture entirely. Whether that is clinically better is an open question, not a settled one.
Second, sermorelin requires more frequent administration than longer-acting analogs to reach equivalent cumulative GH exposure. The trade-off is fidelity to native physiology versus convenience.
Note: Half-life is measured in plasma. The downstream GH pulse from a single sermorelin dose can extend two to three hours past plasma clearance because pituitary signaling outlasts peptide presence. The Evans 1993 paper documented sustained GH elevation for about three hours after a 1 mcg/kg IV bolus despite rapid plasma elimination.
What human studies actually show
The adult human evidence for sermorelin and closely related GHRH(1-29) analogs is thin compared to a Phase 3 GLP-1 program but unusually rich for a peptide of this category. Four studies anchor the literature.
Corpas et al. 1992 (PMID 1379256). Ten healthy old men (mean age 68) received GHRH(1-29) at low dose (0.5 mg) and high dose (1 mg) subcutaneously twice daily for 14 days each, with an intervening 14-day washout, alongside nine young controls. The high-dose arm produced significant increases in 24-hour mean GH (p < 0.001), GH peak amplitude (p < 0.05), and IGF-1 (p < 0.005). The result is the cleanest demonstration that GHRH(1-29) administration alone (no rhGH, no co-stim with a ghrelin agonist) can reverse the biochemical somatotropic decline of aging in a dose-dependent way.
Vittone et al. 1997 (PMID 9005976). Single nightly subcutaneous GHRH(1-29) in healthy elderly men, longer duration. The endpoints expanded to include skeletal muscle bioenergetics and body composition (DEXA). The biochemical effects were present but the body-composition and muscle-function endpoints did not move significantly. The authors' own conclusion was that single nightly dosing is less effective than multiple daily doses for eliciting downstream GH and IGF-1 effects. That is a direct hit at the simplest "one shot at bedtime" protocol.
Khorram et al. 1997 (PMID 9141536). A closely related analog, [Nle27]GHRH(1-29)NH2 (a norleucine-for-methionine substitution at position 27 for stability), administered to age-advanced men and women over 16 weeks. The somatotropic axis activated reliably, with rises in GH, IGF-1, and IGFBP-3. This is not sermorelin per se. It is the structural lineage from which modified GRF (1-29), and downstream CJC-1295, evolved. The relevance is mechanistic continuity, not direct molecule-for-molecule equivalence.
Baker et al. 2012 (PMID 22869065). A 20-week double-blind randomized controlled trial in 137 completers (76 healthy, 61 with mild cognitive impairment) used tesamorelin, a different GHRH analog, not sermorelin. IGF-1 rose 117% and fasting insulin rose 35% within the normal range in MCI participants. Cognitive testing showed favorable effects on fluid intelligence (working memory, planning, processing speed). The relevance to sermorelin is class-level: the GHRH-analog mechanism produced cognitive signal at trial-grade rigor in an aging population, which is the same therapeutic frame sermorelin is most often used in. The caveat is the molecule was different and longer-acting.
| Study | Compound | Sample | Duration | Primary signal |
|---|---|---|---|---|
| Corpas et al. 1992 | GHRH(1-29) 0.5 and 1 mg SC BID | 10 old, 9 young | 14 days each dose | 24-h GH and IGF-1 rose dose-dependently |
| Vittone et al. 1997 | GHRH(1-29) SC nightly | Healthy elderly men | Several weeks | Biochemical signal, no body-comp change |
| Khorram et al. 1997 | [Nle27]GHRH(1-29)NH2 | Age-advanced men and women | 16 weeks | Somatotropic axis activated |
| Baker et al. 2012 | Tesamorelin (not sermorelin) | 137 older adults (61 MCI) | 20 weeks | Fluid intelligence improved, IGF-1 +117% |
Read literally: sermorelin and its near-relatives reliably raise GH and IGF-1 in older adults with declining baseline. Whether that translates to body-composition changes, lean-mass gains, or symptom-level improvements depends on dose frequency, duration, and the population studied. The 14-day Corpas window did not measure body composition. The Vittone work did and saw little. The Baker tesamorelin trial saw cognition, not strength.
Bottom line: The biochemical claim (raises GH and IGF-1) has 30 years of human data behind it. The downstream claim (improves muscle, body composition, sleep, or cognition in healthy adults) has weaker and more selective evidence and varies by analog, dose schedule, and population. Treat the two claims separately.
Where sermorelin sits next to CJC-1295 and tesamorelin
The three GHRH analogs in active research circulation are sermorelin, modified GRF (1-29) (often labeled CJC-1295 without DAC by retail vendors), and CJC-1295 with DAC. Tesamorelin sits adjacent as the FDA-approved analog for HIV-associated lipodystrophy.
| Axis | Sermorelin | CJC-1295 (no DAC) | CJC-1295 with DAC | Tesamorelin |
|---|---|---|---|---|
| Sequence | Native GHRH(1-29) | GHRH(1-29) with stability substitutions | Same as no-DAC plus DAC linker | Native GHRH(1-44) plus N-terminal modification |
| Half-life | ~11 to 12 min | ~30 min | ~5 to 8 days | ~30 to 38 min |
| GH pulse pattern | Sharp, transient, native-like | Slightly extended pulse | Continuous elevation, flattens pulses | Extended pulse, daily |
| FDA approval | Geref, 1997 (pediatric GHD), discontinued 2008 | None | None | EGRIFTA, 2010 (HIV-LD), reformulated as EGRIFTA SV 2019 |
| Adult human RCT data | Multiple older trials | Sparse | One Phase 1 PK trial | Multiple Phase 3 trials |
| 503A compounding status (2026) | Permitted | Restricted (Category 2 in 2023 FDA action) | Restricted | FDA-approved product |
| Best-supported use case | Native pulse approximation | Not well differentiated from sermorelin | Sustained GH elevation research | Visceral adiposity reduction |
Two non-obvious points fall out.
First, "CJC-1295 without DAC" and modified GRF (1-29) are functionally the same molecule. Vendors split them by name for marketing reasons. The PK is essentially identical.
Second, sermorelin is the only molecule in this class that has both native-physiology fidelity and a meaningful FDA approval history. Walker's 2006 review made this the central argument for its return: rhGH replacement skips the pituitary entirely, while sermorelin preserves the neuroendocrine architecture that decays first in aging (Walker 2006).
For protocol-level context on the modified GRF / CJC-1295 / ipamorelin family, the CJC-1295 + Ipamorelin Stack: Complete GH Research Protocol and the FIT Stack walk-through cover that side of the field. For the tesamorelin clinical record, the Tesamorelin visceral fat guide covers the HIV-LD trials and the off-label visceral adiposity literature.
Why sermorelin returned in the telehealth era
Geref left the U.S. market in 2008. By the late 2010s, compounding pharmacies operating under section 503A of the Federal Food, Drug, and Cosmetic Act began producing sermorelin acetate again under individual prescriptions. The September 2023 FDA reclassification of bulk peptide ingredients moved several compounds (BPC-157, CJC-1295, ipamorelin, thymosin beta-4) into Category 2, where 503A bulk compounding is effectively blocked. Sermorelin's pathway is more permissive because of its prior FDA-approved drug status, which kept it eligible for 503A compounding from a different regulatory route. That asymmetry is why telehealth platforms have leaned on sermorelin specifically.
The pull from the demand side is the broader GH-axis interest produced by GLP-1 awareness, longevity content, and Reddit-driven peptide curiosity. Sermorelin offers something CJC-1295 and ipamorelin no longer offer cleanly in a compliant pharmacy supply chain: legal compounding plus 30 years of human data plus a regulatory paper trail.
The honest framing is that sermorelin's renaissance is a regulatory accident, not a scientific breakthrough. The science was there in 1997. The supply chain caught up in 2023.
Safety signals from the literature
Reported adverse effects across sermorelin and GHRH(1-29) trials have been mild. Injection-site redness, mild headache, transient flushing, and infrequent nausea are the most commonly reported. The Walker 2006 review summarized the safety profile across the GHRH(1-29) literature as favorable, with no consistent signal for the metabolic or oncologic concerns that have shadowed long-term rhGH replacement.
Three structural reasons explain the cleaner profile. First, the negative feedback loop through somatostatin caps the maximum GH response, so supraphysiologic peaks are difficult to produce. Second, IGF-1 elevation through native pulsatile GH appears to track baseline regulation more closely than continuous rhGH exposure. Third, the dose ranges used in published research (typically 0.5 to 1 mg subcutaneous) sit far below the doses that produced GH receptor saturation in early dose-finding work.
That said, the safety database is small by modern standards. No long-duration safety study (24+ months, several thousand subjects) exists for sermorelin in non-GHD adults. Inferences about long-term oncologic, metabolic, or cardiovascular safety in healthy users are extrapolations, not data.
Warning: Sermorelin raises IGF-1. IGF-1 has been associated with cancer risk in some epidemiologic literature, particularly for prostate, colorectal, and breast cancers in observational cohorts. Whether sermorelin-driven IGF-1 elevation translates to that risk is unstudied. Researchers with personal or family histories of hormone-sensitive cancers should treat the GH/IGF-1 axis as an unresolved long-term safety question, not a settled one.
Honest limits of the evidence
Several gaps in the literature deserve attention before extrapolating to research planning.
- No large modern adult RCT. The published Corpas, Vittone, and related GHRH(1-29) trials are small (n in the single or low double digits) and dated. The Baker 2012 work is the most recent rigorous trial in the class, and it used tesamorelin, not sermorelin.
- No head-to-head against rhGH. Sermorelin versus rhGH on body-composition or symptom endpoints has not been tested in a powered randomized trial. The case for sermorelin over rhGH in non-deficient adults is mechanistic and regulatory, not evidence-based on hard endpoints.
- No head-to-head against modified GRF (1-29) plus ipamorelin. The most common contemporary GH-secretagogue protocol (modified GRF plus a ghrelin agonist like ipamorelin) has not been compared to sermorelin alone in a controlled trial.
- Sleep and recovery claims are largely inferential. Sermorelin raises GH pulse amplitude, GH supports slow-wave sleep, therefore sermorelin should improve deep sleep. The transitivity is reasonable, but direct polysomnography data on sermorelin in healthy adults is limited. The ghrelin-receptor-agonist literature (MK-677, ipamorelin) carries more direct sleep architecture data than sermorelin does.
- Dose-response is weakly characterized. Most published doses cluster at 0.5 to 1 mg subcutaneous per administration. Whether 200 mcg, 500 mcg, or 1 mg produces meaningfully different pulse amplitudes in healthy older adults is not well established outside of the Corpas low-versus-high comparison.
- Compounded product variability is unmeasured. The Phase 3 record was for branded Geref. The current compounded supply is not assayed in published peer-reviewed work for purity, content uniformity, or cold-chain stability. Researchers using compounded sermorelin are extrapolating from FDA-approved product data.
How researchers structure dosing in published protocols
Doses in the published trials are limited to a narrow band. None of these constitute a clinical recommendation; they describe what the literature has actually tested.
| Protocol context | Dose | Frequency | Source |
|---|---|---|---|
| Older men, biochemical endpoints | 0.5 to 1 mg SC | Twice daily, 14 days | Corpas et al. 1992 |
| Healthy elderly men, body comp | ~1 mg SC equivalent | Once nightly, several weeks | Vittone et al. 1997 |
| Pediatric GHD diagnostic | 1 mcg/kg IV | Single bolus | Geref labeling, Evans 1993 |
| Common compounding-pharmacy starting points (unverified by trial) | 100 to 500 mcg SC | Daily, before sleep | Provider-reported, not RCT |
The trial-grade doses are larger than most contemporary compounded prescriptions for non-GHD adults, and the trial frequency was higher (twice daily in the cleanest positive trial). The implication is that single-evening 200 mcg protocols common in telehealth practice sit below the doses used in the published efficacy literature. Whether that reflects clinical conservatism, dose-response flattening at lower exposures, or cost-driven minimums is not established.
For reconstitution math (bacteriostatic water volume, units to draw, mcg per click), the reconstitution calculator and the reconstitution complete guide cover the standard work. Sermorelin acetate is typically supplied as 2 to 5 mg lyophilized powder per vial.
Sermorelin in the broader GH-axis research stack
Several contiguous questions sit alongside sermorelin in the literature.
- Whether sermorelin pairs additively with a ghrelin-receptor agonist (ipamorelin, hexarelin) in the way modified GRF (1-29) plus ipamorelin does. Mechanistically yes, with two complementary release pathways. Direct human RCT evidence: limited.
- Whether sermorelin can substitute functionally for rhGH in adult-onset GHD. The Walker 2006 argument was yes. The regulatory record never tested it formally; Geref's adult indication was withdrawn before this question matured.
- Whether modified GRF / CJC-1295 (no DAC) provides any meaningful advantage over sermorelin in pulse-fidelity protocols. PK is longer, but pulse architecture is less native. The literature has not resolved the trade-off.
- Whether MK-677 (ibutamoren) achieves comparable IGF-1 elevation through the orally available ghrelin-receptor route. The MK-677 oral GH secretagogue guide covers that side, including the trade-offs around appetite and cortisol that sermorelin does not share.
A research-grade decision frame
The decision between sermorelin and the longer-acting alternatives is not "stronger versus weaker." It is a bet about pulse fidelity versus convenience, with regulatory accessibility as a third axis.
| If the priority is | Sermorelin makes more sense | A longer-acting analog makes more sense |
|---|---|---|
| Native pulse architecture | Yes, half-life maps to pulse interval | No, sustained elevation flattens pulses |
| Once-weekly dosing | No, requires daily or twice-daily SC | CJC-1295 with DAC fits this |
| Visceral fat reduction with FDA evidence | No direct evidence | Tesamorelin, EGRIFTA SV |
| 503A-compliant compounding access in 2026 | Sermorelin is permitted | CJC-1295 / ipamorelin restricted post-2023 |
| Largest body of human RCT data | Sermorelin and tesamorelin | CJC-1295 has minimal direct trial data |
| Cleanest cognition signal in older adults | Tesamorelin (Baker 2012) | Sermorelin literature is biochemical-heavy |
The framing this table is built around is what evidence and what regulatory pathway exist, not vendor marketing.
Sourcing for research-grade sermorelin
For research applications, vial-grade sermorelin and adjacent GHRH analogs are available from Ascension Peptides with the ENHANCED code at 50% off. Reconstitution accuracy and cold-chain handling determine whether the pulse-amplitude expectations from the trial literature are reproducible in a structured protocol. The reconstitution calculator covers the volume math, and the injectable vs oral peptide bioavailability guide addresses why subcutaneous dosing is the published route for this class.
For oral GH-secretagogue alternatives in the ghrelin-receptor lane (MK-677), Limitless Biotech ships oral capsules under code ENHANCED. Note that MK-677 and sermorelin work through different receptor pathways and produce different downstream profiles; they are complements in the literature, not substitutes.
Bottom line
Bottom line: Sermorelin's claim to relevance is not novelty. It is the depth of human data behind a 29-amino-acid fragment that has been studied for 30 years and reached FDA approval once. The biochemical effect (raises GH and IGF-1 in adults with declining baseline) is well documented. The downstream effects (body composition, cognition, sleep, recovery) carry weaker direct evidence and depend heavily on dose schedule, duration, and population. The current compounding access is a regulatory fact, not a scientific verdict.
The most defensible reading is that sermorelin is the GHRH analog with the highest evidence-to-marketing ratio in current circulation. That is faint praise in a class where most marketing outruns data, and meaningful praise compared to the alternatives.
Related research on this site
- CJC-1295 + Ipamorelin Stack: The Complete GH Research Protocol
- The FIT Stack: CJC-1295 + Ipamorelin GH Protocol
- Tesamorelin: Visceral Fat GHRH Peptide Guide
- MK-677 (Ibutamoren): Oral GH Secretagogue Guide
- Peptide Reconstitution: The Complete Guide
- Injectable vs Oral Peptides: Bioavailability Guide
- Sermorelin research page
- Reconstitution Calculator
This article is for educational and research purposes only. It is not medical advice. Sermorelin (Geref) was FDA-approved in 1997 for pediatric growth hormone deficiency and discontinued in 2008 by the manufacturer for commercial reasons. Sermorelin is currently available only through 503A compounding under individual prescription; the compounded product is not FDA-reviewed for safety, effectiveness, or quality as a finished product. Use in adults outside of diagnosed growth hormone deficiency is off-label and not supported by current FDA-approved labeling. Doses, frequencies, and durations summarized here describe what the published clinical literature tested; they are not protocols and do not establish efficacy or safety for any specific individual. The IGF-1 axis carries unresolved long-term safety questions, particularly around cancer epidemiology, that are not addressed by the short-duration trials reviewed here.


