At a glance
- Eloralintide Phase 2 (Billings et al. Lancet 2025, PMID 41207310) produced 9.5% to 20.1% mean weight loss at 48 weeks vs 0.4% on placebo across 263 adults
- The molecule activates the amylin 1 receptor about 12 times more potently than the calcitonin receptor, unlike older amylin analogs (Bhattachar et al. DOM 2026, PMID 41559929)
- Once-weekly subcutaneous with a half-life of approximately two weeks, supporting steady-state weekly dosing
- Phase 3 ENLIGHTEN program is enrolling in obesity, OSA, and knee osteoarthritis, with first reads expected 2027
- Lilly is testing eloralintide as monotherapy and as an add-on to tirzepatide; FDA approval is unlikely before 2028
Lilly's selective amylin agonist eloralintide produced 20.1% mean weight loss at 48 weeks in its Phase 2 trial, the highest published number for any amylin monotherapy and within striking distance of tirzepatide on a much shorter timeline. The Phase 1 proof-of-concept paper appeared in Diabetes, Obesity and Metabolism in early 2026, the Phase 2 read landed in The Lancet at ObesityWeek 2025, and Phase 3 enrollment started in December 2025 under the ENLIGHTEN program.
This article covers what eloralintide is, the Phase 1 and Phase 2 data, how it compares to other amylin candidates and to the GLP-1 class, the Phase 3 program design, and what remains unknown going into 2027 readouts.
What eloralintide is
Eloralintide (Lilly's LY3841136) is a long-acting selective amylin receptor agonist designed to suppress appetite through the same brainstem circuit that endogenous amylin uses. It is an amylin analog conjugated to a C20 fatty diacid for reversible albumin binding, which gives it a half-life of roughly two weeks and supports once-weekly subcutaneous dosing.
The structural feature that distinguishes eloralintide from older amylin work is receptor selectivity. The molecule activates the human amylin 1 receptor (AMY1R) about 12 times more potently than it activates the calcitonin receptor (Bhattachar et al., Diabetes Obesity Metabolism 2026, PMID 41559929). Pramlintide, the legacy amylin analog approved for type 1 diabetes in 2005, has roughly equal affinity for amylin and calcitonin receptors and a half-life under one hour. The combination of long half-life and AMY1R selectivity is the central pharmacology bet behind the program.
Bottom line: Eloralintide is a selective AMY1R agonist with a two-week half-life, dosed once weekly. It is structurally and pharmacologically distinct from cagrilintide and from pramlintide.
How amylin works (and why Lilly is investing here)
Amylin is a 37-amino-acid peptide co-secreted with insulin from pancreatic beta cells in response to meals. Endogenous amylin slows gastric emptying, suppresses postprandial glucagon, and acts on the area postrema in the brainstem to drive satiety. The amylin receptor is a heterodimer of the calcitonin receptor and a receptor activity-modifying protein (RAMP), with three subtypes (AMY1R, AMY2R, AMY3R) defined by which RAMP is associated (Larsen, Curr Drug Targets 2025, PMID 40910290).
Amylin's satiety pathway is distinct from GLP-1's. GLP-1 receptor activation suppresses appetite primarily through nucleus tractus solitarius neurons and vagal afferents. Amylin receptor activation works through area postrema neurons projecting to the hypothalamus, with downstream activation of POMC and inhibition of NPY/AgRP. When both pathways are engaged in parallel, the weight loss effect is additive, which is the structural reason that CagriSema (cagrilintide + semaglutide) produces more weight loss than semaglutide alone. The full pipeline view is in our GLP-1 + amylin combination pipeline 2026 guide.
Lilly's bet with eloralintide is that an AMY1R-selective long-acting analog can produce meaningful weight loss as monotherapy with a gentler GI profile than GLP-1 monotherapy, and that combining it with tirzepatide can push total weight loss higher without compounding GI side effects.
Phase 1 proof of concept (Bhattachar et al. DOM 2026)
The Phase 1 multiple-ascending-dose study evaluated 100 participants with obesity or overweight (mean BMI 32.6, 29% female) over 12 weeks at three US sites (Bhattachar et al., Diabetes Obesity Metabolism 2026, PMID 41559929). Five ascending-dose cohorts received once-weekly subcutaneous eloralintide or placebo. The primary endpoints were safety, tolerability, and pharmacokinetics; weight change was a secondary signal.
Key findings:
- Half-life of approximately two weeks, supporting once-weekly dosing with low peak-to-trough variability
- Dose-dependent weight loss at 12 weeks, with the highest cohort separating cleanly from placebo
- Gastrointestinal adverse events were less frequent than the rates typically reported for GLP-1 monotherapy at comparable weight-loss windows
- No serious safety signals; the adverse event profile supported advancing to Phase 2
The Phase 1 data alone would not be a story. What set up the Phase 2 program design was the mechanistic context: a selective AMY1R agonist with a two-week half-life producing a clean weight signal without the GI burden that defines the GLP-1 class.
Phase 2 trial results (Billings et al. Lancet 2025)
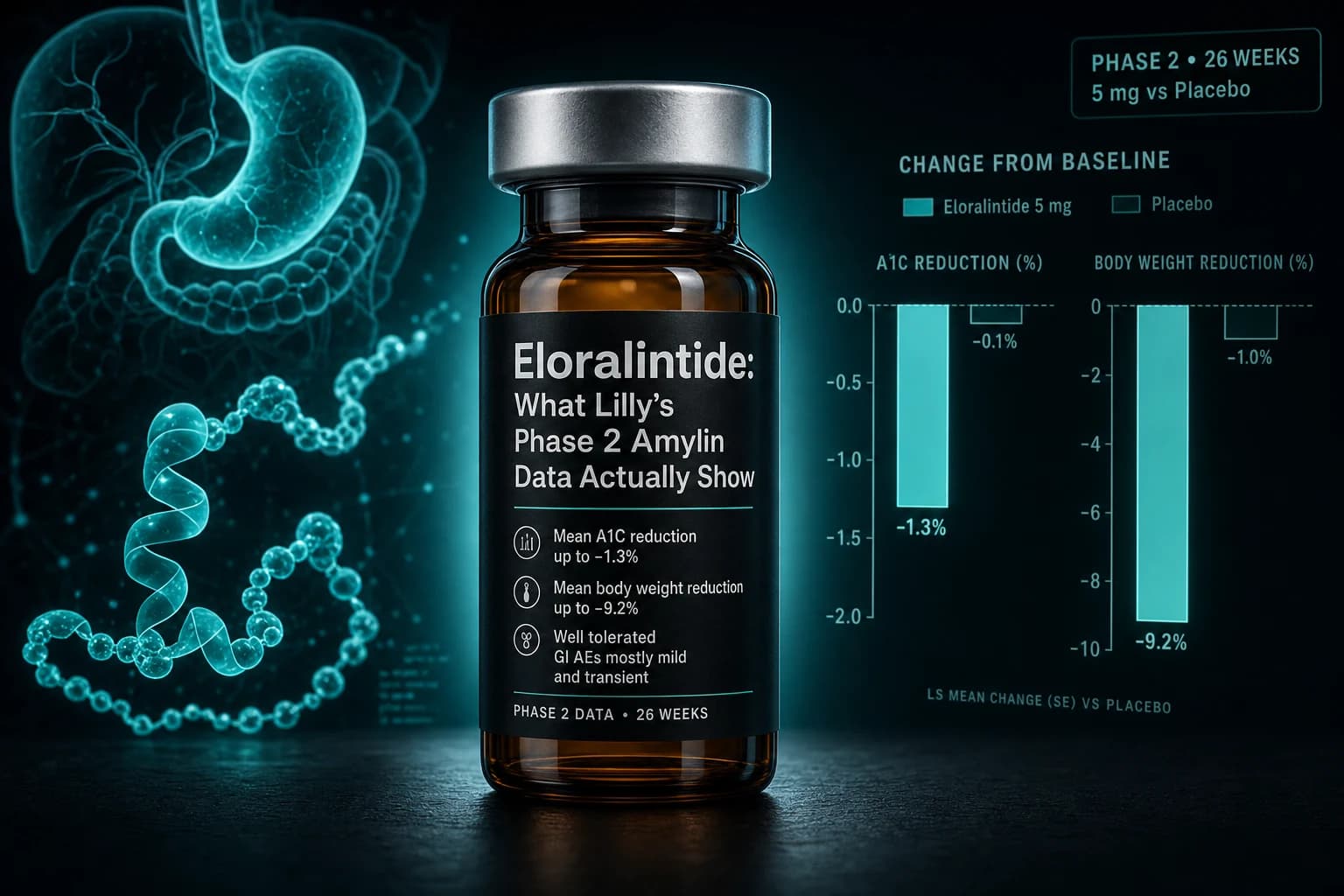
The Phase 2 trial randomized 263 adults with overweight or obesity and at least one obesity-related comorbidity, without type 2 diabetes, across 46 US sites (Billings et al., Lancet 2025, PMID 41207310). Mean baseline characteristics: 78% female, mean age 49, mean BMI in the high 30s. Participants received once-weekly subcutaneous placebo or eloralintide at 1 mg, 3 mg, 6 mg, 9 mg, or one of two dose-escalation regimens, for 48 weeks. Results were presented at ObesityWeek 2025 and simultaneously published in The Lancet.
Weight change at 48 weeks
| Arm | Mean weight change (efficacy estimand) |
|---|---|
| Placebo | -0.4% |
| Eloralintide 1 mg | -9.0% |
| Eloralintide 3 mg | -12% |
| Eloralintide 6 mg | -18% |
| Eloralintide 9 mg | -20.1% |
| Escalation arms | -16% to -20% |
Every active arm met the primary endpoint of superiority to placebo. The 9 mg dose produced 20.1% mean weight loss, the highest result for any amylin monotherapy in any published trial.
For context, semaglutide 2.4 mg in STEP 1 produced 14.9% at 68 weeks. Tirzepatide 15 mg in SURMOUNT-1 produced 22.5% at 72 weeks. Eloralintide 9 mg matches the semaglutide result on a shorter timeline and approaches tirzepatide on a much shorter timeline, suggesting the dose-response curve has not yet flattened.
Cardiometabolic markers
Treatment was associated with improvements across waist circumference, systolic blood pressure, lipid profile, glycemic markers, and high-sensitivity CRP. The cardiometabolic profile mirrored what GLP-1 trials produce at similar weight-loss magnitudes, consistent with weight loss being the primary driver rather than a unique amylin effect on those endpoints.
Tolerability
The most common adverse events were mild-to-moderate nausea and fatigue, with frequency increasing at higher doses. Discontinuation rates due to adverse events were not headline-driving, and the GI profile was reported as more favorable than expected for the weight loss magnitude. A direct read against published GLP-1 monotherapy GI rates is not possible without a head-to-head trial, but the Phase 2 pattern matches the working hypothesis that amylin agonism produces less GI burden per unit weight loss than GLP-1 agonism.
Bottom line: Phase 2 hit 20.1% weight loss at 48 weeks on 9 mg, the highest published amylin monotherapy result. GI tolerability looked favorable for the weight loss magnitude. Phase 3 will determine whether both findings hold at scale.
Eloralintide vs the other amylin candidates
Three amylin-targeted compounds are in late-stage development as of mid-2026. Each makes a different bet on receptor selectivity, half-life, and combination strategy.
| Compound | Sponsor | Selectivity | Half-life | Top Phase 2 weight loss | Status |
|---|---|---|---|---|---|
| Cagrilintide | Novo Nordisk | Dual AMY / calcitonin | ~7 days | ~10% at 26 wk monotherapy | CagriSema combo filed |
| Petrelintide | Zealand / Roche | Amylin-selective | ~7 days | -10.7% at 42 wk | Phase 3 announced April 2026 |
| Eloralintide | Eli Lilly | AMY1R-selective (12x) | ~14 days | -20.1% at 48 wk | Phase 3 enrolling (ENLIGHTEN) |
A few honest observations on this comparison:
Cross-trial Phase 2 numbers are not directly comparable. Different populations, durations, dose ladders, and estimands. The 20.1% number for eloralintide 9 mg is genuinely high for amylin monotherapy, but petrelintide and cagrilintide were not tested at equivalent dose intensities for equivalent durations. The original cagrilintide dose-finding work in 706 adults produced approximately 10.8% weight loss on 4.5 mg at 26 weeks (Lau et al., Lancet 2021, PMID 34798060), which is the closest historical benchmark for amylin monotherapy.
The two-week half-life is a meaningful distinction. Both petrelintide and cagrilintide are weekly with shorter half-lives. Eloralintide's longer half-life is what makes Lilly's combination strategy with tirzepatide cleaner: similar half-lives means a single weekly injection can sit in steady state without one component clearing before the next dose.
The selectivity claim matters mechanistically but the clinical translation is unproven. AMY1R selectivity should in principle reduce off-target activity at calcitonin receptors, which could affect bone or calcium handling. Neither the Phase 1 nor Phase 2 trials reported signals on those endpoints, but those are not the trials designed to find them.
For the unimolecular GLP-1+amylin alternative, see our amycretin Phase 1 evidence article. For the cagrilintide-semaglutide combination context, see the CagriSema REDEFINE Phase 3 guide.
Eloralintide vs GLP-1 and dual agonists
Cross-trial efficacy comparisons should always carry a warning, but the rough picture matters for understanding where eloralintide sits relative to the established class.
| Drug | Class | Top published weight loss | Trial | Duration |
|---|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 | -14.9% | STEP 1 | 68 wk |
| Tirzepatide 15 mg | GIP + GLP-1 | -22.5% | SURMOUNT-1 | 72 wk |
| Retatrutide 12 mg | GIP + GLP-1 + glucagon | up to ~30% | TRIUMPH-1 Phase 3 | 80 wk |
| CagriSema 2.4/2.4 mg | GLP-1 + amylin | -22.7% | REDEFINE 1 | 68 wk |
| Eloralintide 9 mg | Amylin monotherapy | -20.1% | Phase 2 | 48 wk |
| Petrelintide top dose | Amylin monotherapy | -10.7% | ZUPREME-1 | 42 wk |
Eloralintide as monotherapy produces weight loss in the same ballpark as injectable semaglutide and approaching the dual and triple agonists on shorter timelines. For most of the obesity field this is the surprising part of the Phase 2 read. The class historical record (pramlintide as a thrice-daily insulin adjunct produced about 6 kg over 12 months in obese non-diabetic adults, Smith et al., Diabetes Care 2008, PMID 18753666) bounded expectations for amylin monotherapy in the high single digits. Eloralintide breaks that ceiling.
What the comparison does not address: tolerability cost per percentage point, durability after discontinuation, long-term safety, and population-scale variability. Multi-agonists carry GLP-1 GI burden; eloralintide is the only candidate in this comparison without a GLP-1 component, which is the entire reason its tolerability story matters. The retatrutide TRIUMPH-1 article covers the triple agonist Phase 3 data, the tirzepatide vs semaglutide SURMOUNT-5 head-to-head covers the GLP-1 vs GIP+GLP-1 comparison, and the orforglipron Phase 3 evidence covers the oral GLP-1 monotherapy benchmark. Our GLP-1 dosing comparison 2026 holds the full dose-response context.
The ENLIGHTEN Phase 3 program
Lilly began enrolling Phase 3 studies in December 2025 under the ENLIGHTEN program. The trials test eloralintide across multiple populations:
| Trial | Indication | Design notes |
|---|---|---|
| ENLIGHTEN obesity | Obesity, monotherapy | Multi-dose vs placebo, large randomized double-blind |
| ENLIGHTEN-4 | Obesity + knee osteoarthritis pain | Master protocol, weight loss + OA pain endpoints |
| ENLIGHTEN-6 | Persistent obesity on weekly incretin | Add-on to tirzepatide arm |
| OSA program | Obstructive sleep apnea + obesity | Pre-specified AHI endpoint |
The OA and OSA Phase 3 trials are doing the same thing the SURMOUNT-OA and SURMOUNT-OSA trials did for tirzepatide: building indication-specific labels alongside the obesity indication, which improves payer coverage and broadens the prescribing population. The combination-with-tirzepatide arm is the most consequential strategically. If eloralintide + tirzepatide produces meaningful additional weight loss over tirzepatide monotherapy with manageable tolerability, Lilly would have a multi-mechanism in-house combination that competes directly with CagriSema without depending on semaglutide.
Note: Phase 3 readouts are not expected before late 2027. FDA approval, if Phase 3 succeeds, would land no earlier than 2028.
What is still unknown
Five open questions through 2027:
-
Does the 20.1% number hold at scale? Phase 3 sample sizes are much larger than 263 participants. Placebo response, dropout rate, and the full distribution of outcomes will all influence the registrational number. A drop of 1 to 3 percentage points from Phase 2 to Phase 3 is common in obesity drug development.
-
Does the tolerability story survive larger populations? Phase 2 reported a favorable GI profile, but Phase 3 with thousands of patients on multiple doses for 72+ weeks will determine whether the Phase 2 read holds. If yes, that is the defining advantage of the class.
-
How does the add-on-to-tirzepatide arm perform? This is the most strategically important arm. If eloralintide adds 5 to 7 percentage points to tirzepatide 15 mg with acceptable tolerability, Lilly has a CagriSema-class combination built entirely on in-house molecules.
-
What does discontinuation look like? GLP-1 discontinuation produces meaningful weight regain in most patients within a year. Amylin's claimed restoration of leptin sensitivity should theoretically translate to better off-treatment durability, but no published trial has tested this directly. The stopping GLP-1 weight regain research covers the GLP-1 baseline.
-
Where do bone and calcium endpoints land? AMY1R selectivity should reduce calcitonin-mediated off-target activity, but the trials that would surface bone density signals over multiple years have not been run. The GLP-1 bone density and fracture risk research is the closest analog for understanding why this matters for weight-loss drug labeling.
Sourcing notes
Eloralintide is not available as a research-grade compound as of May 2026. It is in active Lilly clinical development with sponsor exclusivity, and no research peptide vendor produces or distributes it.
Researchers working with the closest available compound in the amylin class can source injectable cagrilintide from Ascension Peptides with public per-batch COAs and 50% off using code ENHANCED. For GLP-1 comparison work, semaglutide and tirzepatide are also available from Ascension with the same code.
FAQ
How does eloralintide compare to semaglutide?
At 48 weeks, eloralintide 9 mg produced 20.1% mean weight loss in Phase 2. Semaglutide 2.4 mg in STEP 1 produced 14.9% at 68 weeks. Cross-trial comparisons should be read with caution, but eloralintide as monotherapy produced more weight loss than semaglutide on a shorter timeline and operates through a different receptor pathway. It does not engage the GLP-1 receptor, so it does not carry the GLP-1 class GI tolerability profile.
Is eloralintide approved by the FDA?
No. As of May 2026, eloralintide is in Phase 3 enrollment under the ENLIGHTEN program. FDA approval, if Phase 3 succeeds, is unlikely before 2028. Lilly has not announced a regulatory submission timeline.
What is the difference between eloralintide and cagrilintide?
Both target amylin receptors. Cagrilintide has roughly equal affinity for amylin and calcitonin receptors and a half-life of approximately one week. Eloralintide is about 12 times more selective for AMY1R over the calcitonin receptor and has a half-life of approximately two weeks. Cagrilintide is filed as part of CagriSema (cagrilintide + semaglutide). Eloralintide is being developed as monotherapy and as an add-on to tirzepatide.
Can eloralintide be combined with tirzepatide?
Lilly is running a Phase 3 add-on study (ENLIGHTEN-6) testing eloralintide in adults with persistent obesity on a weekly incretin. If results show meaningful additional weight loss over tirzepatide monotherapy without compounding GI side effects, the combination would compete with CagriSema for the top of the weight-loss class. Results are not expected before 2027.
Does eloralintide cause nausea?
The Phase 2 trial reported nausea and fatigue as the most common adverse events, generally mild to moderate and dose-dependent. The rate appeared lower than GLP-1 monotherapy at comparable weight-loss magnitudes, but no head-to-head trial has been published. Phase 3 will determine whether the Phase 2 tolerability holds at scale.
This article is for educational and research purposes only. It summarizes Phase 1 and Phase 2 clinical trial data and pre-clinical pharmacology for an investigational compound. Eloralintide (LY3841136) is not FDA-approved, not EMA-approved, and not available outside of clinical trials as of May 2026. Trial results described here reflect what was measured under controlled conditions and do not establish efficacy or safety for any individual outside of those trials. Long-term safety, durability after discontinuation, and outcomes in populations excluded from Phase 2 (active type 2 diabetes, severe psychiatric illness, pregnancy) are not yet characterized. Doses described here are what the published literature tested, not protocols or recommendations.