At a glance
- Tissue NAD+ drops ~50% between ages 40 and 60
- Subcutaneous NAD+ achieves 70-85% bioavailability vs 10-20% oral
- Start at 50 mg SC 2-3x/week; titrate to 100-300 mg over 2-3 weeks
- Inject slowly to minimize flushing, head pressure, and chest tightness
- NAD+ fuels sirtuins (longevity) and PARP-1 (DNA repair) simultaneously
Why NAD+ (and not NMN or NR)
Nicotinamide adenine dinucleotide (NAD+) is the central coenzyme in cellular energy metabolism and a direct substrate for the sirtuin family of longevity enzymes. Every cell in the body uses it, and levels decline measurably with age.
The longevity research community has spent the last decade arguing over the right way to restore it. The three main options:
- NAD+ itself: the finished molecule, administered directly (IV, IM, SC, or oral)
- NMN (nicotinamide mononucleotide): one step upstream, orally bioavailable, converts to NAD+ intracellularly
- NR (nicotinamide riboside): two steps upstream, orally bioavailable, converts to NMN then NAD+
The precursor argument (NMN, NR) is that they're cheaper, orally stable, and the body handles the final conversion. The direct NAD+ argument, favored in the research protocols of Sinclair, Attia, and popularized by Huberman's commentary, is that injected NAD+ raises tissue NAD+ levels faster and more reliably than precursors, especially in tissues where the upstream conversion pathway is rate-limited.
The pharmacokinetic data supports this hierarchy. Oral NAD+ has only 10-20% bioavailability because of its large molecular size and instability in the GI tract. Oral precursors perform better but still face hepatic first-pass metabolism and variable gut absorption. A head-to-head crossover study from Norwegian researchers (Nature Metabolism, 2025) found that NR produced roughly 2.3x greater blood NAD+ increases than NMN at equivalent gram doses, though both remain indirect routes. By contrast, subcutaneous NAD+ injection achieves 70-85% bioavailability by bypassing the gut entirely, with peak plasma levels at 2-4 hours post-injection and a sustained-release depot effect over 4-6 hours. IV infusion reaches 100% bioavailability by definition, but the subcutaneous depot avoids the sharp plasma spike that may trigger CD38 upregulation (a tolerance mechanism identified by Camacho-Pereira et al., Cell Metabolism, 2016).
For context on the precursor comparison: a study of NMN supplementation (250 mg/day) in 42 healthy older men showed a sixfold increase in whole-blood NAD+ levels. NR at similar doses raised blood NAD+ up to 2.7-fold in some individuals. These are meaningful increases, but they still depend on intact intracellular conversion enzymes (NMNAT1/2/3 for NMN; NRK1/2 for NR). Direct NAD+ injection sidesteps this conversion bottleneck entirely.
Injectable NAD+ is the most direct repletion method. The tradeoff is that it stings more than any other peptide in common research use, and injection-site sensitivity during the push is real.
What NAD+ actually does
NAD+ is not a peptide in the technical sense (it is a dinucleotide coenzyme), but it's routinely grouped with research peptides because it's lyophilized, reconstituted the same way, and injected subcutaneously by the same community.
Its functions fall into three buckets:
1. Mitochondrial energy production
NAD+ is the electron acceptor in the Krebs cycle. Every ATP molecule produced through oxidative phosphorylation requires NAD+ as a cofactor. Low NAD+ means constrained ATP production, which shows up as fatigue, reduced exercise capacity, and slower recovery.
2. Sirtuin activation
The sirtuin family (SIRT1 through SIRT7) are NAD+-dependent deacetylases. They regulate DNA repair, stress response, metabolic adaptation, and (in the longevity literature) lifespan extension. The enzymatic mechanism is specific: sirtuins use NAD+ as a cosubstrate to remove acetyl groups from lysine residues on target proteins, yielding the deacetylated substrate plus nicotinamide and O-acetyl-ADP-ribose as byproducts. Critically, SIRT1's Km for NAD+ falls within the range of normal physiological NAD+ fluctuations (Canto et al., Cell Metabolism, 2012), meaning even modest declines in cellular NAD+ can measurably suppress sirtuin activity. This is why the longevity community describes SIRT1 as a "metabolic sensor." When NAD+ drops, SIRT1 senses it immediately, and downstream targets like PGC-1alpha (mitochondrial biogenesis), FOXO3 (stress resistance), and NF-kB (inflammation) all lose their deacetylation-dependent regulation.
3. PARP-mediated DNA repair
PARP-1 is the dominant NAD+ consumer in the DNA repair pathway. When it binds damaged DNA, it catalyzes the transfer of ADP-ribose units from NAD+ onto acceptor proteins, building branched poly(ADP-ribose) chains that recruit repair machinery. The problem: under high oxidative stress or accumulated DNA damage (both of which increase with age), PARP-1 can consume NAD+ so aggressively that it depletes the pool available for sirtuins. This creates a direct competition. A 2011 study (Bai et al., Cell Metabolism) demonstrated that PARP-1 inhibition increased NAD+ availability enough to activate SIRT1 and improve mitochondrial function in mice. Conversely, SIRT1 can physically bind and deacetylate PARP-1 to suppress its activity (Rajamohan et al., Molecular Cell, 2009). The two enzymes are locked in a tug-of-war over the same NAD+ substrate.
Restoring NAD+ is essentially putting fuel back into three parallel systems that all ran lower than they should. The SIRT1/PARP-1 competition makes the case particularly compelling: repletion does not just add to one pathway; it relieves the zero-sum constraint between repair and longevity signaling.
Age-related decline
NAD+ levels drop measurably with age. The specific numbers vary by tissue and measurement method, but the published data is now detailed enough to break down by organ. Massudi et al. (2012, PLOS ONE) measured NAD+ in human skin biopsies and found concentrations dropped by approximately 50% between ages 40 and 60, the most-cited figure in the NAD+ aging literature. Human liver samples from patients over 60 showed roughly a 30% decline compared to patients under 45 (Zhu et al., 2015). Two MRI-based studies using 31P magnetic resonance spectroscopy found NAD+ declined 10-25% in human brains between young adulthood and old age. Skeletal muscle data shows 15-65% decline depending on species and model, with a narrower human-extrapolated range of 20-40%. A 2022 Frontiers in Endocrinology study measuring whole-blood NAD+ across 85 human subjects confirmed the age-associated decline, with concentrations severalfold lower in older adults compared to newborns.
The rough consensus: tissue NAD+ at age 20 is approximately 2x higher than at age 60, with the decline accelerating after 40. The mechanism is not just reduced synthesis. Camacho-Pereira et al. (Cell Metabolism, 2016) identified CD38, a NAD+-consuming enzyme, as a primary driver. CD38 expression increases with age and chronic inflammation, actively destroying NAD+ rather than merely failing to produce it. This "destruction" model explains why the decline accelerates with metabolic stress, chronic inflammation, and sleep disruption.
This is the core rationale for repletion: restore levels toward youthful baselines and restore the downstream signaling that depended on those levels. Whether this translates into extended lifespan in humans is unanswered. Whether it translates into measurable improvements in energy, recovery, and subjective "metabolic health" is increasingly supported by clinical data. A 2025 randomized trial (Qualia NAD+ study, ages 35-76) found 28 days of supplementation increased whole-blood NAD+ by 67% versus 4% with placebo.
Injection dosing
Published and research-community protocols for subcutaneous NAD+:
- Starting dose: 50-100 mg SC, 2-3 times weekly
- Titration: Increase to 150-200 mg over 2-3 weeks if well tolerated
- Maintenance: 100-300 mg SC, 1-3 times weekly
- Maximum typical research dose: 300 mg per injection
The range is wide because tolerance varies significantly. Some researchers run 100 mg 3x/week indefinitely; others push to 300 mg 2x/week for more aggressive repletion. IV NAD+ protocols (in clinic settings) commonly run 500-1000 mg per session, but the subcutaneous route does not tolerate those volumes. Clinical compounding protocols (Empower Pharmacy, Olympia Pharmacy) typically start patients at 20 mg SC and ramp to 100 mg over several weeks, with a common ceiling of 300 mg per week total. Loading protocols for acute repletion may use 100-200 mg daily for seven to ten days before stepping down to maintenance frequency.
Start low
Unlike most research peptides, the standard advice is to start lower than you think you need. NAD+ has dose-dependent side effects (below) that are unpleasant enough to abandon the protocol if you push too fast. Starting at 50 mg and titrating over 2-3 weeks gives the body time to adapt.
Reconstitution math
A 1000 mg NAD+ vial is the standard size from the verified partner:
- 1000 mg vial + 10 mL BAC water = 100 mg/mL
- 100 mg dose: 1.0 mL = 100 units on a U-100 syringe
- 200 mg dose: 2.0 mL = 200 units (two draws)
- 300 mg dose: 3.0 mL = 300 units (three draws)
The 10 mL water volume is larger than most peptides because of the higher mass per dose. If you prefer smaller injection volumes, 1000 mg + 5 mL BAC water = 200 mg/mL, but higher concentration = more sting on injection.
For smaller doses, 1000 mg + 20 mL BAC water = 50 mg/mL gives the most comfortable injection experience:
- 100 mg dose: 2.0 mL
- 200 mg dose: 4.0 mL
Verify any combination in the reconstitution calculator.
Side effects (and how to manage them)
NAD+ has a distinctive side effect profile unlike any other injectable in the research peptide space. The overall safety record is favorable (no serious adverse events have been reported in published NAD+ supplementation studies), but the acute sensations during and immediately after injection are more pronounced than typical peptides. Most researchers describe it as "unpleasant but brief."
The common three
- Flushing: face and upper body warmth/redness, typically starts 30-60 seconds into the injection, lasts 5-10 minutes post-injection
- Head pressure: a dense, full-head sensation that can feel alarming the first time, resolves within 15-30 minutes
- Chest tightness: transient, unrelated to cardiac effects, resolves with the head pressure
All three are dose-dependent and almost entirely caused by pushing the injection too fast. NAD+ needs to go in slowly. A 1-2 mL SC injection that would normally take 5 seconds should take 30-60 seconds for NAD+. IV clinics report the same pattern: when NAD+ is infused too rapidly, nausea, flushing, and cramping spike. Experienced clinics use 2-4 hour slow drips instead of rapid pushes, and the subcutaneous equivalent is the same principle applied at smaller volumes. With a slower injection rate, the NAD+ enters the subcutaneous depot more gently and side effects remain mild or absent entirely.
Additional side effects reported in clinical settings include mild nausea (especially at doses above 200 mg), abdominal discomfort, dizziness, and transient palpitations. These are uncommon at lower doses and virtually absent below 100 mg.
Management
- Inject slowly. This is the single highest-ROI change. Slow the plunger to a crawl.
- Start low. 50 mg is essentially asymptomatic for most researchers. Move up only when the current dose is boring.
- Warm the vial to body temperature before injection. Cold NAD+ stings more.
- Hydrate before and after. Dehydration amplifies the head pressure.
- Time it well. First injection: morning, not evening, so you're not trying to sleep through the adaptation window.
The flushing and head pressure fade with adaptation. Most researchers describe it as "intense in week 1, fine by week 3."
Stacking
NAD+ is commonly stacked with other longevity-oriented peptides. Two popular combinations:
NAD+ + MOTS-c
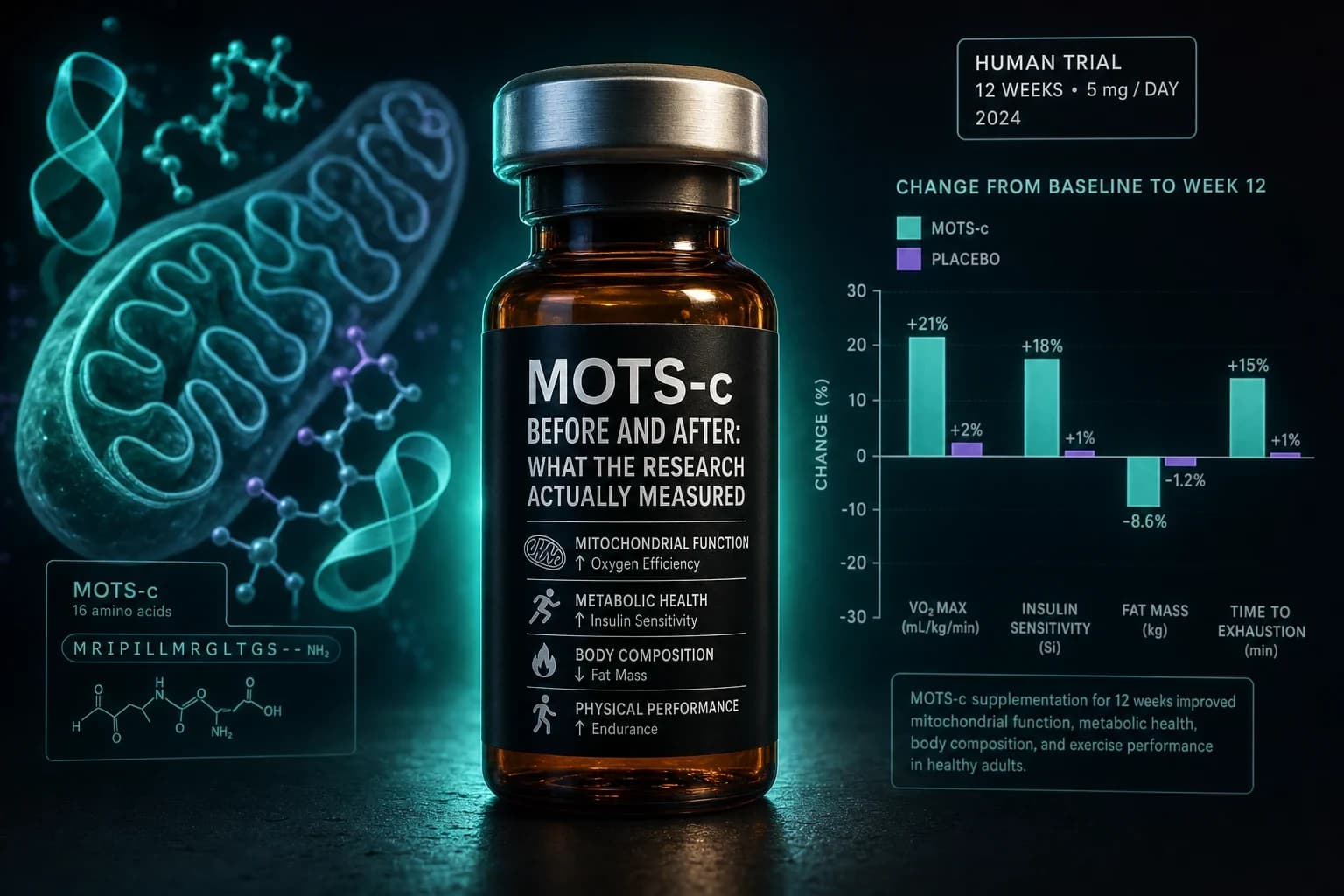
MOTS-c is a mitochondrial-encoded peptide that activates AMPK signaling and improves skeletal muscle insulin sensitivity and metabolic function. NAD+ and MOTS-c attack the mitochondrial dysfunction of aging from different angles: NAD+ restores the cofactor pool, MOTS-c restores the regulatory signaling. Research protocols typically run both during the same cycle.
Typical stack:
- NAD+ 100-200 mg SC, 2-3x/week
- MOTS-c 5-10 mg SC, 2-3x/week
NAD+ + Epithalon
Epithalon is a tetrapeptide researched for telomerase activation and circadian regulation. It's commonly stacked with NAD+ for "longevity protocols"; different mechanisms (DNA-level telomere maintenance vs coenzyme repletion) but aligned endpoints.
Typical stack:
- NAD+ 100-200 mg SC, 2-3x/week
- Epithalon 5-10 mg SC, daily for 10-20 day cycles, 2-3x per year
NAD+ + SS-31
SS-31 (elamipretide) stabilizes the inner mitochondrial membrane via cardiolipin binding. Another mitochondrial angle: NAD+ for the cofactor pool, SS-31 for membrane integrity. Stacked in advanced longevity protocols.
Protocol schedule
A typical NAD+ research cycle:
- Weeks 1-2: Titration (50 → 100 mg, 2x/week)
- Weeks 3-6: Maintenance (100-200 mg, 2-3x/week)
- Weeks 7-8: Off period
- Repeat: 2-4 cycles per year
Some researchers run continuous low-dose protocols (100 mg 2x/week indefinitely) rather than cycling. Both approaches appear in the literature. Cycling is more conservative; continuous use is better supported for people running NAD+ as a replacement for declining endogenous levels.
Storage
- Lyophilized vial: 2-8°C (refrigerator). Can tolerate room temperature short-term during shipping.
- Reconstituted vial: 2-8°C, protected from light. Use within 14 days. NAD+ is less stable than most research peptides after reconstitution.
- Do not freeze reconstituted NAD+.
- Do not shake; swirl gently to dissolve.
See peptide reconstitution: the complete guide for the general procedure.
When NAD+ makes sense
For research in:
- Mitochondrial dysfunction and age-related energy decline
- Metabolic health (especially alongside exercise programming)
- Longevity stacks with MOTS-c, Epithalon, or SS-31
- Recovery from high oxidative stress loads
Less useful for:
- Researchers who have never verified NAD+ depletion as a baseline problem
- Protocols that prioritize convenience, since injection discomfort is real
- Researchers who can tolerate the oral precursor route (NMN, NR), which is cheaper and has no injection burden, though less direct
Research access
NAD+ 1000 mg vials are available from the verified partner with 50% off using code ENHANCED. COA-verified for identity and purity.
- NAD+ research guide →
- MOTS-c research guide →
- Epithalon research guide →
- SS-31 research guide →
- Reconstitution calculator →
Disclaimer
This article is provided for research and educational purposes only. Injectable NAD+ is not approved for general human use in most jurisdictions. Nothing here is medical advice, and any decision to self-administer should involve a qualified healthcare professional.