At a glance
- The US gray-market peptide trade runs an estimated $5-10 billion a year and keeps growing
- Every peptide API traces back to Chinese manufacturers; there are no American-made peptides
- No-prescription semaglutide tested at 7-14% purity vs the 99% claimed (JAMA Network Open 2024)
- One buyer's gray-market 'tirzepatide' was melanotan II; his skin darkened instead
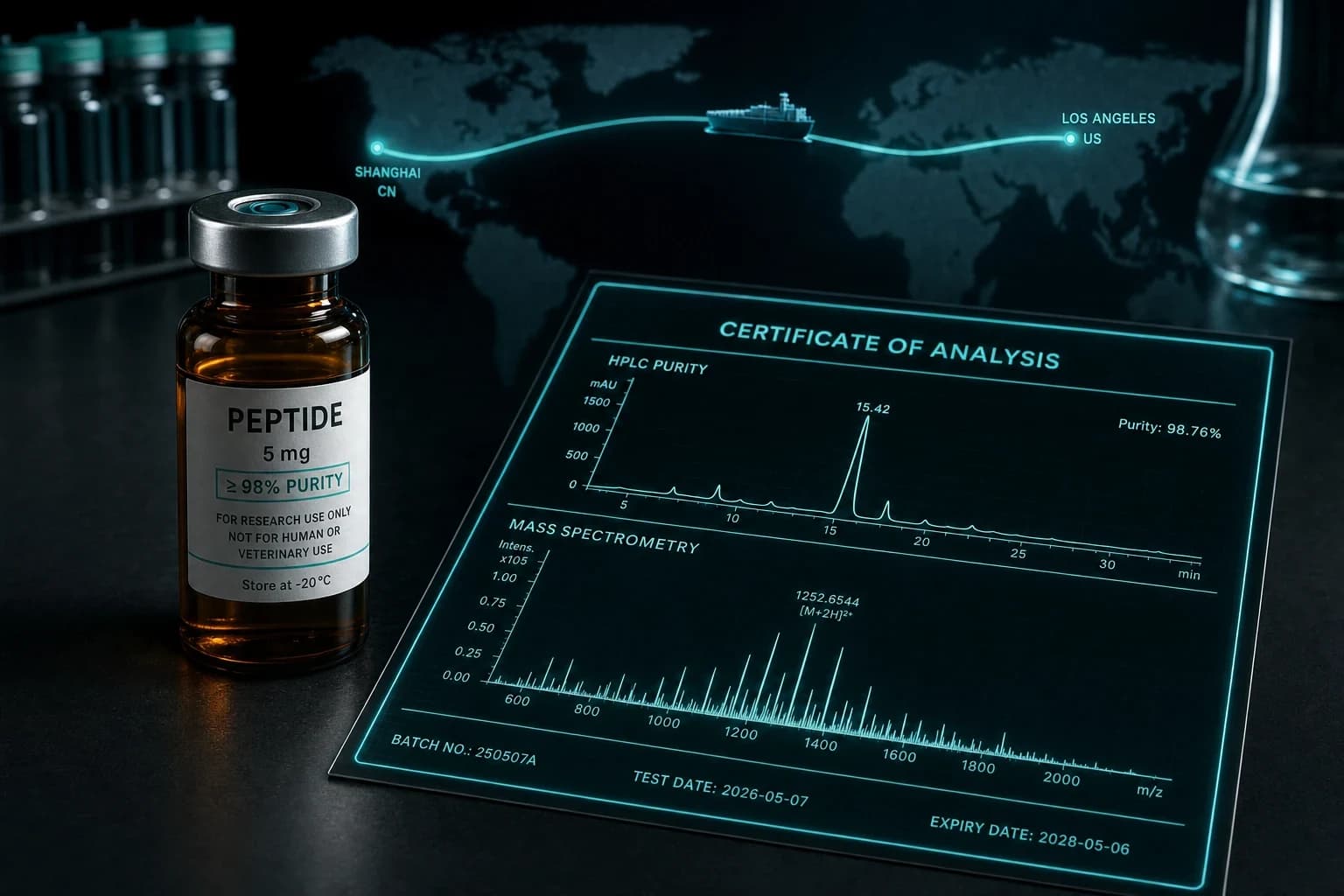
- Vet a source with a third-party HPLC and mass-spec COA matching your lot number
On the June 2026 Huberman Lab episode, Dr. Abud Bakri said the quiet part out loud: there are no American-made peptides. Every active pharmaceutical ingredient in the vial you buy, whether it ships from a licensed compounding pharmacy or a Telegram seller, started as raw material made in a Chinese factory. That single fact reframes the whole sourcing question. The label on the vial tells you almost nothing. The paperwork behind it tells you almost everything.
Bakri put a number on the underground side of the trade too. The US gray market for research peptides runs an estimated 5 to 10 billion dollars a year and it is growing. That is not a fringe corner of the supplement aisle. It is a parallel pharmaceutical economy operating with no batch consistency, no recall mechanism, and no one to call when a vial is wrong.
This guide turns what Bakri described into something you can act on. We will walk the sourcing hierarchy from safest to never-touch-it, explain what "made in China" does and does not mean for safety, cover the compounding-pharmacy markup nobody tells you about, and then get concrete about how to actually vet a source before money leaves your account.
The sourcing hierarchy, safest to riskiest
Bakri laid out a tier list, and it is worth memorizing because the gap between adjacent tiers is larger than it looks.
At the top sits standard pharmaceutical product: an FDA-approved drug, made by the originator, dispensed through a licensed pharmacy. Ozempic and Mounjaro live here. Identity, purity, sterility, and dose are guaranteed by a regulated supply chain.
Next is a quality compounding pharmacy: a 503A or 503B facility that buys USP-grade API, tests it, and compounds under sterile conditions. Legitimate, but only as good as its sourcing and its analytics.
Below that is the low-quality compounder: technically licensed, but cutting corners on testing, sterility, or API grade. The vial looks identical to the good one.
Then comes the gray market: research-use vendors selling "not for human consumption" peptides. Batch-to-batch quality is unpredictable. Some lots test clean. The next lot from the same vendor might not.
At the bottom is the black market: counterfeits laundered through real supply chains, Telegram dealers, drugs sold as something they are not. Bakri's guidance here is one word. Never.
| Source tier | Purity confidence | Dose accuracy | Sterility | Recourse if wrong | Risk |
|---|---|---|---|---|---|
| Standard pharma (FDA-approved) | Guaranteed | Guaranteed | Guaranteed | Recall + liability | Lowest |
| Quality compounding pharmacy | High (if COA on file) | High | High | Pharmacy + state board | Low |
| Low-quality compounder | Variable | Variable | Questionable | Limited | Moderate |
| Gray market (research vendor) | Per-lot only, if tested | Per-lot only | Rarely verified | Effectively none | High |
| Black market / Telegram | None | None | None | None | Do not |
Bottom line: The jump from a tested gray-market lot to an untested one is the difference between a calculated risk and a blind one. The tier is set by the paperwork, not the price or the website design.
"No American-made peptides": what it does and does not mean
The China point gets misread in both directions, so be precise about it.
Bakri's claim is about the active pharmaceutical ingredient, the raw peptide powder. The synthesis capacity for research and bulk peptides is concentrated overseas, and the US-facing supply, including material that legitimate compounders buy, ultimately originates from those manufacturers. A vendor advertising "American-made" peptides is, at best, describing where the vial was filled, not where the molecule was made.
What it does not mean is that all peptides are equally risky because they share a country of origin. A USP-grade API that arrives with a manufacturer's certificate, gets independently re-tested by a US lab, and is compounded under sterile conditions is a categorically different product from an unlabeled bag of powder bought through a chat app, even if both started in the same industrial park.
So "made in China" is not the risk signal. The risk signal is the absence of independent verification between that factory and your vial. That is the entire game, and it is why the rest of this guide is about documents.
Note: Country of origin is a distraction. The variable that actually predicts safety is whether a third-party lab confirmed identity and purity on the specific lot you are holding.
The compounding-pharmacy markup nobody mentions
Here is the ethics problem Bakri raised, and it is uncomfortable because it implicates well-meaning clinics.
Many telehealth and wellness clinics buy compounded peptides from a pharmacy at cost, then mark them up substantially to the patient, who has no idea what the underlying price was. The patient assumes the price reflects the drug. Often it reflects the clinic's margin.
His suggested question is blunt and effective: ask what your doctor pays the pharmacy versus what they charge you. A clinic operating in good faith can answer that. One that gets evasive is telling you something.
This matters for sourcing because markup and quality are not correlated. Paying a 400 percent markup does not buy you a better-tested vial. It buys you the clinic's overhead. If you are paying premium prices, the COA standard you demand should be premium too, and we will define that standard below.
The malpractice-insurance gap
This one rarely comes up and it should. Bakri pointed out that standard medical malpractice insurance does not cover prescribing non-FDA-approved injectable peptides.
Sit with the implication. If a clinician is prescribing you an injectable peptide that the FDA has not approved, and something goes wrong, the usual liability backstop may not apply. The clinic carries the upside of the sale and you carry much of the downside of the outcome.
That does not make every peptide clinic reckless. Plenty operate carefully. But it does mean the safety net you assume exists in a normal doctor-patient transaction may be thinner here than you think, which is one more reason the verification burden falls on you rather than on an institution.
The cautionary tale: when "tirzepatide" turns your skin brown
The single most instructive gray-market story Bakri told involves a buyer who thought he had purchased tirzepatide. He injected it. His skin started darkening. What he actually had was melanotan II, a melanocortin agonist that drives melanin production, sold to him under the wrong name.
The skin change was the obvious tell. The frightening part is everything that is not obvious. Melanotan II carries documented concerns about new and changing moles, and melanocortin agonism has been scrutinized for melanoma risk. A buyer expecting a GLP-1 agonist had no reason to be watching his skin at all.
The analytical literature explains how this happens. When researchers bought melanotan II from three online shops and ran it through liquid chromatography and tandem mass spectrometry, vials labeled 10 mg actually contained between 4.32 and 8.84 mg, with unknown impurities of 4.1 to 5.9 percent in two of the three (Breindahl et al., 2015, Drug Test Anal, PMID 24771717). If a vial labeled correctly is off by that much, a vial labeled incorrectly is a coin flip you did not know you were making. For the full risk picture on this compound, see our melanotan II dosing and melanoma-risk guide.
Warning: On the gray and black market, you are not just risking a weak or contaminated dose. You are risking receiving an entirely different molecule with its own side-effect profile. Identity testing, not just purity testing, is what catches this.
The data on what gray-market vials actually contain
The melanotan story is not an outlier. When analytical chemists go shopping in the no-prescription market, the results are consistent and grim.
In the most rigorous study to date, researchers identified 317 online pharmacies selling semaglutide and found that 42.27 percent were illegal operations (Ashraf, Mackey et al., 2024, JAMA Network Open, PMID 39093567). Of six vendors they test-purchased from, three never delivered and instead ran nondelivery scams demanding extra payments of 650 to 1,200 dollars under fake customs pretenses. The product that did arrive measured 7 to 14 percent purity against a 99 percent label claim, while the actual semaglutide content ran 29 to 39 percent over the stated dose.
The same group's market-surveillance write-up adds the detail that should worry you most. Alongside the purity and overdosing numbers, endotoxin was detected in every sample at 2.16 to 8.95 EU/mg, and more than half of each product failed basic visual compliance checks (Ashraf et al., 2024, J Med Internet Res, PMID 39509151). Endotoxin in an injectable is not a rounding error. It is a fever-and-shock risk.
Even regulated-channel products are not immune. The WHO issued a global Medical Product Alert in June 2024 after three falsified batches of Ozempic were detected moving through legitimate supply chains in Brazil, the UK, and the US (WHO, Medical Product Alert N°2/2024, plain text: https://www.who.int/news/item/20-06-2024-who-issues-warning-on-falsified-medicines-used-for-diabetes-treatment-and-weight-loss). And the FDA has warned that dosing errors with compounded injectable semaglutide led patients to administer 5 to 20 times the intended dose, with some adverse events serious enough to require hospitalization (FDA Drug Compounding alert, July 2024, plain text: https://www.fda.gov/drugs/human-drug-compounding/fda-alerts-health-care-providers-compounders-and-patients-dosing-errors-associated-compounded).
The pattern shows up in adverse-event surveillance too. A disproportionality analysis of 8,096 tirzepatide reports in the FDA Adverse Event Reporting System flagged "incorrect dose," extra doses, and off-label use among the most over-represented unexpected signals, alongside the expected nausea and injection-site reactions (Li et al., 2025, Endocr J, PMID 39603650). When the dose in the vial is a mystery, dosing errors stop being user error and start being baked in.
How to actually vet a source
This is the part that matters. Demand all of it, not some of it. A vendor that nails four of these five and dodges the fifth is failing the one that matters most to them.
1. A third-party certificate of analysis with HPLC and mass spec. The COA must come from an independent lab, not the vendor's own bench, and it must show two things: a purity number from high-performance liquid chromatography (HPLC), and an identity confirmation from mass spectrometry (MS). HPLC tells you how much of the vial is the peptide versus junk. Mass spec confirms it is the right peptide. The melanotan-as-tirzepatide disaster is exactly what mass spec catches and HPLC alone does not. Treat 99 percent HPLC purity with no mass-spec identity confirmation as half a document.
2. A lot number that matches the COA. A COA for "BPC-157, generally" is marketing. A COA tied to the specific lot number printed on your vial is evidence. Match the lot on the paper to the lot on the vial. If the vendor cannot produce a per-lot COA, the gray-market batch-to-batch problem is yours now.
3. A COA that is recent and complete. Check the date. A two-year-old COA recycled across every new batch is meaningless because, as Bakri stressed, gray-market quality is a per-lot property. Confirm the document lists the testing lab, the method, the date, and the lot, not just a single purity figure floating on a letterhead.
4. A reconstitution sanity check. Once it arrives, the physical product should behave correctly. Lyophilized peptide powder should fully dissolve into a clear, particle-free solution after you add bacteriostatic water; persistent cloudiness or floaters suggest contamination or a non-peptide filler. Color is a tell for specific compounds: copper peptide solutions like GHK-Cu should be visibly blue, and if yours is not, the copper has fallen out and the product is compromised. Our reconstitution calculator handles the dosing math once you trust the vial.
5. Reputable-vendor signals. Beyond the documents, look for consistency: a stable catalog, public per-batch COAs you can pull before ordering rather than after, responsive support that can answer the markup and sourcing questions, and a track record you can verify in third-party communities. A vendor that publishes COAs proactively is operating differently from one that produces a document only when cornered.
Tip: Run the documents in this order. Identity first (mass spec, right molecule), then purity (HPLC, how much), then lot match (this vial), then the physical reconstitution check (did it arrive intact). A failure at any step ends the transaction.
Where this leaves a careful buyer
The honest summary is that no purchase outside the FDA-approved channel is risk-free, and pretending otherwise is how people end up injecting endotoxin or melanotan II by accident. But "not risk-free" is not the same as "all equally bad." The verification stack above is what separates a calculated decision from a blind one.
If you are buying research-grade injectables, the standard to hold is a per-lot, third-party COA with both HPLC purity and mass-spec identity, published before you order. The vendors we track against that bar are broken down in our best legit peptide vendors of 2026 review, with compound-specific deep dives in where to buy BPC-157 with a real COA and where to buy GHK-Cu. Our lab-tests database lists the published purity documents we have collected by compound and vendor.
For COA-verified injectables that meet that standard, research-grade peptides are available from Ascension Peptides with 50% off using code ENHANCED; they publish a per-batch certificate of analysis on each lot, which is the document this entire guide tells you to demand. Whatever source you choose, hold it to the same paperwork, and read our editorial policy for how we evaluate vendors and citations.
Frequently Asked Questions
Are gray-market peptides illegal?
In the US, peptides sold "for research use only, not for human consumption" occupy a legal gray zone. Selling unapproved drugs for human use is illegal, but the research-use framing is what keeps these vendors operating. Buying for personal use sits in ambiguous territory. The legal risk is real but usually secondary to the safety risk, which is that batch-to-batch quality is unverified unless you verify it yourself with a per-lot COA.
If all peptide API comes from China, does the country of origin matter?
Not as a safety signal on its own. As Dr. Bakri noted, there are no American-made peptides; the raw material originates overseas regardless of vendor. What changes the safety equation is whether an independent US lab confirmed identity and purity on your specific lot, and whether the final product was compounded under sterile conditions. Verification, not geography, is the variable that predicts a clean vial.
What is the single most important thing to check on a COA?
Mass-spectrometry identity confirmation tied to your lot number. HPLC purity gets the attention, but purity alone cannot tell you the vial contains the right molecule. The melanotan-II-sold-as-tirzepatide case is precisely the failure that mass spec catches and a purity-only document misses. Identity first, purity second, lot match third.
How do I know if my doctor is marking up compounded peptides?
Ask directly what the clinic pays the pharmacy versus what it charges you. A clinic operating in good faith can answer. Remember that markup does not correlate with quality, so a high price is not evidence of a better-tested product. If you are paying premium prices, demand a premium COA standard to match.
Why does my GHK-Cu need to be blue?
GHK-Cu is a copper peptide, and the copper ion gives a correctly formulated solution a visible blue tint. If your reconstituted GHK-Cu is clear rather than blue, the copper has dissociated from the peptide and the product is degraded or was never properly formulated. It is a free, instant reconstitution sanity check, and one reason Dr. Bakri's framing of "if it isn't blue, the copper fell out" is genuinely useful at the kitchen counter.
This article is for research and educational purposes only and is not medical advice. Peptides discussed here are sold for research use; many are not approved by the FDA for human use. Nothing here is an endorsement to purchase or self-administer any compound. Consult a qualified, licensed clinician before making any medical or sourcing decision.