At a glance
- TRANSCEND-T2D-1 (n=537): retatrutide 12 mg cut HbA1c 2.0% and weight 15.3% at 40 weeks vs 2.6% on placebo.
- 89% of the 12 mg arm hit HbA1c below 7.0%; 83% reached 6.5% or lower.
- Trial was monotherapy in early T2D: no metformin, no SGLT2i, mean diabetes duration 2.5 years.
- Dysesthesia hit about 12.5% at 12 mg, lower than the 20.9% signal seen in TRIUMPH obesity Phase 3.
- Head-to-head vs semaglutide (TRANSCEND-T2D-2) is still pending as of July 2026.
What TRANSCEND-T2D-1 actually delivered
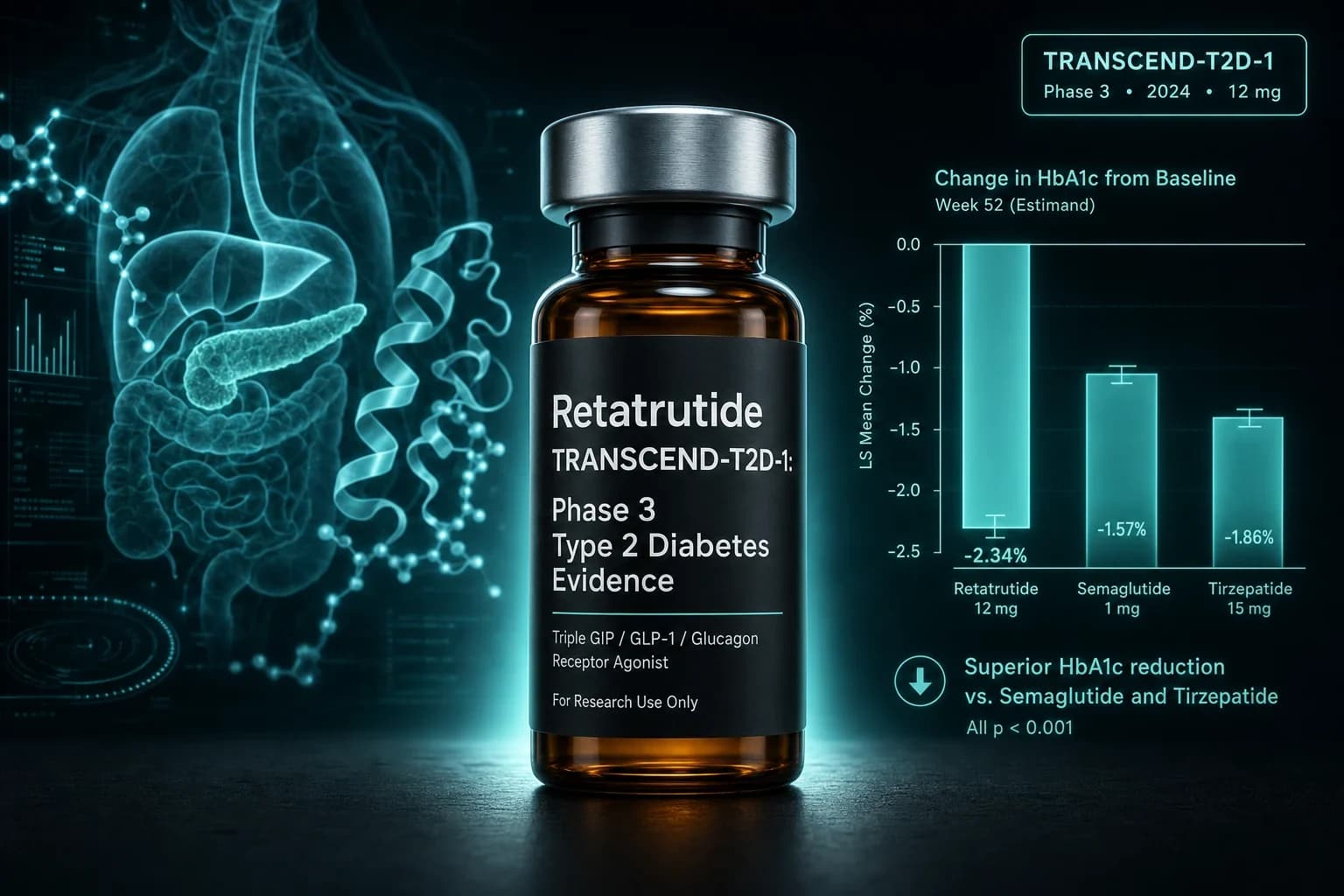
Eli Lilly's triple agonist just cleared its first Phase 3 diabetes bar. TRANSCEND-T2D-1 randomized 537 adults with type 2 diabetes to retatrutide 4 mg, 9 mg, 12 mg or placebo for 40 weeks. At the top dose, HbA1c fell 2.0 percentage points and body weight dropped 15.3 percent. In a treatment-naive cohort with an A1C between 7.0 and 9.5 percent, that puts monotherapy retatrutide on par with, or above, current best-in-class incretin therapy.
The topline landed on 19 March 2026. The full paper, Bajaj et al., Lancet 2026, followed on 6 June 2026, timed to the ADA Scientific Sessions in New Orleans. It is the first Phase 3 retatrutide readout in a diabetes-only population, and it locks in the glucose signal that the Rosenstock Phase 2 Lancet 2023 paper had projected.
This walkthrough covers what the trial measured, how it compares to SURPASS-2 tirzepatide and SUSTAIN-6 semaglutide, where the comparison stops being fair, and what the safety readout looks like after 40 weeks.
What the trial actually tested
TRANSCEND-T2D-1 (NCT06354660) is a 40-week, double-blind, placebo-controlled Phase 3 study. Design details from the Giblin et al. TRIUMPH and TRANSCEND rationale paper (Diabetes Obes Metab 2026, PMID 41090431):
- 537 adults with type 2 diabetes
- Diet plus exercise alone at baseline (about 85 percent were treatment-naive to any diabetes medication)
- HbA1c 7.0 to 9.5 percent
- BMI at least 23 kg/m²
- Mean diabetes duration 2.5 years
- 1:1:1:1 randomization to retatrutide 4 mg, 9 mg, 12 mg, or placebo
- Weekly subcutaneous dosing with dose escalation to steady state
- Primary endpoint: change in HbA1c at 40 weeks
- Key secondary: percent change in body weight
The trial did not include an active comparator. That is important. Retatrutide is compared to placebo, not to semaglutide or tirzepatide. The comparison across trials in the next section is indirect and needs to be read that way.
The trial is also monotherapy. Participants were not required to be on metformin, sulfonylurea, or SGLT2 inhibitor. That makes the population early-stage T2D: short duration, no polypharmacy, and higher baseline reserve of beta-cell function. Early-stage T2D responds better to any incretin than a late-stage T2D population would, which is why the effect sizes here beat what many later-stage trials report.
The headline numbers
Bajaj et al. reported the following at 40 weeks under the efficacy estimand.
| Endpoint | Retatrutide 4 mg | 9 mg | 12 mg | Placebo |
|---|---|---|---|---|
| HbA1c change | -1.7% | -1.9% | -2.0% | ~0% |
| Body weight change | -11.5% | -13.9% | -15.3% | -2.6% |
| Reached HbA1c < 7.0% | 82% | 88% | 89% | not reported |
| Reached HbA1c ≤ 6.5% | 75% | 82% | 83% | not reported |
| Reached HbA1c ≤ 5.7% (normoglycemia) | dose-ranked, up to about 40% | not reported |
Three things stand out.
First, there was no glycemic plateau at 40 weeks. HbA1c was still trending down at study end, and so was body weight. That matches what the Phase 2 data hinted at and what TRIUMPH-1 confirmed for obesity: retatrutide has a longer glycemic decay curve than tirzepatide or semaglutide over comparable trial windows.
Second, the placebo arm lost 2.6 percent of body weight over 40 weeks on structured lifestyle counseling alone. That is a real signal about how tightly the trial was run and how motivated the diet plus exercise arm was. In some SGLT2 add-on trials of a similar length, placebo arms are essentially weight-neutral.
Third, the normoglycemia rate is unusual. In SURPASS-2, tirzepatide 15 mg achieved HbA1c below 5.7 percent in 46 percent of participants at 40 weeks (Frías et al., NEJM 2021, PMID 34170647). Retatrutide 12 mg is now in that range in an even less pharmacologically pretreated cohort.
How TRANSCEND-T2D-1 compares to the best T2D reads
Cross-trial comparisons in obesity and diabetes drug development are always imperfect. Populations, background therapy, baseline A1C, and trial duration all differ. Even so, this is the current shape of Phase 3 T2D incretin data at July 2026, using the highest studied dose in each pivotal trial.
| Trial | Drug | Trial length | Baseline A1C | Background | A1C change | Weight change |
|---|---|---|---|---|---|---|
| TRANSCEND-T2D-1 | Retatrutide 12 mg | 40 wk | 8.3% | None (monotherapy) | -2.0% | -15.3% |
| SURPASS-2 | Tirzepatide 15 mg | 40 wk | 8.28% | Metformin | -2.30% | -12.4% (11.2 kg) |
| SUSTAIN-7 (2018) | Semaglutide 1.0 mg | 40 wk | 8.2% | Metformin | -1.5% | -6.5% (6.5 kg) |
| SUSTAIN-6 | Semaglutide 1.0 mg | ~104 wk | 8.7% | Standard care | -1.4% | ~-4.9 kg |
The most instructive line is SURPASS-2. Tirzepatide's A1C signal is still slightly larger, but retatrutide moves body weight another three percentage points, and it does that as monotherapy. The tirzepatide arm had metformin behind it. Whether the head-to-head crashes that gap or extends it is the entire point of TRANSCEND-T2D-2, the ongoing randomized trial of retatrutide versus semaglutide 1 mg in T2D patients on metformin, with or without SGLT2 inhibitor.
Bottom line: In a treatment-naive early T2D cohort, retatrutide 12 mg matches or beats tirzepatide 15 mg (SURPASS-2) on glycemic control while pushing weight loss deeper. The catch is that TRANSCEND-T2D-1 had no active comparator, so the head-to-head is still theoretical until TRANSCEND-T2D-2 reads out.
Where the cross-trial comparison stops being fair
Three specific caveats matter.
Background therapy is the biggest one. SURPASS-2 tirzepatide, SUSTAIN-2 through 5 semaglutide, and most later-stage T2D trials layer their study drug on top of metformin. TRANSCEND-T2D-1 does not. Adding metformin adds a base A1C reduction of roughly 1.0 to 1.5 percentage points, which lowers the ceiling for any drug added on top. Monotherapy retatrutide will not compete against an add-on tirzepatide arm on absolute A1C drop until the head-to-head is actually run.
Trial length matters. TRANSCEND-T2D-1 was 40 weeks. Real-world T2D pharmacotherapy is measured in decades. A 2.0 percent A1C signal at 40 weeks does not tell you anything about beta-cell durability at three or five years. That is what TRANSCEND-T2D-3 and any future outcome trials will have to answer.
Population matters. Mean diabetes duration was 2.5 years and about 85 percent of participants had not taken a diabetes drug before enrollment. Introduce metformin failure, insulin dependence, and 10 or more years of diabetes and the effect sizes will compress. TRANSCEND-T2D-1 sets a ceiling for early-stage T2D response, not a universal number.
The safety story: GI, dysesthesia, discontinuation
Retatrutide has two safety signals worth reading in the TRANSCEND-T2D-1 record.
GI adverse events tracked the incretin class. Nausea, vomiting, and diarrhea were common during dose escalation and mostly mild to moderate. That is unsurprising, since the GLP-1 component of retatrutide runs through the same central and peripheral GI circuits that produce nausea for semaglutide and tirzepatide. In the Phase 2 obesity trial (Jastreboff et al., NEJM 2023, PMID 37366315), GI events accounted for the majority of adverse events and were dose-dependent, and TRANSCEND-T2D-1's safety pattern is consistent with that Phase 2 record.
Dysesthesia is more retatrutide-specific. It is a cutaneous sensory disturbance, usually described as tingling, prickling, or burning skin sensations, that has not been reported at meaningful rates for tirzepatide or semaglutide. In the TRIUMPH obesity Phase 3s, dysesthesia hit 20.9 percent at the 12 mg dose. In TRANSCEND-T2D-1, dysesthesia reached about 12.5 percent at 12 mg. The events were mostly mild, rarely led to discontinuation, and there is no signal so far that they represent structural nerve damage. Mechanism is not settled. Candidate explanations include direct GLP-1 receptor engagement on peripheral sensory neurons, indirect effects from rapid weight loss and adipose tissue remodeling, or glucagon receptor activity in nervous system tissue.
Discontinuation rates were dose-dependent, approaching 11 percent at the 12 mg dose in TRANSCEND-T2D-1. That is meaningfully higher than the placebo arm but in the same range as high-dose tirzepatide and semaglutide discontinuation across pivotal T2D trials. No new hypoglycemia signal appeared. Retatrutide's glucagon receptor arm blunts insulin-mediated hypoglycemia, which is one of the class differentiators that has held up across Phase 2 and Phase 3.
Warning: Retatrutide is not FDA-approved for any indication as of July 2026. Every number in this article comes from a trial or a peer-reviewed publication and does not authorize personal use. Compounded retatrutide is not currently on a legal 503A pathway in the US, and the drug remains an investigational Phase 3 asset, not a prescription medication.
Where this puts retatrutide in the T2D pipeline
TRANSCEND-T2D-1 is the first of a planned five-trial diabetes program. Remaining planned reads:
- TRANSCEND-T2D-2. Head-to-head against semaglutide 1 mg in T2D patients on metformin with or without SGLT2i. Randomized. This is the answer to the caveat above.
- TRANSCEND-T2D-3. Longer-duration T2D efficacy and safety.
- TRIUMPH-2. Obesity plus type 2 diabetes population, larger sample. Retatrutide's answer to SURMOUNT-2 for tirzepatide.
- Kidney and cardiovascular outcomes. A dedicated CKD trial and cardiovascular outcome trial round out the program. Neither has reported yet.
For readers tracking the market, tirzepatide's cardiovascular outcome trial (SURPASS-CVOT) is now the reference point for late-stage GLP-1/GIP evidence, and TRIUMPH-1 is retatrutide's answer on obesity. TRANSCEND-T2D-1 does the same job for early T2D. What is still missing is a head-to-head under real background therapy and a long-term outcome trial. Both are coming.
Deeper context on the retatrutide obesity Phase 3 lives in the TRIUMPH-1 topline breakdown, which walks the 30.3 percent weight loss extension data. The retatrutide compound page covers dosing, pharmacokinetics, and stack context. Sourcing is another question, and gray-market vials of Phase 3 investigational compounds carry a specific set of risks covered in the peptide gray-market sourcing article.
What this changes for T2D treatment strategy
Treatment guidelines will not move on a single 40-week monotherapy trial. But there are three practical takeaways for clinicians and researchers watching the incretin class evolve.
- Early T2D can hit near-normoglycemia on incretins alone. If TRANSCEND-T2D-1 replicates at scale, the case for skipping metformin and going straight to an incretin in early T2D becomes harder to ignore. Metformin is safe and cheap. It is not a barrier to incretin efficacy; retatrutide monotherapy demonstrates that in a naive population.
- A1C differentiation between incretins is narrowing. SURPASS-2, TRANSCEND-T2D-1, and the SURPASS series are all clustering around 2.0 percent A1C drops in early-stage T2D. The next real differentiator between molecules is weight loss depth and organ-specific outcomes (kidney, cardiovascular, hepatic).
- Retatrutide's dysesthesia signal will get scrutiny. Any drug that produces a dose-dependent sensory nervous system signal, even a mild reversible one, will be studied hard as regulatory review approaches. Watch for post-hoc analyses characterizing the phenotype, time course, and titration strategies that reduce incidence.
What you should not read into this trial
TRANSCEND-T2D-1 does not tell you:
- How retatrutide compares to tirzepatide 15 mg head to head. That is TRANSCEND-T2D-2.
- Whether retatrutide reduces cardiovascular events. That waits for a dedicated outcome trial.
- What happens beyond 40 weeks. The weight loss slope had not plateaued and the A1C slope had not plateaued.
- Whether retatrutide is safe or effective in late-stage T2D, T1D, or patients on insulin. Those trials have not been done.
- Whether the dysesthesia signal disappears with slower titration or dose splitting. That is under active investigation.
For anyone browsing sourcing pages, retatrutide remains investigational. The overview at GLP-1 dosing comparison 2026 covers what is currently prescribable, and the GLP-1 amylin combination pipeline article puts retatrutide in context against CagriSema and amycretin. For a broader view of where the wider glucose class is heading, Marso et al. NEJM 2016 SUSTAIN-6 is still the benchmark cardiovascular outcome readout for a GLP-1 in T2D, and the retatrutide CV outcome trial will be the natural comparison when it reads out.
The takeaway
Retatrutide's first Phase 3 T2D readout does what the Phase 2 program promised: a 2 percent A1C drop, mid-teens percent weight loss, no glycemic plateau at 40 weeks, and a safety profile that is class-standard except for the still-unresolved dysesthesia signal. Whether that translates to a durable head-to-head advantage over tirzepatide waits for TRANSCEND-T2D-2. Whether the effect holds up in older, sicker, longer-diagnosed T2D populations waits for the rest of the TRANSCEND program.
For now, the trial adds a fifth pivotal Phase 3 data point to the retatrutide record after TRIUMPH-1, TRIUMPH-2 (obesity plus T2D, pending), TRIUMPH-3 (OSA, pending), and TRIUMPH-4 (knee OA, positive). All Phase 3 reads to date have hit their primary endpoints. The regulatory package is coming together, and the first weight loss drug to reset the class ceiling above 30 percent looks likely to also be the first triple agonist to enter T2D care.
Related coverage
- Retatrutide TRIUMPH-1 Phase 3 topline
- GLP-1 dosing comparison 2026
- GLP-1 amylin combination pipeline 2026
- Retatrutide reconstitution guide 30mg
- Where to buy retatrutide in 2026
- Retatrutide compound page
- Reconstitution calculator
This article is for educational and research purposes only and is not medical advice. Retatrutide is an investigational Phase 3 asset from Eli Lilly. It is not FDA-approved for type 2 diabetes, obesity, or any other indication as of July 2026. TRANSCEND-T2D-1 is a single 40-week trial in a treatment-naive early type 2 diabetes population; the numbers reported above should not be extrapolated to late-stage T2D, T1D, patients on insulin, or patients with meaningful renal or cardiovascular comorbidity. Retatrutide carries the class GI risk profile of GLP-1 receptor agonists (nausea, vomiting, diarrhea, delayed gastric emptying, gallbladder events, pancreatitis signal, thyroid C-cell tumor warning in rodent studies, and pre-procedural aspiration risk) plus a dose-dependent cutaneous dysesthesia signal that has not been reported for approved incretins. Compounded retatrutide is not currently on a legal 503A pathway in the United States. Do not source retatrutide from gray-market vendors as a substitute for prescription diabetes therapy. Consult a licensed clinician about individual treatment decisions before acting on any information here.