At a glance
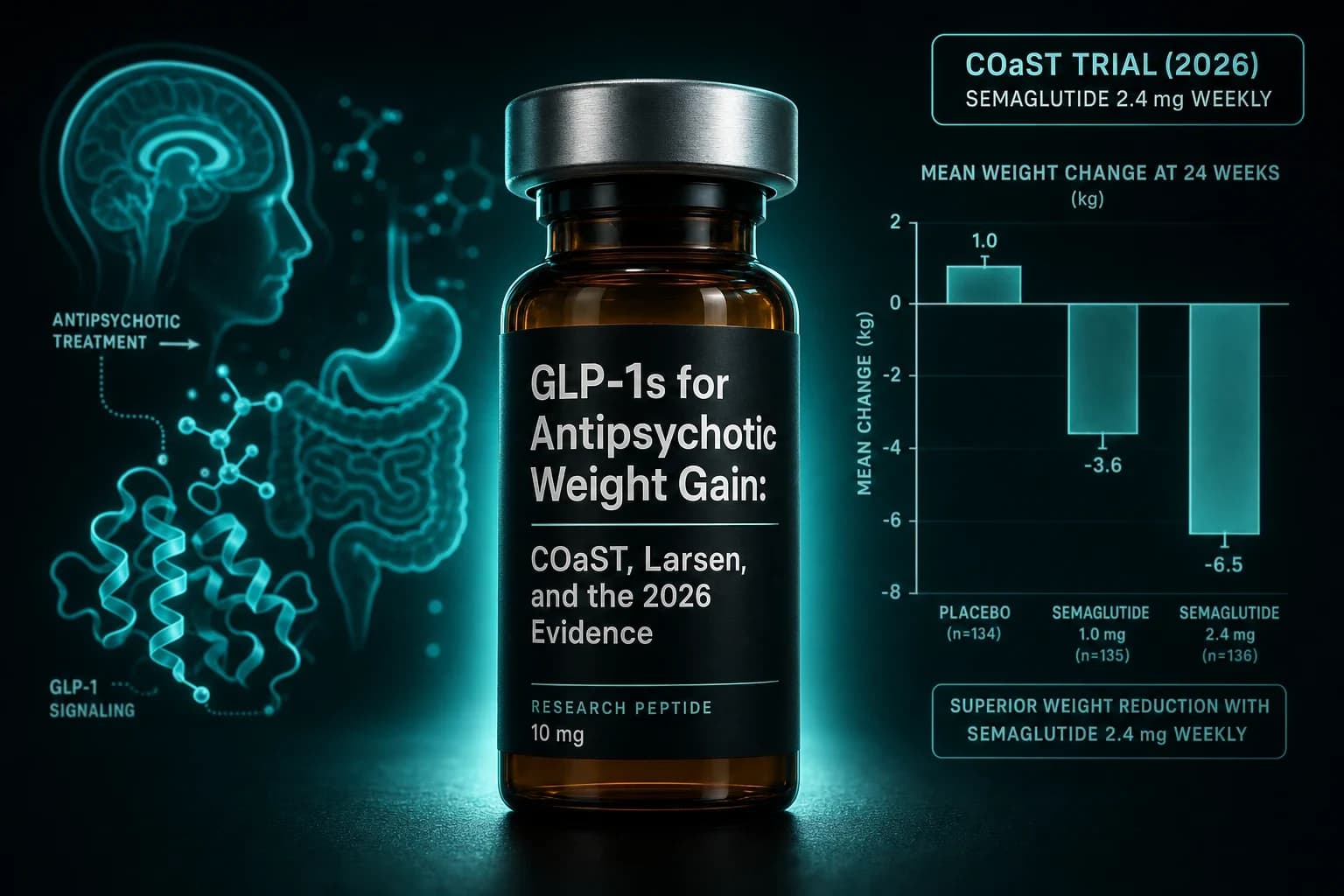
- COaST 2025 (Lancet Psychiatry) reported 13.88% body weight loss with weekly semaglutide vs 0.42% on placebo in 31 clozapine-treated schizophrenia patients over 36 weeks.
- Larsen 2017 (PMID 28601891) JAMA Psychiatry: liraglutide 1.8 mg in 103 clozapine or olanzapine patients with prediabetes normalized oral glucose tolerance in 4x more patients than placebo (NNT 2).
- Siskind CODEX 2018 (PMID 29194917) showed exenatide BD added no weight loss versus placebo over 24 weeks in clozapine-treated diabetics, despite metabolic benefit.
- Ishoy 2017 (PMID 27717222) once-weekly exenatide also failed to outperform placebo on weight, hinting that older GLP-1 RAs may underperform in this population.
- Across trials, semaglutide and liraglutide did not exacerbate PANSS scores, alter clozapine or norclozapine plasma levels, or trigger psychiatric serious adverse events.
Thirty-one adults on clozapine. Thirty-six weeks. Weekly semaglutide titrated to 2.0 mg or placebo. The semaglutide arm lost 13.88 percent of body weight. Placebo lost 0.42 percent. The between-group difference of 13.46 percent (P less than 0.0001) tripped the trial's interim early-stopping rule for success. Two-thirds of the semaglutide group hit 10 percent weight loss. PANSS scores did not budge. Clozapine and norclozapine plasma levels did not budge. That is the COaST result, published by Siskind, Mahmood, Castle and colleagues in Lancet Psychiatry 12(7):493-503 in July 2025.
The population matters. Life expectancy in chronic clozapine-treated schizophrenia runs 16 to 20 years shorter than the general population, driven almost entirely by cardiometabolic disease tied to the same antipsychotics that control psychosis. A 13.46 percent placebo-adjusted weight loss at 36 weeks is the largest effect any pharmacologic intervention has produced against antipsychotic-induced weight gain in a randomized trial.
Bottom line: Across one positive 2025 RCT (COaST), one 2017 prediabetes RCT (Larsen), one 2026 early-metabolic RCT (JAMA Psychiatry), one positive 2025 exenatide RCT (Patino), and two earlier negative or mixed RCTs (CODEX, Ishoy), semaglutide and liraglutide reduced weight, glycemia, and cardiometabolic risk in clozapine and olanzapine-treated patients without worsening psychotic symptoms or altering antipsychotic plasma concentrations. Older once-weekly exenatide trials underperformed. The evidence supports semaglutide as the first-line GLP-1 RA in this population, with liraglutide as the alternate.
Why this matters more than the average GLP-1 indication
Clozapine and olanzapine are the second-generation antipsychotics with the highest efficacy in treatment-resistant schizophrenia and the worst metabolic profile in the class. The pattern is well characterized: 5 to 12 kg of weight gain in the first 6 to 12 months, dyslipidemia within weeks, fasting glucose rise within months, and a roughly twofold increased risk of incident type 2 diabetes within a year. The mechanism involves antagonism at histamine H1, serotonin 5HT2C, and muscarinic M3 receptors, plus disrupted hypothalamic POMC and AGRP signaling. Patients gain weight even on isocaloric diets because the central drive to eat is upregulated and energy expenditure falls.
The cardiovascular cost is real and large. People with schizophrenia on second-generation antipsychotics die earlier than the general population by roughly two decades, and 70 to 80 percent of that excess mortality is cardiovascular. Metformin, lifestyle interventions, switching antipsychotics, and olanzapine plus samidorphan have all been tried, with effect sizes that rarely exceed 3 to 4 kg of weight loss after a year. The size of the COaST signal is what changed the conversation in 2025.
The trial timeline at a glance
| Trial | Year | Drug | Population | N | Duration | Weight change vs placebo | Psychiatric safety |
|---|---|---|---|---|---|---|---|
| Ishoy | 2017 | Exenatide 2 mg weekly | Obese antipsychotic-treated schizophrenia | 45 | 3 months | No difference (both lost about 2.2 kg) | No PANSS change |
| Larsen | 2017 | Liraglutide 1.8 mg daily | Clozapine or olanzapine + prediabetes, BMI 27+ | 103 | 16 weeks | -5.3 kg vs placebo, OGTT normalized in 4x more (NNT 2) | No PANSS change |
| Siskind CODEX | 2018 | Exenatide 10 mcg BD | Clozapine + T2D, obesity | 28 | 24 weeks | No difference on weight, HbA1c improved | No PANSS change |
| Whicher | 2021 | Liraglutide 3.0 mg daily | Schizophrenia, schizoaffective, FEP + overweight | 47 | 6 months | -5.7 kg vs placebo (pilot, exploratory) | No PANSS change |
| COaST Siskind | 2025 | Semaglutide 2.0 mg weekly | Clozapine + obesity (BMI 26+) | 31 | 36 weeks | -13.46 percent (P less than 0.0001) | No PANSS change, no clozapine level change |
| JAMA Psychiatry 2026 RCT | 2026 | Semaglutide 1 mg weekly | Olanzapine or clozapine + early dysglycemia (HbA1c 5.4-7.4) | Larger | 26 weeks | About -8.7 kg, HbA1c -0.25 percent | No PANSS or psychiatric worsening |
| Patino 2025 (J Affect Disord) | 2025 | Exenatide 10 mcg BD | Olanzapine, mood or psychotic disorders | 54 | 16 weeks | -3 to -4 kg vs placebo, insulin sensitivity improved | No worsening |
What Larsen 2017 actually established
The 2017 Larsen et al. trial in JAMA Psychiatry is the foundational paper. The design was rigorous for a psychiatric metabolic trial: 103 patients with schizophrenia spectrum disorders, all on clozapine or olanzapine, all overweight or obese, all with prediabetes (HbA1c 5.7 to 6.4 percent or impaired fasting glucose or impaired glucose tolerance). Patients were randomized to liraglutide 1.8 mg once daily or placebo for 16 weeks. Ninety-six completed.
The metabolic results were dramatic by the standards of antipsychotic-associated weight intervention. Oral glucose tolerance tests normalized in 63.8 percent of the liraglutide group versus 16.0 percent of placebo. The number needed to treat for prediabetes reversal was 2. Body weight fell by 5.3 kg more in the liraglutide arm. Waist circumference dropped 4.1 cm more. Systolic blood pressure fell 4.9 mmHg more. LDL cholesterol fell 0.4 mmol/L more.
Psychiatric outcomes were the question that mattered for clinicians. PANSS scores did not change. Clinical Global Impression scores did not change. No patient experienced worsening of psychotic symptoms attributable to liraglutide. The trial established two things that the field had been uncertain about: a GLP-1 RA could be added to clozapine or olanzapine without destabilizing psychosis, and the metabolic benefit was clinically meaningful in a population that historically did not respond to standard weight loss interventions.
Why the older exenatide trials looked weaker
Ishoy et al. (2017) randomized 45 obese antipsychotic-treated schizophrenia patients to once-weekly exenatide 2 mg or placebo for 3 months. Both groups lost about 2.2 kg. No between-group difference. The authors hypothesized that dopamine D2 antagonism from antipsychotics blunted the central appetite-suppressing pathway exenatide depends on, and that this could explain a smaller response in this population than in non-psychiatric obese cohorts.
Siskind's CODEX trial (2018) ran twice-daily exenatide 10 mcg in 28 clozapine-treated patients with type 2 diabetes for 24 weeks. The result was directionally similar: HbA1c improved modestly, but no statistically significant weight difference versus placebo. The CODEX sample was small and the trial was framed as a pilot, but the negative weight finding fit the Ishoy pattern.
The combined message from 2017 to 2018 was that exenatide, the first-generation GLP-1 RA with weak central penetration and modest efficacy in general obesity, was probably the wrong molecule for this population. That hypothesis got tested again when Patino et al. (2025) published a 16-week double-blind exenatide trial in 54 olanzapine-treated patients with mood or psychotic disorders in the Journal of Affective Disorders. This time the result was positive: a 3 to 4 kg between-group difference, improved insulin sensitivity, reduced self-reported hunger. The difference from CODEX was longer titration, larger sample, and a population skewed toward newer-onset weight gain rather than long-standing clozapine-associated obesity. The lesson clinicians took: exenatide can work, but it works less reliably than the newer GLP-1 RAs, and probably needs careful patient selection.
What COaST and the 2026 JAMA Psychiatry trial settle
COaST and the JAMA Psychiatry 2026 trial (Siskind D et al., Semaglutide and Early-Stage Metabolic Abnormalities in Individuals With Schizophrenia Spectrum Disorders, 83(2):128-138) are the two semaglutide RCTs that moved this field from "interesting case series" to "consider semaglutide for clozapine-induced obesity."
COaST is the most clinically informative because the patient profile is the hardest: established obesity, established clozapine therapy, high baseline metabolic risk, refractory or treatment-resistant schizophrenia. 31 patients is small, but the effect size (13.46 percent placebo-adjusted weight loss) is large enough that the trial hit its early-stopping rule. Clozapine and norclozapine plasma concentrations were measured serially and did not change, which addresses the practical clinician question of whether GLP-1 RA initiation might destabilize clozapine dosing.
The JAMA Psychiatry 2026 trial took a different angle. The population was earlier in the disease and earlier in the metabolic complication: adults aged 18 to 65, on clozapine or olanzapine for less than 5 years, with early dysglycemia (HbA1c 5.4 to 7.4 percent). They received semaglutide 1 mg weekly or placebo for 26 weeks. HbA1c dropped 0.25 percent more on semaglutide. Body weight fell about 8.7 kg more. No worsening of psychiatric symptoms. The trial extended the indication beyond established obesity into the earlier prediabetes-to-early-diabetes transition.
The Whicher 2021 pilot of liraglutide 3.0 mg in schizophrenia, schizoaffective, and first-episode psychosis added a third data point. The effect size was smaller than COaST (about 5.7 kg between-group difference at 6 months), the sample was 47, and the trial was framed as feasibility. It established that the higher liraglutide dose used for obesity outside psychiatry (the Saxenda dose) was tolerable in patients with psychotic disorders and produced meaningful weight loss.
The 2019 IPD meta-analysis and what it added
Siskind et al. (2019) in Diabetes, Obesity and Metabolism pooled individual participant data from the available randomized trials of GLP-1 RAs in antipsychotic-treated patients with elevated cardiometabolic risk. The pooled analysis covered 168 patients across the available studies up to that date. The findings: waist circumference dropped 4.5 cm more on GLP-1 RA, BMI dropped 1.36 kg/m^2 more, HbA1c dropped 0.21 percent more, fasting glucose dropped 0.4 mmol/L more, and visceral adiposity decreased significantly. The pooled weight difference was -3.7 kg, smaller than COaST or the JAMA Psychiatry 2026 trial because liraglutide 1.8 mg and exenatide carry smaller class-level effect sizes than semaglutide 2.0 mg or liraglutide 3.0 mg.
The meta-analysis matters because it preceded the COaST and JAMA Psychiatry 2026 readouts and the field was, as of late 2024, debating whether the modest pooled effect was the realistic ceiling. COaST and the 2026 RCT effectively answered: no, the ceiling is set by the molecule and the dose, and the newer GLP-1 RAs at obesity doses reproduce the 10 to 15 percent weight loss seen in non-psychiatric populations.
Mechanism: why GLP-1 RAs work even with dopamine blockade
The Ishoy hypothesis of D2 blockade interference is mechanistically reasonable but probably wrong as a class explanation. GLP-1 receptors are expressed in the arcuate nucleus on POMC and AGRP neurons, the nucleus tractus solitarius, the parabrachial nucleus, and the area postrema. The appetite-suppressing effect involves vagal afferent signaling, hindbrain integration, and central reward modulation. Dopamine D2 antagonism affects a partly overlapping but distinct circuitry. Exenatide has weak central penetration relative to liraglutide and semaglutide, which themselves cross the blood-brain barrier in a regional pattern that includes the circumventricular organs and the hypothalamus. The most parsimonious explanation for why exenatide underperformed and semaglutide and liraglutide work is the same explanation that holds in non-psychiatric obesity: the newer molecules deliver higher receptor occupancy at the relevant central sites for longer.
A second mechanism worth flagging is that olanzapine and clozapine drive weight gain partly through increased reward valuation of palatable food. GLP-1 RA signaling at central reward circuits reduces that valuation. The Patino 2025 finding of reduced self-reported hunger and tendency to overeat is consistent with this. The COaST finding of preserved or improved lean mass to fat mass ratio is also consistent with the broader semaglutide literature in non-psychiatric populations.
A practical framework for the prescribing question
| Patient profile | What the 2025 to 2026 evidence supports |
|---|---|
| Clozapine, established obesity, BMI 30+, treatment-resistant schizophrenia | Strongest case for semaglutide. COaST is the most directly applicable trial. Expect 10 to 15 percent weight loss at 6 to 9 months on the obesity dose. |
| Olanzapine or clozapine, early dysglycemia (HbA1c 5.4 to 7.4), less than 5 years on the antipsychotic | Strong case for semaglutide at the diabetes dose. The 2026 JAMA Psychiatry trial supports both glycemic and weight benefit in this profile. |
| Clozapine or olanzapine, prediabetes, BMI 27+ | Liraglutide 1.8 mg has the largest dataset (Larsen 2017). Semaglutide is reasonable if available and tolerated. |
| Stable on antipsychotic, first-episode psychosis or schizoaffective, recent weight gain | Whicher 2021 supports liraglutide 3.0 mg. Limited semaglutide data in first-episode populations specifically. |
| Mood disorder on olanzapine, weight gain in the first 6 months | Patino 2025 supports exenatide. Semaglutide is reasonable by extrapolation. |
| On metformin already, inadequate response | The Canadian case series (2023, published 2023) showed semaglutide produced mean 8.67 kg loss over 12 months in 12 patients who failed metformin. The 2026 Jacobson Margolese review (PMID 41091899) discusses sequencing. |
Note: None of the published trials studied tirzepatide, retatrutide, or any next-generation GLP-1/GIP or GLP-1/glucagon co-agonist in patients on clozapine or olanzapine. The class-effect assumption is reasonable but not directly evidenced. Until tirzepatide-in-schizophrenia trials read out, semaglutide is the molecule with the largest randomized trial in this population.
Safety: what the trials actually measured
Across COaST, Larsen, Whicher, Patino, CODEX, Ishoy, and the JAMA Psychiatry 2026 trial, the consistent psychiatric safety signal was no signal. PANSS total scores did not differ from placebo. No trial reported semaglutide, liraglutide, or exenatide-attributable psychotic exacerbation. The 2025 to 2026 disproportionality analyses of FAERS, Health Canada, and TGA databases summarized in the Jacobson Margolese review found no GLP-1 RA class signal for psychosis or mania.
Suicidality was the question that surfaced in 2023 when EMA opened a review of semaglutide and liraglutide after passive surveillance reports. The subsequent analyses, including the SELECT cardiovascular outcomes trial post hoc analysis and the GLP-1 mental health and suicidal ideation evidence article, did not find a causal signal. None of the antipsychotic-population trials reported semaglutide or liraglutide-attributable suicidal ideation. Sample sizes are too small to exclude a rare signal, but the direction of evidence does not support a class-level risk in psychiatric populations.
Clozapine plasma concentrations are the practical safety variable that matters most. COaST measured clozapine and norclozapine serially through 36 weeks of semaglutide titration. Levels did not change. This is reassuring because GLP-1 RAs slow gastric emptying, and a clinically meaningful change in clozapine absorption would have shown up as drifting serum levels. It did not.
Gastrointestinal adverse events are the dominant tolerability question. Nausea, diarrhea, and constipation occurred at the rates expected from non-psychiatric semaglutide and liraglutide trials. COaST specifically did not see increased constipation versus placebo, which matters because clozapine-induced constipation is a known clinical problem with rare but real fatal outcomes. The combination did not look additive in COaST, though the sample size is too small for a definitive answer.
What this evidence does not change
The labeled indication for semaglutide (Wegovy, Ozempic), liraglutide (Saxenda, Victoza), and exenatide (Byetta, Bydureon) does not include antipsychotic-induced weight gain. Use in this context is off-label. Insurance coverage typically depends on whether the patient meets the obesity (BMI 30+ or 27+ with comorbidity) or type 2 diabetes indication independently.
Lifestyle interventions, dietary counseling, and physical activity programs remain the first-line non-pharmacologic recommendation in every major schizophrenia treatment guideline. They produce smaller effect sizes than GLP-1 RAs in this population, but they have safety profiles and access patterns that favor them as starting interventions. Metformin remains the first-line pharmacologic adjunct in many guidelines, with a typical 2 to 4 kg effect size at 6 to 12 months.
Switching antipsychotics is sometimes proposed as a metabolic intervention. For most patients with treatment-resistant schizophrenia stabilized on clozapine, switching carries an unacceptable relapse risk that no metabolic intervention justifies. The GLP-1 RA conversation is specifically about additive metabolic management, not a substitute for the antipsychotic decision.
The trials to date are short. COaST is 36 weeks. The JAMA Psychiatry 2026 trial is 26 weeks. No GLP-1 RA has been studied beyond a year in antipsychotic-treated patients with serial measurement of weight regain after discontinuation, sustained metabolic improvement on continued treatment, or long-term psychiatric safety. The stopping GLP-1s and weight regain literature in non-psychiatric populations is informative but not directly applicable.
Where this fits in the broader GLP-1 cardiometabolic case
The schizophrenia and severe mental illness population sits at the intersection of multiple GLP-1 RA indications: obesity, type 2 diabetes risk, cardiovascular disease, hepatic steatosis, and a partly underrecognized fertility and reproductive-health burden. The semaglutide SELECT cardiovascular outcomes review covers the MACE reduction data that probably applies to this population by extrapolation, given how concentrated cardiovascular mortality is in severe mental illness. The semaglutide MASH (ESSENCE) evidence covers hepatic outcomes that matter for olanzapine-treated patients with frequent fatty liver. The GLP-1 fertility and long-term effects review covers reproductive endpoints relevant to younger first-episode patients.
The GLP-1 dosing comparison covers the practical titration question in detail. The bariatric surgery and weight regain article covers patients who have already had metabolic surgery and need GLP-1 augmentation. The Larsen and COaST dose regimens are explicit in those trials: liraglutide 0.6 mg titrating to 1.8 mg over 4 weeks, or semaglutide 0.25 mg titrating to 2.0 mg over 16 weeks. The reconstitution calculator covers the practical injection math for research-grade semaglutide preparations.
For research-only sourcing of injectable semaglutide, Ascension Peptides carries semaglutide with code ENHANCED for 50 percent off. Oral semaglutide and the next-generation oral GLP-1 candidates relevant to this population are catalogued at Limitless Biotech with code ENHANCED. The article on oral semaglutide Rybelsus vs orforglipron discusses the oral alternatives.
Bottom line: In 31 clozapine-treated patients across 36 weeks, weekly semaglutide produced 13.88 percent weight loss versus 0.42 percent placebo, with no change in PANSS scores and no change in clozapine plasma levels. In 103 clozapine or olanzapine patients with prediabetes across 16 weeks, daily liraglutide 1.8 mg normalized oral glucose tolerance in 4x more patients than placebo. In the 2026 JAMA Psychiatry trial of 26 weeks, semaglutide 1 mg cut HbA1c 0.25 percent and produced 8.7 kg of weight loss in patients with early dysglycemia. Older once-weekly exenatide trials did not show weight benefit, probably reflecting molecule-level limitations rather than a class failure. The 2026 evidence supports semaglutide as the first-line GLP-1 RA in clozapine and olanzapine-induced weight gain, liraglutide as the alternate, and off-label use under specialist supervision as the appropriate frame.
This article is for educational and research purposes only and is not medical advice. No GLP-1 receptor agonist is FDA-approved for antipsychotic-induced weight gain, schizophrenia, schizoaffective disorder, bipolar disorder, or any psychiatric indication. The data summarized above is drawn from randomized controlled trials in which semaglutide, liraglutide, and exenatide were used off-label as adjuncts to ongoing antipsychotic therapy under specialist psychiatric supervision. Clozapine and olanzapine remain the most clinically effective antipsychotics for treatment-resistant schizophrenia, and no metabolic intervention is a substitute for the antipsychotic decision, which belongs with the treating psychiatrist. The COaST trial of 31 patients, the Larsen 2017 trial of 103 patients, and the JAMA Psychiatry 2026 trial are the largest individual randomized trials of this question to date, and the sample sizes are too small to exclude rare psychiatric or metabolic adverse events that would emerge in larger registration trials. None of the trials studied tirzepatide, retatrutide, or any next-generation co-agonist in this population. GLP-1 receptor agonists carry class side effects including nausea, vomiting, delayed gastric emptying, pancreatitis signal, gallbladder events, thyroid C-cell tumor warning in rodent studies, and pre-procedural aspiration risk that apply independently of the psychiatric question. Patients on clozapine specifically should have monitoring of clozapine and norclozapine plasma concentrations during GLP-1 RA initiation and titration, even though the COaST data did not show a clinically meaningful interaction. Do not start, switch, or stop any GLP-1 receptor agonist, antipsychotic, mood stabilizer, or other psychotropic medication on the basis of this article. Consult a psychiatrist and a prescribing physician about your individual circumstances before acting on any information here.