At a glance
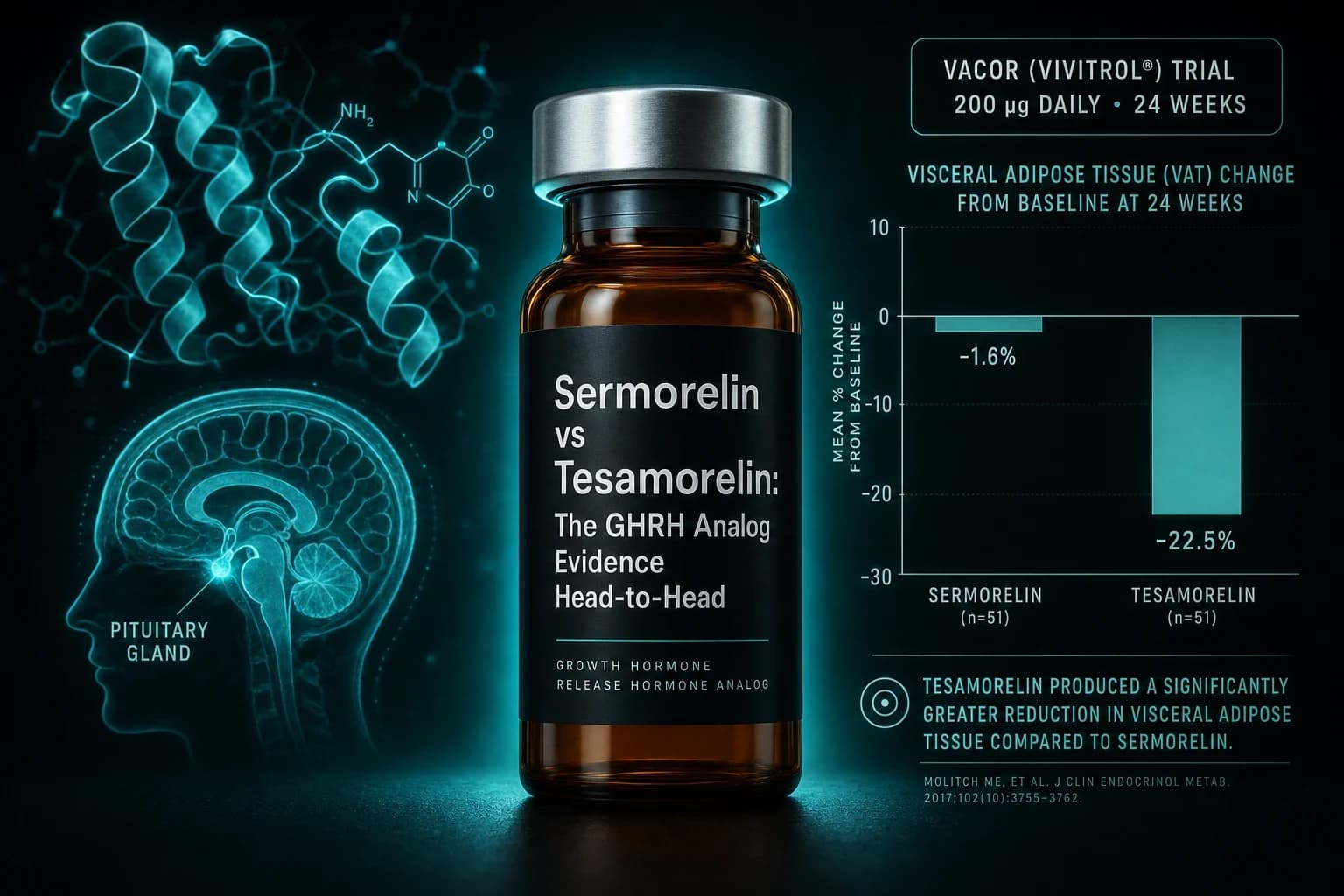
- Tesamorelin cut visceral fat 15.2% in NEJM 2007 (n=412); no equivalent VAT trial exists for sermorelin.
- Sermorelin has three small trials on IGF-1 restoration in adults 55+, each under 20 subjects.
- Tesamorelin half-life is roughly 26-38 min (DPP-IV protected); sermorelin sits around 11-12 min.
- Only tesamorelin (Egrifta SV) holds active FDA approval; sermorelin's Geref was withdrawn in 2008.
- Compounded sermorelin typically runs $100-300 per month; compounded tesamorelin $400-900+, brand tesamorelin $3,000+.
The 30-second framing
Tesamorelin is a 44-amino-acid peptide with two Phase III trials, FDA approval, and a brand-name Egrifta SV price that runs several thousand dollars per month. Sermorelin is a 29-amino-acid GHRH fragment with no active FDA approval for adults, a compounding-pharmacy price a fraction of that, and a clinical evidence base that mostly stopped growing in the late 1990s.
Both bind the same GHRH receptor. Both trigger endogenous growth hormone release. Both preserve the pulsatile GH pattern that exogenous rhGH flattens. Treating them as interchangeable "GHRH analogs" is the mistake most vendor pages make. The endpoints they have been trialed against are different, the populations are different, and the reasonable research use cases diverge more than the shared receptor suggests.
This is the head-to-head we walk research readers through when they ask which one fits the question they are actually asking.
What each peptide actually is
Sermorelin is GHRH(1-29)-NH2, the first 29 amino acids of the 44-amino-acid endogenous human growth hormone-releasing hormone. Those 29 residues carry the full biological activity of the parent peptide. Truncating everything after position 29 makes sermorelin easier to synthesize, but it leaves the N-terminus exposed to the same enzymatic clipping that limits native GHRH's usable half-life.
Tesamorelin is a modified full-length GHRH(1-44) with a trans-3-hexenoic acid group attached at the N-terminus. That single fatty-acid modification blocks dipeptidyl peptidase-IV (DPP-IV) from cleaving the peptide at the vulnerable Tyr1-Ala2 bond. The rest of the sequence is unchanged from native GHRH.
Practically: sermorelin trades molecular protection for structural simplicity; tesamorelin trades simplicity for enzymatic protection. Both engage GHRH receptor 1 on somatotroph cells in the anterior pituitary. Neither delivers growth hormone directly. Both work only if the pituitary itself can still respond to a GHRH pulse. That last point matters more than most vendor pages acknowledge, because it is the single reason GHRH analogs are not a substitute for true GH replacement in adults with pituitary damage.
Half-life and why it matters less than you think
The DPP-IV modification gives tesamorelin a plasma half-life of roughly 26 to 38 minutes after subcutaneous injection. Sermorelin, unprotected at the N-terminus, clocks in around 11 to 12 minutes.
Neither number is long by any drug metric. That is by design. GHRH is a physiologic secretagogue. Its natural role is to trigger a brief pulse, then clear. If either peptide stayed elevated for hours, it would flatten the pulsatile GH profile the therapy is trying to preserve. What tesamorelin's extended half-life actually buys is a more predictable single daily dose reaching the pituitary intact, rather than sustained receptor stimulation.
Sermorelin's shorter window is why the clinical literature tends toward bedtime dosing. Endogenous GH release peaks during slow-wave sleep, so pulsing the pituitary right before that window rides an existing rhythm rather than fighting it. Tesamorelin's approved label is also once-daily bedtime for the same reason, plus a practical one: patients tolerate injection-site reactions better if the timing coincides with the end of the day.
Neither peptide is a candidate for CJC-1295-DAC-style permanent receptor saturation. Both are pulse-preserving by construction. If your research question involves flat, prolonged GHRH signaling, both peptides answer that question the same way: no.
Tesamorelin's clinical file
Two Phase III trials sit under Egrifta's 2010 FDA approval. Both were run in HIV-positive adults with lipodystrophy, both used 2 mg subcutaneously daily, and both have been reproduced across follow-up studies since.
The first trial (Falutz et al., NEJM 2007, n = 412) reported a 15.2% reduction in visceral adipose tissue at 26 weeks with tesamorelin versus a 5.0% increase in the placebo arm (p < 0.001). Trunk fat, waist circumference, and triglycerides all shifted in the treatment group's favor. IGF-1 rose into the upper physiologic range without exceeding it in most patients. The trial was one of the first large-cohort demonstrations that stimulating endogenous GH release, rather than administering exogenous rhGH, could produce clinically meaningful body-composition changes without the fluid-retention profile that limited earlier GH therapy in this population.
The extension trial (Falutz et al., JAIDS 2010, n = 404) followed patients out to 52 weeks. Sustained treatment held the VAT reduction at approximately 18%, and stopping tesamorelin caused VAT to reaccumulate. Glucose parameters over the full year showed no clinically significant deterioration, which had been the pre-registration concern given growth hormone's known insulin resistance signal.
A later mechanistic trial (Stanley et al., JAMA 2014, n = 50) added liver fat as an endpoint. Six months of tesamorelin dropped liver fat fraction by 2.0 percentage points versus a 0.9-point increase with placebo (p = 0.003) and reduced VAT by 34 cm² versus placebo's 8 cm² gain. The trial was small, but it introduced the possibility that tesamorelin does more than shift adipose distribution. It also shrinks ectopic fat in the liver.
Beyond the labeled HIV population, tesamorelin has been studied in non-HIV NAFLD, in patients on integrase-strand-transfer inhibitors, and for muscle-fat effects. The evidence base outside HIV lipodystrophy is thinner and mostly exploratory, but the mechanism (GHRH → GH → IGF-1 → lipolysis in visceral depots) does not depend on HIV status. For a deeper dive on the full trial file and the mechanistic rationale, our tesamorelin visceral fat guide covers each pivotal study in more detail.
Sermorelin's clinical file
Sermorelin's peer-reviewed adult evidence base is older, smaller, and less endpoint-driven. The weakness reflects trial design rather than mechanism failure: most trials were short, involved small cohorts, and were built around biochemistry endpoints rather than clinical outcomes.
Corpas et al. (JCEM 1992) gave older men GHRH(1-29) at 0.5 mg or 1 mg subcutaneously twice daily for 14 days. IGF-1 rose in a dose-related fashion, and the higher-dose group returned to a range typical of younger adults. That was the proof-of-concept study for using GHRH(1-29) to restore the age-related decline in the GH/IGF-1 axis, and it remains the foundational citation most compounding-pharmacy protocols trace back to.
Vittone et al. (Metabolism 1997) took the same 1-29 fragment, gave 2 mg nightly to 11 men aged 64-76 for 6 weeks, and roughly doubled nocturnal GH output. IGF-1 did not rise significantly over that timeframe, suggesting the 6-week window was too short for downstream biochemistry to catch up with the pulsatile GH increase.
Khorram, Laughlin, and Yen (JCEM 1997) went longer. Nineteen adults aged 55-71 received GHRH(1-29) at 10 μg/kg nightly for 16 weeks after a 4-week placebo run-in. Nocturnal GH, IGF-1, and IGFBP-3 all rose significantly in both sexes. Lean body mass increased by an average of 1.26 kg in the men. Skin thickness increased in both groups.
Beyond those three trials and a small number of variations, the adult sermorelin literature effectively stops. Sermorelin's original branded product (Geref, from Serono) was withdrawn from the US market in 2008 for commercial reasons, not safety. Most current adult prescribing runs through 503A compounding pharmacies. Our sermorelin clinical research guide walks through the full mechanistic and trial history in more detail.
Head-to-head comparison
The table strips out the parts that should not drive a decision and keeps the parts that should.
| Feature | Sermorelin | Tesamorelin |
|---|---|---|
| Structure | GHRH(1-29)-NH2 | Modified GHRH(1-44) with trans-3-hexenoic acid |
| Molecular weight | ~3,358 Da | ~5,196 Da |
| Plasma half-life (SC) | ~11-12 min | ~26-38 min |
| Route | Subcutaneous | Subcutaneous |
| Typical research dose | 100-500 mcg nightly (compounding); trials used 0.5-2 mg | 2 mg nightly |
| FDA approval status | None active (Geref withdrawn 2008) | Egrifta / Egrifta SV, approved 2010 for HIV lipodystrophy |
| Largest published RCT | ~19 adults (Khorram 1997) | 412 adults (Falutz 2007) |
| Best-evidenced endpoint | Nocturnal GH increase, IGF-1 restoration in older adults, modest lean mass gain | Visceral fat reduction (15-18%), modest liver fat reduction |
| Trial population | Healthy older adults (55-80) | HIV-positive adults with lipodystrophy |
| 503A compounded availability (US) | Widely available | More limited; branded product primary channel |
| Estimated monthly cost | Compounded: $100-$300 range | Compounded: $400-$900 range; brand (Egrifta SV): $3,000+ |
Bottom line: Tesamorelin has the clinical file, an FDA-approved indication, and specificity to visceral fat as an endpoint. Sermorelin has a longer research history, broader access channels, and IGF-1 restoration data in older adults. Use case, not brand loyalty, should drive the choice.
Dosing patterns from the research literature
Sermorelin dosing in the published adult literature clusters around two protocols. Corpas used 0.5-1 mg twice daily; Vittone and Khorram used 2 mg or approximately 10 μg/kg once nightly. Current 503A compounding-pharmacy protocols typically start much lower (100-300 mcg subcutaneous nightly) than the trial doses. The mismatch is not fully explained by the peer-reviewed record. The lower dose reflects an emphasis on avoiding IGF-1 supraphysiologic excursions in a broader adult population rather than replicating trial pharmacology in age-restricted cohorts.
Tesamorelin's dose is straightforward: 2 mg subcutaneous once daily. That is the dose the FDA approved, the dose used in both Phase III trials, and the dose used in the JAMA 2014 liver-fat trial. There is no widely accepted "microdose" protocol for tesamorelin in the way there is for sermorelin. Some clinicians use every-other-day dosing to reduce cost or IGF-1 excursion; that is off-label and not supported by any of the pivotal trials.
For anyone reconstituting either compound, the standard math applies. Our reconstitution calculator handles the unit-per-dose conversions, and the sermorelin dosage chart and tesamorelin dosage chart hold pre-worked tables for common vial sizes and dose targets.
Note: Neither peptide should be dosed by extrapolating from short-term biochemistry to long-term clinical outcomes. IGF-1 rising into the upper physiologic range is the biochemical marker most studies use to titrate. Sustained IGF-1 above age-adjusted normal is the marker most clinicians use to back off.
Cost, access, and the 2026 compounding market
Tesamorelin's brand-name product (Egrifta SV, Theratechnologies) is priced in the low thousands per month in the US, with insurance coverage largely limited to the FDA-approved HIV-lipodystrophy indication. For research use or off-label investigation, the compounding-pharmacy route sits well below that but still runs meaningfully more than sermorelin, largely because the peptide is synthetically more complex and demand from HIV-lipodystrophy prescribing keeps the API price elevated.
Sermorelin has been the workhorse of 503A compounding pharmacies for GH-optimization protocols since Geref's 2008 withdrawal. Vial pricing at reputable compounding pharmacies typically lands under $300 per month at common doses, and access channels (telehealth clinics, research vendors) are broader than for tesamorelin.
The FDA's evolving posture on 503A peptide compounding is the wildcard neither pricing snapshot fully captures. Sermorelin's regulatory classification has shifted over 2023-2025, affecting some pharmacy access, though it has generally remained available. Tesamorelin's approval-backed availability is less exposed to that regulatory shift because the branded product provides an approved distribution channel independent of 503A rules. For anyone building a research protocol they want to maintain over 12+ months, that regulatory stability matters, and our tesamorelin compound page tracks the current label and access status.
Compounded peptide sourcing quality varies widely. The relevant questions are the same for both compounds: is there a current certificate of analysis, does the vendor test finished product (rather than only the raw API), and is potency verified independently? Our Ascension Peptides review walks through how to evaluate that stack of questions on the injectable side, and the sermorelin compound page captures the current market pricing snapshot.
Which peptide fits which research question
The clean way to think about this: pick the peptide whose evidence base is closest to the endpoint you care about.
If the research question is visceral fat reduction: Tesamorelin is the only option with head-to-head clinical evidence. The Falutz 2007 and Stanley 2014 trials both measured VAT by CT and MRI. Sermorelin has no published trial with visceral fat as a primary endpoint.
If the research question is age-related IGF-1 restoration in older adults: Sermorelin's evidence base fits better. Corpas, Vittone, and Khorram all measured IGF-1 changes in adults over 55, and doses/schedules from those trials remain the reference protocols.
If the research question is HIV-associated lipodystrophy specifically: Tesamorelin, without qualification. It is the only GHRH analog with an FDA-approved indication for this population, and Egrifta remains the reference standard of care.
If the research question is broad GH-axis optimization in a healthy adult context: Neither peptide has strong evidence. Both raise IGF-1 modestly in the short term. Neither has been trialed against clinical outcomes like sarcopenia, cognitive function, or metabolic markers in that population at the level Phase III designs would require. Vendor pages that claim otherwise are extrapolating well past the data.
If the research question is stackability with a GH secretagogue (GHRP-2, ipamorelin, MK-677): Sermorelin has more of a compounding tradition here. Combined GHRH plus GHRP dosing exploits the synergy between two receptor systems (GHRH-R stimulation plus ghrelin-receptor stimulation) to produce larger GH pulses than either alone. Our sermorelin vs CJC-1295 vs ipamorelin comparison covers that combination protocol in more detail.
Safety and monitoring
Tesamorelin's most consistent adverse events across the Phase III trials were injection-site reactions (erythema, pruritus) and arthralgia. Glucose parameters shifted modestly (small increases in fasting glucose and HbA1c) but did not cross into clinical diabetes rates different from placebo over 52 weeks. Fluid retention and carpal tunnel symptoms were rare compared with what direct rhGH administration produces, which is a mechanistic advantage of preserving pulsatility.
Sermorelin's safety record in the short-term adult trials was similarly benign: transient facial flushing, injection-site reactions, and occasional headaches. No trial has been powered to detect long-term risks in the way Egrifta's post-marketing surveillance has been for tesamorelin.
The theoretical concerns common to both peptides are the same as for any GH-axis intervention. Sustained IGF-1 elevation above age-adjusted normal is associated in observational data with cancer incidence signals, and any patient with active malignancy or a history of malignancy is generally excluded from GHRH-analog research. Both peptides should be avoided in that context. IGF-1 monitoring at 4-6 weeks after initiation, then quarterly, is the standard approach for either compound.
Warning: Neither sermorelin nor tesamorelin should be assumed safe for people with active or historical malignancy, severe uncontrolled diabetes, or acute critical illness. The safety data supporting broader use come from carefully selected trial populations, not from unrestricted use.
Bottom line
The useful framing asks which peptide has been trialed against the endpoint you actually care about, rather than which one is better in the abstract.
Tesamorelin has the file. FDA approval, two Phase III trials totaling more than 800 patients, a specific and well-measured endpoint (visceral fat), and a supporting liver-fat signal from the JAMA 2014 trial. If visceral adiposity is the research question, tesamorelin is the answer.
Sermorelin has the history and the access. The clinical trials are smaller and older, but they establish that GHRH(1-29) restores age-related declines in GH pulsatility and IGF-1. If IGF-1 restoration in older adults is the research question, sermorelin's evidence base fits, and current access, cost, and regulatory conditions make it more workable for long-horizon research protocols.
The competitor swap test still applies. If a peptide vendor tells you sermorelin will do everything tesamorelin does, or vice versa, they are marketing to whichever one is in stock. Neither is generic for the other. Neither is a replacement for endogenous physiology in an adult who does not have documented GH deficiency. And neither is FDA-approved for anti-aging.
For readers building an injectable research stack, Ascension Peptides carries both sermorelin and tesamorelin with 50% off using code ENHANCED. Review the vendor evaluation and COA process before you order either one; the sourcing questions matter more than the price gap between them.
This article is for research and educational purposes only. Neither sermorelin nor tesamorelin is approved as a general anti-aging, longevity, or performance intervention in the US or EU. Tesamorelin (Egrifta SV) is FDA-approved only for HIV-associated lipodystrophy. Any use outside that indication is off-label and requires a qualified prescribing clinician. Cited studies are peer-reviewed publications linked inline via PubMed. Nothing in this article is medical advice; specific dosing, monitoring, and safety decisions should be made by a licensed practitioner familiar with your health status.