At a glance
- Elamipretide (SS-31) is the only peptide on this list with FDA approval (Barth syndrome, 2025), not for anti-aging.
- GHK-Cu modulates over 4,000 human genes across collagen, antioxidant, and DNA-repair pathways (Pickart 2018, PMID 29986520).
- Sermorelin raised nocturnal GH 3-4x and IGF-1 by 35% in men aged 64-76 (Vittone 1997, PMID 9005976).
- Thymosin alpha-1 improved influenza vaccine antibody response in elderly RCTs (Ershler 2007, PMID 17600281).
- MOTS-c, FOXO4-DRI, and epithalon rest on mouse or single-lab data, not human anti-aging trials.
Every "best anti-aging peptides" list you have seen this year ranks by TikTok, biohacker Substack, or a supplement store's margin. This one ranks by whether the peptide has ever been given to a person under a randomized protocol and had its effect measured against placebo.
That filter kills most of the field. What is left is a much shorter list than the internet suggests, with a clear split between compounds that have real human evidence for a defined age-related endpoint and compounds that rest on animal work plus decades of forum enthusiasm. The order below is honest, and the tier is disclosed for every entry.
The one filter that separates anti-aging peptides from anti-aging marketing
"Anti-aging" is not a regulatory endpoint. No agency approves a drug because it makes you biologically younger. So peptides marketed for "longevity" are almost always approved (if at all) for a specific age-associated disease, or not approved at all and sold as research chemicals.
The useful question is which peptides target a well-defined aging pathway, and which of those have been tested in humans against a placebo or a matched natural-history cohort. Three pathways drive most of the biology:
- Mitochondrial decline and cardiolipin damage in aged cells.
- Growth hormone and IGF-1 collapse (the somatopause), which drops lean mass and skin quality after age 40.
- Immunosenescence and the accumulation of senescent cells that leak inflammatory signals.
Every peptide on the list below hits at least one of those three levers. Whether the human data is strong, thin, or entirely absent decides its tier.
Evidence-quality snapshot
| Peptide | Best human evidence | Aging pathway | Anchor citation | Tier |
|---|---|---|---|---|
| Elamipretide (SS-31) | Phase 2/3 RCT in Barth syndrome; FDA-approved 2025 | Cardiolipin, mitochondrial function | Reid Thompson 2021 PMID 33500606 | A (approved, narrow) |
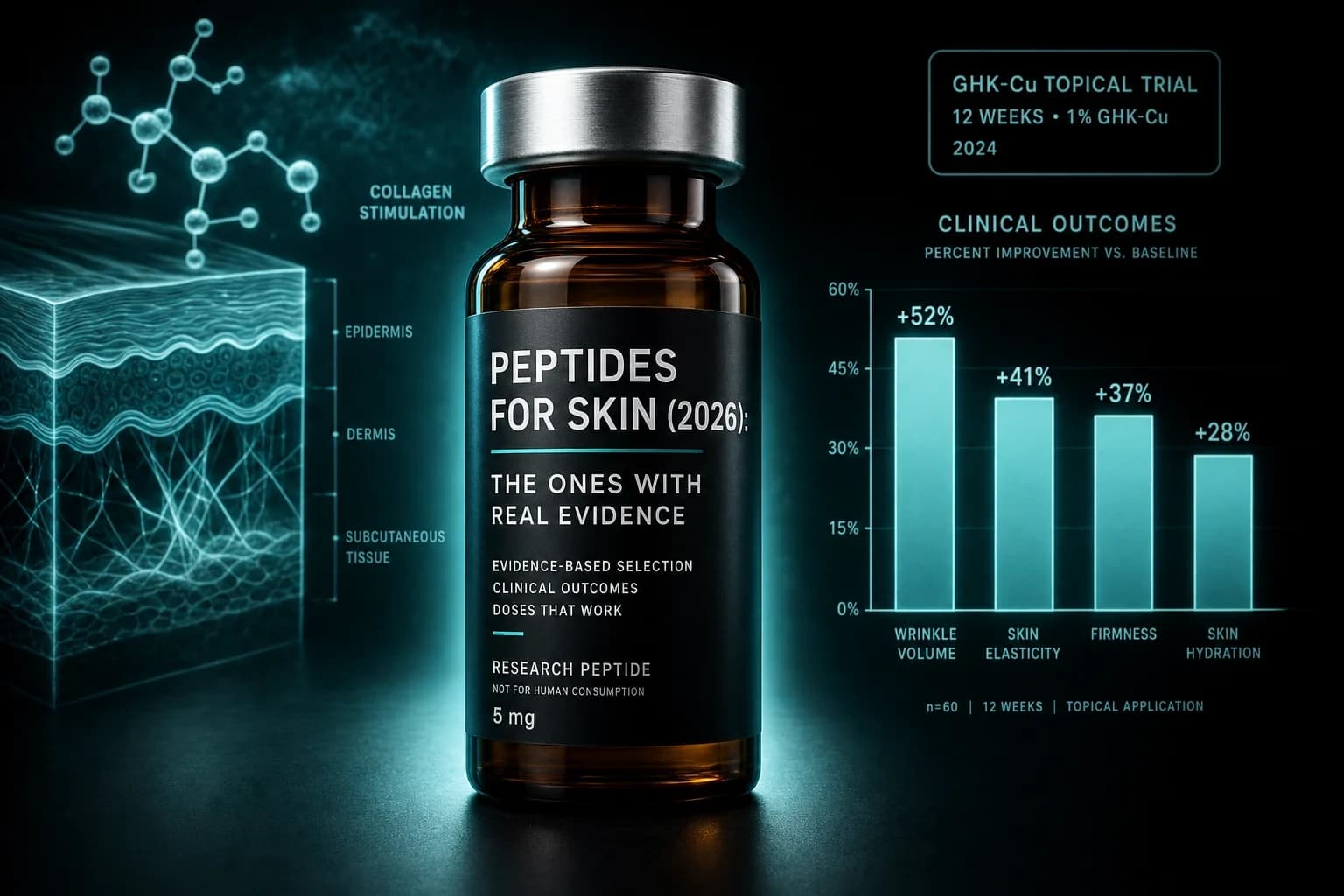
| GHK-Cu | Multiple controlled skin trials over 30 years | Gene regulation, collagen, wound repair | Pickart & Margolina 2018 PMID 29986520 | A (topical) |
| Sermorelin / GHRH 1-29 | Placebo-controlled trials in elderly men | Somatopause, GH-IGF axis | Vittone 1997 PMID 9005976 | A (older adults) |
| Thymosin alpha-1 | Vaccine adjuvant RCTs in elderly | Immunosenescence, T-cell function | Ershler 2007 PMID 17600281 | B (adjunctive) |
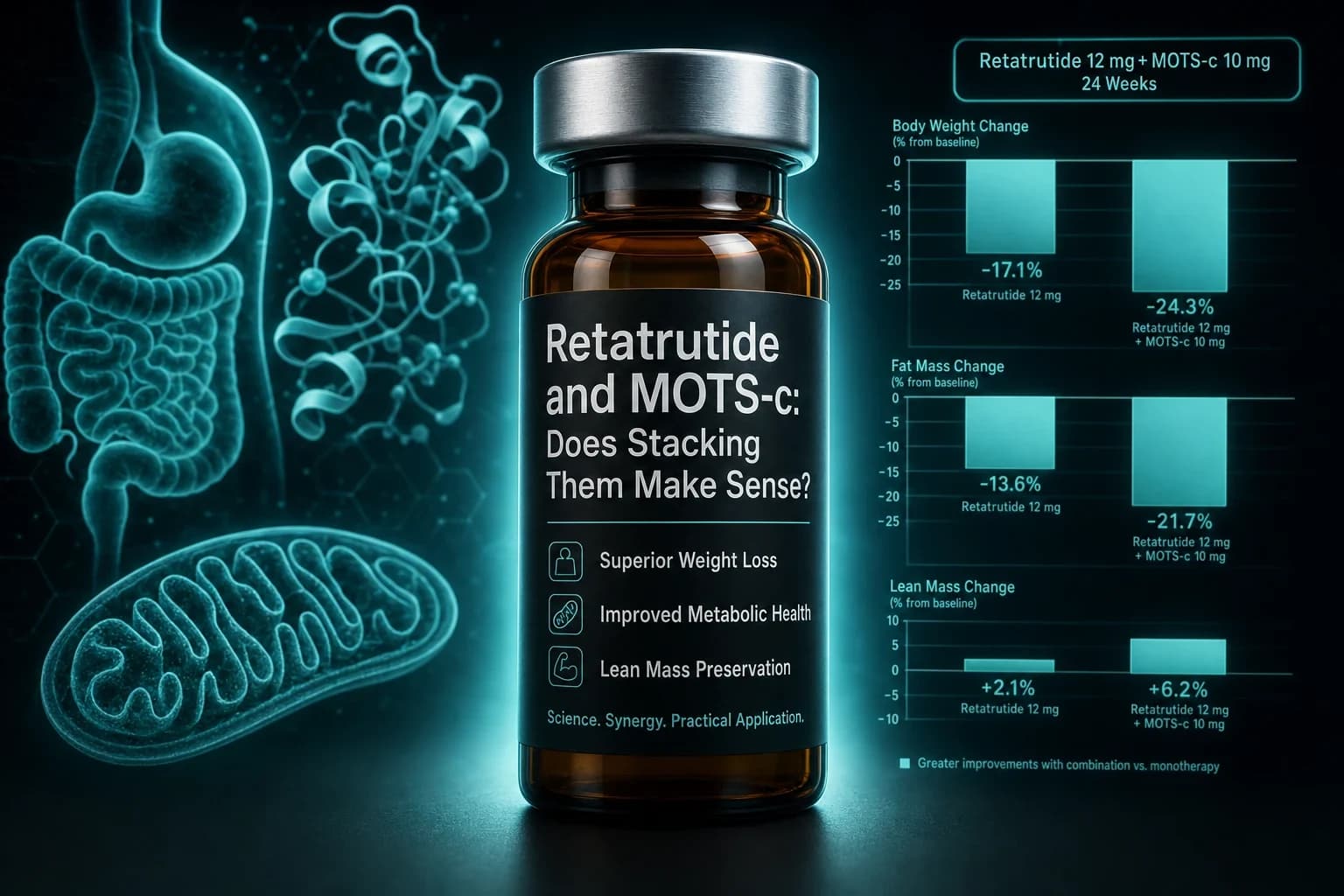
| MOTS-c | One human exercise-induction biopsy study; rest is mouse | Mitochondrial-encoded metabolism | Reynolds 2021 PMID 33473109 | B (mostly preclinical) |
| FOXO4-DRI | None in humans; mouse-only | Senescent cell clearance | Baar 2017 PMID 28340339 | C (preclinical) |
| Epithalon (AEDG) | Single Russian research group; no Western RCT | Telomerase induction, pineal | Khavinson 2003 PMID 12937682 | C (single-lab) |
The rest of this guide walks each row of that table in order, so you can see the actual data instead of the marketing framing.
Elamipretide (SS-31): the only peptide on this list with FDA approval
Elamipretide, also called SS-31, is a small aromatic-cationic peptide that binds to cardiolipin on the inner mitochondrial membrane. Cardiolipin damage is one of the more consistent findings in aged tissue: as it accumulates, the electron transport chain leaks electrons, ATP output drops, and reactive oxygen species rise. SS-31 stabilizes cardiolipin without changing its structure, and preserves cristae architecture in stressed mitochondria.
The reason it sits in Tier A is not because someone ran a longevity trial. It is because SS-31 was studied under a Phase 2/3 randomized crossover design in Barth syndrome, a rare mitochondrial disease of cardiolipin metabolism. In Reid Thompson et al. 2021 (Genetics in Medicine, PMID 33500606), 12 patients were randomized to 40 mg subcutaneous elamipretide daily or placebo for 12 weeks, crossed over, then continued in open-label extension. The 36-week open-label data showed a 95.9-meter improvement in the 6-minute walk test (p = 0.024) and a 2.1-point drop in the Barth Syndrome Symptom Assessment score (p = 0.031).
Long-term follow-up from the TAZPOWER 168-week open-label extension (Karaa et al. 2024, PMID 38602181) tracked eight patients out past three years on daily elamipretide, with sustained improvements in cardiac stroke volume and skeletal muscle performance. That data pack drove FDA approval of elamipretide (brand name Forzinity) for Barth syndrome in September 2025.
So what does that have to do with anti-aging? Two things. First, it is the only peptide on this list that has cleared an FDA advisory committee, which sets a floor for the quality of the evidence package. Second, the mitochondrial-decline mechanism is a general aging pathway, and Phase 2/3 trials of elamipretide in age-related conditions (heart failure with preserved ejection fraction, primary mitochondrial myopathy, age-related macular degeneration) are ongoing. If any of them read out positive, SS-31 becomes the first peptide with formal age-related indications, not just a rare-disease label.
What this does not mean: buying research-grade SS-31 to inject subcutaneously does not have anti-aging outcome data behind it. The Barth data proves the compound works on cardiolipin. It does not prove that a healthy 45-year-old gets a longevity benefit. Anyone claiming that is running past the evidence.
For the mechanistic deep dive and the FDA-approval context, see the full SS-31 elamipretide breakdown and the SS-31 dosing chart.
GHK-Cu: 30 years of controlled skin data, best evidence in the topical column
GHK-Cu is a tripeptide (glycyl-L-histidyl-L-lysine) bound to copper. It occurs naturally in human plasma, drops sharply with age, and has been studied continuously since Loren Pickart's early work in the 1980s. It is the peptide on this list with the deepest published record.
The strongest single reference is Pickart & Margolina 2018 (Int J Mol Sci, PMID 29986520), a review of published gene-expression data showing that GHK-Cu modulates the expression of more than 4,000 human genes at a threshold of at least 50 percent change. The regulated pathways cluster around collagen and elastin synthesis, antioxidant response, DNA repair, wound healing, and ubiquitin-proteasome activity. That gene-regulation profile explains why controlled topical trials have consistently reported reduced wrinkle depth, improved skin thickness, and firmer photoaged skin.
One important nuance is route. GHK-Cu is Tier A when applied topically to skin, where the human trial record is real and long. Injected GHK-Cu is a different question: the preclinical wound-healing and organ-protective work is impressive, and there is a plausible systemic anti-inflammatory story, but there are no adequately powered human trials of injectable GHK-Cu against a placebo for any age-related endpoint. Users who inject are extrapolating from mouse and cell data.
Bottom line: GHK-Cu earns its Tier A rating on skin, and that is not a small win. The photoaged skin trial data holds up. Systemic anti-aging benefits from injection are plausible on mechanism, unproven on outcome.
Practical breakdowns are in the copper peptides guide, the GHK-Cu hair loss protocol write-up, and the GHK-Cu dosing chart.
Sermorelin (GHRH 1-29): the somatopause bet with the best older-adult data
The somatopause is real. GH pulse amplitude drops by roughly 50 percent between age 20 and age 60, and IGF-1 falls with it. That decline correlates with the loss of lean mass, the accumulation of visceral fat, and the collapse of slow-wave sleep that starts in middle age. Sermorelin, a GHRH analog covering the first 29 amino acids of native growth-hormone-releasing hormone, is the compound with the cleanest human trial data for pushing that axis back up in older adults.
Vittone et al. 1997 (Metabolism, PMID 9005976) is the anchor citation. Eleven healthy men aged 64 to 76 received 2 mg subcutaneous GHRH 1-29 nightly for six weeks. Nocturnal GH secretion increased 3-fold to 4-fold, IGF-1 rose by roughly 35 percent, and body composition markers moved in the right direction with a small trial size. The signal was clean enough that it framed a decade of follow-up work on GHRH analogs in aging.
Sermorelin is not FDA-approved for anti-aging. It is prescribed off-label by longevity clinics on the basis of the Vittone data and a series of open-label follow-ups, which is a real-world use case with a real (if modest) evidence base. The safety story is much better than exogenous growth hormone: GHRH analogs restore GH pulsatility rather than flatlining serum GH, IGF-1 stays in physiologic range in the published trials, and receptor desensitization limits runaway stimulation.
The reasonable framing is that sermorelin is a targeted intervention for age-related GH decline in adults over roughly 45, backed by controlled human data in older cohorts, with a mechanism that does not require overshooting IGF-1 into the range where cancer risk becomes a concern. It is not going to lengthen your telomeres or clear senescent cells. It is going to nudge the GH-IGF axis toward the range it occupied a decade earlier.
For the observational timeline data, see sermorelin before and after and the sermorelin dosing chart.
Thymosin alpha-1: the immunosenescence peptide with the most useful adjunct data
Thymosin alpha-1 is a 28-amino-acid peptide originally isolated from thymic tissue. Its mechanism is T-cell modulation: it enhances dendritic cell function, restores blunted vaccine responses, and rebalances Th1/Th2 signaling. Immunosenescence, the age-related decline of adaptive immunity, is one of the clearest measurable aging phenotypes, and thymosin alpha-1 sits closer to it than any other peptide on this list.
The evidence tier is B, not A, because thymosin alpha-1 has never been trialed as a general anti-aging drug. It has been trialed as an influenza vaccine adjuvant in elderly patients, which is the closest published proxy for a longevity endpoint. Ershler et al. 2007 (Ann NY Acad Sci, PMID 17600281) summarized four randomized double-blind trials in elderly adults where thymosin alpha-1 co-administered with influenza vaccine improved antibody seroconversion and antibody titers versus vaccine alone. That is a specific, measurable win against a defined age-related decline (poor vaccine response), on a peptide with a decades-long safety record and FDA orphan-drug approval for another indication.
Regulatory status matters here. Thymosin alpha-1 is approved in more than 30 countries under the brand name Zadaxin for chronic hepatitis B and as adjunctive cancer support. It is not FDA-approved in the United States for any indication, which affects legal access.
What the data does not show: thymosin alpha-1 has not been proven to extend lifespan or reverse thymic involution in humans. It has been shown to partly restore T-cell response in a specific immunosenescence context (vaccine response in the elderly). That is a real result and a real limit at the same time.
MOTS-c: real mechanism, mostly mouse evidence, one interesting human observation
MOTS-c is a 16-amino-acid peptide encoded within the mitochondrial genome itself, discovered by Changhan Lee and Pinchas Cohen's group at USC. It acts as a mitochondrial-derived hormone: circulating MOTS-c levels fall with age, and administration in preclinical models improves insulin sensitivity and metabolic function. Mechanistically it is one of the cleanest aging peptides on the list.
The mouse data anchor is Lee et al. 2015 (Cell Metabolism, PMID 25738459). MOTS-c injection in mice improved glucose tolerance, prevented diet-induced obesity, and restored insulin sensitivity on hyperinsulinemic-euglycemic clamp. The follow-up Reynolds et al. 2021 (Nature Communications, PMID 33473109) added the most important human data point: acute cycling exercise in 10 young men increased MOTS-c mRNA in skeletal muscle biopsy roughly 12-fold and circulating MOTS-c 1.6-fold. That established MOTS-c as an exercise-induced mitokine in humans.
What is missing: no randomized trial of injectable MOTS-c in humans for any age-related endpoint. The exercise study measured endogenous MOTS-c response, not a drug effect. Everything sold on peptide sites as "anti-aging MOTS-c" is based on mouse data plus a plausible mechanism. That does not make the peptide worthless, but it puts it firmly in Tier B.
The full write-up with the exercise-mimetic framing is in the MOTS-c mitochondrial exercise peptide guide.
FOXO4-DRI: the senolytic with a beautiful mouse study and no human data
FOXO4-DRI is a peptide inhibitor designed to disrupt the FOXO4-p53 interaction inside senescent cells. Once that interaction is broken, senescent cells lose their apoptosis-resistance and self-destruct, without harming healthy neighboring cells. It is the highest-conviction senolytic peptide by mechanism.
The evidence base is Baar et al. 2017 (Cell, PMID 28340339), a landmark paper in which naturally aged mice treated with FOXO4-DRI showed reduced senescent cell burden, restored coat density, improved liver and kidney biomarkers, and better grip strength and running capacity. The paper is one of the most-cited results in the modern senolytic field.
That paper is also entirely in mice. There is no published randomized trial of FOXO4-DRI in humans for any endpoint. The compound is sold as a research chemical and used by biohackers, but every claim about human anti-aging effects is extrapolated from the Baar data. Dosing protocols circulating on forums are not derived from human pharmacokinetics, because those studies have not been done.
FOXO4-DRI sits at Tier C not because the science is weak. The mouse work is genuinely impressive. It sits at Tier C because there is no human trial data at all. The compound is a research tool that has been adopted for self-experimentation faster than the trial literature can catch up.
For a fair breakdown of what the mouse data does and does not support, see the FOXO4-DRI senolytic research write-up and the FOXO4-DRI dosing chart with the strict evidence caveats.
Epithalon (AEDG): the telomerase claim you should read carefully
Epithalon is the tetrapeptide Ala-Glu-Asp-Gly, the synthetic version of a peptide fraction extracted from bovine pineal glands. It is the flagship compound of Vladimir Khavinson's group at the Saint Petersburg Institute of Bioregulation and Gerontology, which has published on peptide bioregulators since the 1970s.
The strongest cell-culture citation is Khavinson et al. 2003 (Bull Exp Biol Med, PMID 12937682), which reported that epithalon induced telomerase activity in human fetal fibroblasts and enabled the cells to divide past passage 44, versus a control that stopped at passage 34. That is a genuinely striking in vitro result. The lifespan data comes from Anisimov et al. 1998 (Ann NY Acad Sci, PMID 9701766) and follow-ups: mice, rats, and Drosophila given epithalamin (the natural pineal extract) or synthetic epithalon lived 11 to 31 percent longer than controls.
One catch is the concentration of the evidence. Nearly every published trial of epithalon comes from one research group, in one language, over several decades. No independent Western randomized controlled trial has replicated the animal or human findings, and no regulatory agency has approved the compound. That is not necessarily a fatal problem, but it is a strong argument for treating the results as a single-lab hypothesis rather than settled science.
Legal status is also uneven. Epithalon is a Schedule I substance in some jurisdictions, unregulated in others, and typically sold as a research chemical. Any published human data is on the same single-group base as the mouse work.
Warning: Epithalon has a huge presence on longevity forums that is not proportional to its independent evidence base. The mechanism is interesting. The lab is prolific. The independent replication is thin. Read the Khavinson bioregulator evidence write-up and the epithalon telomerase deep dive for a more forgiving take on the same evidence base, and adjust your priors accordingly.
What actually holds up: the honest ranking
Stripped of the marketing:
- Topical GHK-Cu for photoaged skin. Multiple controlled trials, decades of data. Buy it. Use it.
- Elamipretide (SS-31) for mitochondrial diseases and, plausibly, mitochondrial aging endpoints once the ongoing Phase 2/3 trials read out. FDA-approved for Barth syndrome. The evidence is real but narrow. Do not extrapolate to healthy 30-year-olds.
- Sermorelin (GHRH 1-29) for adults over 45 with measurable IGF-1 decline. Real placebo-controlled elderly data. Modest effect size. Reasonable off-label use under clinician supervision.
- Thymosin alpha-1 as an adjunct in immunosenescence contexts, especially poor vaccine response in the elderly. Not a general longevity drug.
- MOTS-c, FOXO4-DRI, and epithalon are compounds with plausible aging mechanisms and mostly preclinical or single-group data. Interesting to watch. Not evidence-based to use as anti-aging drugs today.
That is a ranking a skeptical clinician would recognize. It is different from the ranking you get from a store selling all seven.
How to think about anti-aging peptide stacks
The instinct on longevity forums is to stack every compound on the list. The instinct is usually wrong. Every peptide on this list either has narrow indications or thin human data. Stacking them multiplies unknowns, not benefits.
A cleaner mental model:
- Skin pathway: topical GHK-Cu, plus retinoids and sunscreen (both of which have larger evidence bases than any peptide on this list).
- GH-IGF pathway: sermorelin, or CJC-1295 plus ipamorelin, in adults with documented age-related IGF-1 decline, under supervision.
- Mitochondrial pathway: elamipretide once trials in age-related indications read out. Until then, exercise and sleep quality remain the two highest-return inputs to mitochondrial function, well ahead of any peptide.
- Immune pathway: thymosin alpha-1 as an adjunct if you have a defined immunosenescence phenotype and a clinician to prescribe it.
The compounds outside those four lanes belong in the "watching" bucket, not the "using" bucket, unless you are comfortable being a data point in an uncontrolled experiment.
Where to actually source these
Research-grade versions of every peptide in this list are sold as laboratory reagents by a handful of established vendors. The verification question that matters is not which vendor has the best branding, but which one publishes third-party certificates of analysis you can match to your lot. Our full breakdown of vendor testing standards, COA quality, and independent lab results is the Ascension Peptides review, and the actual lab-test dataset behind those ratings lives in the public lab tests library. Ascension Peptides is the partner we trust for research-grade injectables including GHK-Cu, sermorelin, SS-31, and MOTS-c; the current promo is code ENHANCED for 50 percent off.
For adjacent evidence-tiered guides, see best peptides for sleep, which walks the same GH-axis mechanism from a different endpoint.
Disclaimer
This article is for research and educational purposes only. It is not medical advice, not a treatment protocol, and not an endorsement of self-experimentation with any compound discussed. Every peptide named here is either FDA-approved for a specific non-aging indication, prescribed off-label, or sold as a research chemical outside the standard drug approval pathway. None is approved by any regulatory agency as an anti-aging or longevity drug. Anti-aging claims made online almost always outrun the underlying evidence, and the tier assignments in this article reflect what the current published literature actually supports, not what a marketing page promises. Any decision to use these compounds, including for skin care, hormone-axis support, or immune modulation in older adults, should be made in consultation with a qualified clinician who can weigh individual risks, screen for contraindications, and monitor outcomes.