At a glance
- Allison 2023 liraglutide 3.0 mg pilot RCT (n=27, 17 weeks): primary outcome (binge episodes per week) was not significantly different from placebo (-4.0 vs -2.5, p=0.37).
- Same trial: weight loss was significant (5.2% vs 0.9%, p=0.005), and binge remission ran 44% vs 36% (not significant).
- Richards 2023 retrospective: semaglutide alone cut Binge Eating Scale scores by 7.9 points in 48 obesity-clinic patients; adding stimulants did not add benefit.
- Radkhah 2025 meta-analysis (5 studies, 182 patients): GLP-1 RAs reduced BES by 8.14 points and weight by 3.81 kg vs comparators.
- Lisdexamfetamine remains the only FDA-approved BED pharmacotherapy, based on two Phase 3 trials with about 770 adults (McElroy 2015 to 2016).
- Tirzepatide BED Phase 2 trials are recruiting; no controlled tirzepatide BED outcome has been published.
The headline trial missed its primary endpoint
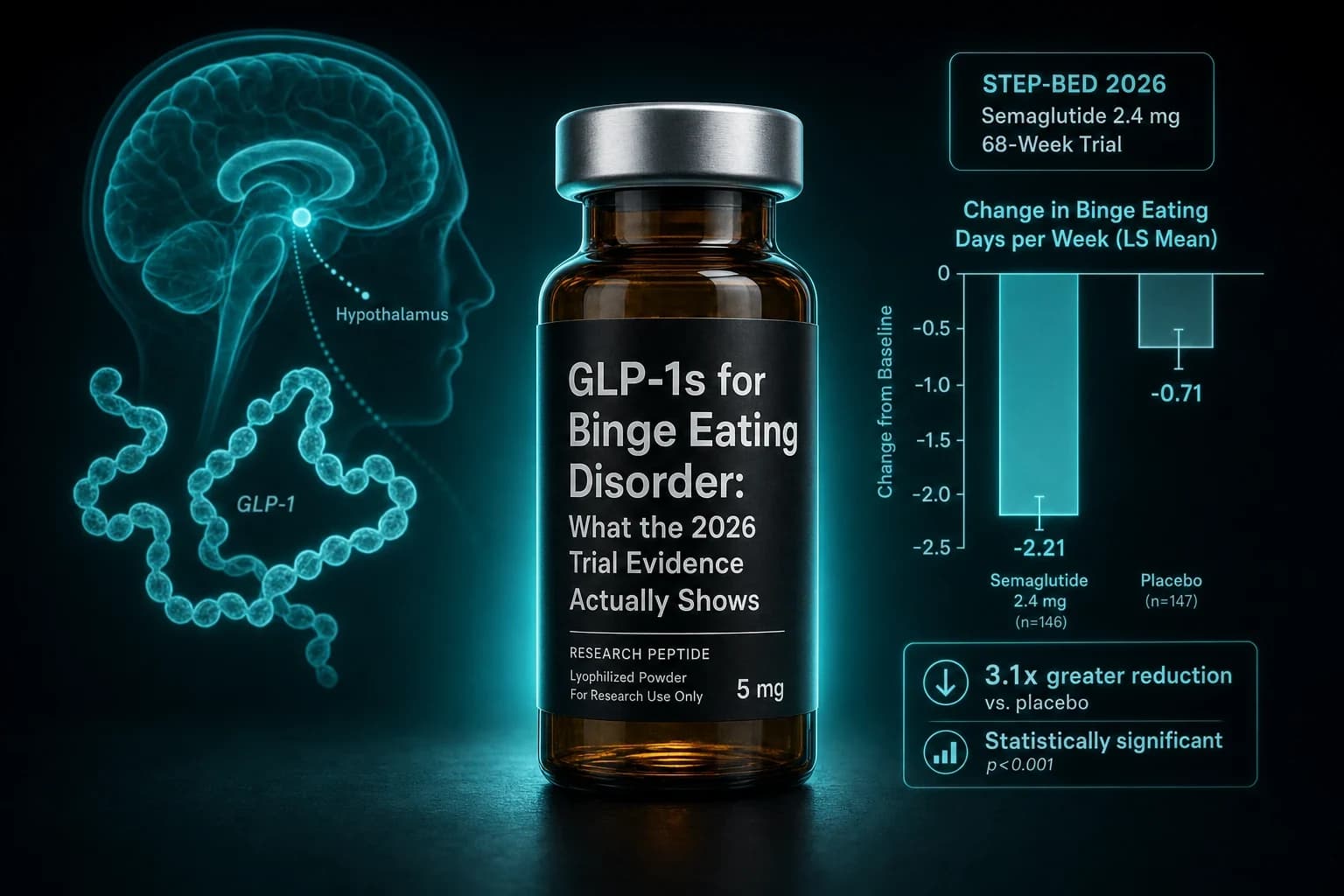
The Allison liraglutide pilot is the strongest controlled trial of a GLP-1 receptor agonist in binge eating disorder published to date. Twenty-seven adults with BMI of at least 27, randomized double-blind to liraglutide 3.0 mg daily or placebo for 17 weeks, with objective binge episodes per week as the primary outcome (Allison et al., Obesity Science & Practice 2023, PMID 37034559). The headline result that did not make the headlines: the liraglutide arm dropped 4.0 ± 0.6 binge episodes per week, placebo dropped 2.5 ± 0.5, and the between-arm difference was not statistically significant (p=0.37). Binge remission ran 44% on liraglutide and 36% on placebo, also not significant.
What did move was weight. Liraglutide produced 5.2% body weight loss versus 0.9% on placebo (p=0.005). That is the picture the field is working with: a small randomized trial in which weight loss reached significance but the binge eating primary outcome did not, sitting on top of a stack of open-label cohorts that report large reductions in Binge Eating Scale scores. Two years later, tirzepatide and semaglutide Phase 2 BED trials are recruiting but have not read out. So when a clinic, vendor, or telehealth ad tells you GLP-1s "treat binge eating disorder," the truthful response is: the strongest controlled trial did not show that on the primary endpoint, and everything else is hypothesis-generating.
Bottom line: GLP-1 receptor agonists consistently reduce Binge Eating Scale scores in open-label and retrospective work, but the only published randomized BED trial (Allison 2023, liraglutide 3.0 mg) missed its primary endpoint. Treat this as a signal, not a settled treatment.
This piece walks through what the controlled and observational data actually show, how the GLP-1 evidence compares to lisdexamfetamine (the only FDA-approved BED medication), what the mechanism story can and cannot carry, where the misuse risk in eating-disorder populations sits, and what the 2026 to 2027 trial readouts should clarify. For the closest sibling topic, see the GLP-1 alcohol cravings research breakdown. For the safety-signal context, see the GLP-1 mental health and suicidal ideation evidence guide.
Where the human BED evidence actually stands
The cleanest way to read the current literature is study by study, with the design intact. Four publications carry most of the weight, and a fifth is the FDA-approved comparator that everyone is implicitly measuring against.
| Study | Design | Compound | N | Primary BED outcome | Notes |
|---|---|---|---|---|---|
| Allison et al., Obesity Sci Pract 2023, PMID 37034559 | 17-week double-blind RCT | Liraglutide 3.0 mg daily | 27 adults, BMI 27+ | Objective binge episodes/week: -4.0 vs -2.5 placebo (p=0.37, NS) | Weight loss 5.2% vs 0.9% (p=0.005). BED remission 44% vs 36% NS. |
| Richards et al., Obes Pillars 2023, PMID 37990682 | Retrospective open-label cohort | Semaglutide alone vs semaglutide + LDX/topiramate vs LDX/topiramate alone | 48 obesity clinic patients (BES-defined BED) | BES reduction: -7.9 (sema), -8.8 (sema + other), -4.8 (other) | Combination did not beat semaglutide alone. No placebo. |
| Gong & Wentworth, Intern Med J 2024, PMID 39239945 | Single case report | Semaglutide for obesity + T1D with BED | 1 patient | Resolution of binge symptoms with semaglutide | Case-level, not generalizable. |
| Bartel et al., Int J Eat Disord 2024, PMID 38135891 | Narrative review of GLP-1 use across ED populations | All GLP-1 RAs | N/A | Synthesis only | Outlines opportunity and misuse concerns side by side. |
| Radkhah et al., Eat Weight Disord 2025, PMID 39891848 | Systematic review and meta-analysis | Mixed GLP-1 RAs | 5 studies, 182 participants | BES -8.14 points; weight -3.81 kg; both vs controls | Heterogeneous designs; mostly open-label inputs. |
| McElroy et al., Neuropsychopharmacology 2016, PMID 26346638 | Two 12-week Phase 3 RCTs (pivotal for FDA approval) | Lisdexamfetamine 50 or 70 mg/day | 383 + 390 adults with moderate-severe BED | Binge eating days/week significantly reduced vs placebo | The only FDA-approved BED medication. |
Reading those rows together is the entire story. The only modern randomized BED trial of a GLP-1 agonist did not reach its prespecified primary endpoint. The cohort and meta-analysis estimates show large BES reductions but rest on open-label data. The FDA-approved comparator is lisdexamfetamine, with a much larger randomized evidence base in this specific population. That asymmetry is what the 2026 Phase 2 tirzepatide and semaglutide BED trials are trying to close.
Reading the Allison liraglutide trial without spin
The Allison pilot enrolled 27 adults with BMI 27 or higher and DSM-5 binge eating disorder at the University of Pennsylvania. Participants were randomized 1:1 to liraglutide titrated to 3.0 mg daily (the Saxenda obesity dose) or matched placebo for 17 weeks, alongside standard clinical contact. The primary outcome was the change in objective binge episodes per week, the secondary outcomes included BED remission status, weight change, and psychosocial scales.
Key numbers worth holding onto:
- Objective binge episodes per week: -4.0 ± 0.6 on liraglutide versus -2.5 ± 0.5 on placebo. Mean difference 1.2 episodes per week (95% CI -1.3 to 2.0). p=0.37. Not statistically significant.
- BED remission: 44% on liraglutide versus 36% on placebo. Not statistically significant.
- Percent body weight loss at 17 weeks: 5.2 ± 1.0 on liraglutide versus 0.9 ± 0.7 on placebo. p=0.005.
- Both groups reduced binge episodes substantially from baseline, which is consistent with the well-documented placebo response in BED trials.
Two interpretive points matter. First, a 27-patient pilot is underpowered to detect anything but a very large between-arm difference on a noisy weekly count outcome. The authors framed the trial as hypothesis-generating, and the literature has carried it forward as a positive signal mostly because both arms moved and the weight loss outcome reached significance. Second, the placebo arm did the typical thing BED placebo arms do, which is improve substantially. That placebo response is the single most under-discussed feature of this field. Any sponsor running a Phase 2 BED trial in 2026 has to assume placebo will cut binge episodes by 40 to 60 percent on its own, and design accordingly.
What the Allison trial does honestly establish: liraglutide 3.0 mg produces clinically meaningful weight loss in adults with BED and obesity, on top of usual care. What it does not establish: that liraglutide specifically reduces binge episodes more than placebo, that the BED-specific symptom benefit holds beyond 17 weeks, or that semaglutide and tirzepatide will replicate any of this at their higher doses and longer half-lives. The Allison trial is the floor, not the ceiling, of the GLP-1 BED case.
What the Richards semaglutide cohort actually showed
The Richards et al. retrospective cohort is the closest thing the literature has to a semaglutide BED dataset (Richards et al., Obes Pillars 2023, PMID 37990682). Forty-eight adults attending an obesity and bariatric clinic in 2021 to 2022 met Binge Eating Scale criteria for moderate to severe BED, with three open-label treatment paths: semaglutide alone (n around 19), semaglutide plus lisdexamfetamine or topiramate (n=13), and lisdexamfetamine or topiramate alone (n=16).
BES reductions ran 7.9 points in the semaglutide-only group, 8.8 points in the combination group, and 4.8 points in the non-semaglutide group. Adding stimulants or topiramate to semaglutide did not produce a larger reduction than semaglutide on its own. The 7.9-point BES drop is in the same range as what trials of lisdexamfetamine and dialectical behavior therapy report in moderate to severe BED. That is the headline most coverage runs.
What the design cannot tell you: this was a retrospective chart review at a single obesity clinic. There was no randomization, no blinding, no placebo arm. Patients self-selected or were channeled by clinician preference into the three groups. The combination group was small. The follow-up window was the clinic's standard treatment course, not a fixed prespecified duration. None of that disqualifies the data; it just means the BES reductions cannot be attributed to semaglutide pharmacology with any confidence, and the absence of an advantage for combination therapy could reflect the small combination group as easily as a true ceiling effect.
The Richards cohort is best read as a hypothesis-confirming companion to the Allison RCT and the preclinical reward-circuit literature: semaglutide-treated BED patients in routine obesity-medicine practice report large symptom improvements that are not obviously inferior to lisdexamfetamine in the same clinic. Whether semaglutide would still come out ahead in a placebo-controlled, intention-to-treat randomized design is the open question the pending Phase 2 trials will answer.
The 2025 meta-analysis: how much further the field has moved
Radkhah et al.'s 2025 systematic review and meta-analysis is the first attempt to pool the GLP-1 eating-disorder evidence quantitatively (Radkhah et al., Eat Weight Disord 2025, PMID 39891848). It included five studies and 182 participants across BED and other disordered-eating populations, with mixed designs and mostly open-label inputs.
Pooled estimates ran:
- Binge Eating Scale: -8.14 points on GLP-1 receptor agonists versus controls
- Body weight: -3.81 kg (95% CI -5.14 to -2.49) on GLP-1 RAs
- BMI: -1.48 kg/m² on GLP-1 RAs
- Waist circumference: -3.14 cm on GLP-1 RAs
Only the BES effect size materially differs from what the underlying obesity-population GLP-1 literature would predict. Weight, BMI, and waist circumference all sit close to the kind of numbers you would expect from 12 to 24 weeks of liraglutide 3.0 mg or semaglutide 1.0 mg in any obese patient cohort. The 8-point BES drop is the extra slice that the pooled BED literature claims for the class.
One honest caveat: the meta-analysis inherits the limitations of its inputs. With 182 patients across five studies, no individual placebo-controlled randomized BED trial of semaglutide, and a heavy reliance on retrospective and uncontrolled designs, the pooled BES estimate is fragile. It is the right direction for the field to head, and it is not the kind of evidence the FDA or the BED treatment guidelines committees will treat as conclusive.
How this compares to lisdexamfetamine, the only approved BED drug
Lisdexamfetamine (Vyvanse) is the only medication FDA-approved for moderate to severe BED in adults. Approval came in January 2015 on the strength of two Phase 3 randomized, double-blind, placebo-controlled trials enrolling 383 and 390 adults respectively, both 12 weeks in duration (McElroy et al., Neuropsychopharmacology 2016, PMID 26346638). Dose-optimized lisdexamfetamine (50 or 70 mg/day) produced statistically superior and clinically meaningful reductions in binge eating days per week at weeks 11 to 12 across both trials. The treatment effect appeared as early as week 1.
That is the comparator standard. Two adequately powered Phase 3 trials, replicated, in the actual indication, with binge eating days per week as the primary outcome. The current GLP-1 BED literature is several orders of magnitude away from that quality bar, even if the open-label BES reductions look large.
The pragmatic decision-aid question for clinicians and informed patients is whether the off-label GLP-1 path is reasonable given the controlled-trial gap. The honest framing has several legs:
| Variable | Lisdexamfetamine (LDX) | Liraglutide 3.0 mg | Semaglutide 2.4 mg | Tirzepatide 5 to 15 mg |
|---|---|---|---|---|
| Approved for BED in US | Yes (since 2015) | No | No | No |
| Phase 3 RCT evidence in BED | Two pivotal trials, n approximately 770 | None | None published | None published; Phase 2 recruiting |
| Phase 2 / pilot RCT evidence in BED | Yes (dose-finding) | Allison 2023, n=27, primary endpoint NS | None published | None published |
| Weight loss impact | Modest (typically 4 to 6%) | 5 to 7% at full dose | 14 to 17% at full dose (STEP 1) | Up to 20%+ (SURMOUNT 1) |
| Cardiovascular outcome data | Stimulant safety profile, BP and HR caveats | LEADER positive | SELECT positive | SURPASS-CVOT positive |
| Schedule status | Schedule II (US) | Prescription only | Prescription only | Prescription only |
| Stop-and-restart pattern | Easy | Slow off-titration | Slow off-titration | Slow off-titration |
| Anti-binge mechanism | Catecholamine-driven appetite and impulse suppression | Mesolimbic GLP-1R activation + satiety | Mesolimbic GLP-1R activation + satiety | GLP-1R + GIP-R activation + satiety |
Bottom line: Lisdexamfetamine has the better controlled-trial evidence specifically for BED. GLP-1 receptor agonists have the better weight-loss and cardiovascular evidence in obese populations, and a plausible but not yet proven BED-specific signal. For a patient whose primary problem is binge eating with normal weight, the controlled evidence still points to LDX. For a patient whose primary problem is BED plus obesity plus cardiometabolic risk, the GLP-1 story is more defensible.
The mechanism story: real, but it does not carry the article alone
GLP-1 receptors are expressed in two locations that matter for binge eating biology. The first is the homeostatic appetite circuitry: arcuate nucleus, paraventricular nucleus, brainstem, and vagal afferents. That is the satiety axis that explains most of the food-intake reduction at obesity doses. The second is the mesolimbic reward circuitry: ventral tegmental area, nucleus accumbens, lateral septum, and hippocampus. GLP-1 receptor activation in those structures reduces operant responding for palatable food in rodents, reduces sweetened fat self-administration, and blunts dopamine release during reward consumption.
That preclinical signal is the same circuit that explains the GLP-1 effect on alcohol cue reactivity in the Klausen and Hendershot trials. The unified picture: GLP-1 agonism dampens hedonic reward across multiple consumed substances, with food, alcohol, and possibly other drugs of misuse all sharing overlapping mesolimbic substrates. That coherence is part of why the BED community has been willing to take small open-label studies seriously, even though the controlled evidence is still thin.
The mechanism is real and it explains the signal. It does not by itself establish clinical efficacy. The history of CNS pharmacology is full of compounds that look beautiful in mesolimbic circuit models and fail in randomized clinical trials. Until the Phase 2 BED tirzepatide and semaglutide trials read out with placebo arms and prespecified binge-day outcomes, the right way to weight the mechanism story is as plausibility, not proof.
When the GLP-1 path might fit and when it might not
For researchers and informed patients reading the literature in 2026, the practical question is whether to consider a GLP-1 protocol when BED symptoms and obesity coexist. The literature does not yet support a confident yes or no. What it does support is a structured set of conditional considerations.
| Profile | Reasonable approach |
|---|---|
| BED at normal weight, no metabolic risk | LDX has the controlled evidence. GLP-1 RAs do not have a clear case here, and rapid weight loss in a non-overweight patient adds risk without obvious benefit. |
| BED with class I obesity, otherwise healthy | LDX remains evidence-supported. A GLP-1 RA is a reasonable second-line consideration if LDX is contraindicated or not tolerated, with the caveat that BED-specific RCT evidence is limited. |
| BED with class II to III obesity, cardiometabolic risk | The weight-loss and cardiovascular case for a GLP-1 RA stands on its own. Any BED benefit is an additional reason to choose this path over phentermine or other older anti-obesity drugs. |
| BED with type 2 diabetes | Semaglutide or tirzepatide carry independent indications. The BED signal is a downstream consideration, not the primary indication. |
| BED with prior anorexia or bulimia history | Caution. The misuse signal in the case literature warrants close screening before any anti-obesity drug, GLP-1 or otherwise. LDX has its own misuse concerns. |
| Adolescent BED | Off-label use of GLP-1 RAs in adolescents has emerging trial coverage in obesity but not in BED specifically. Caution and specialist supervision are appropriate. |
Protocol design in the obese cardiometabolic-risk profile is best read against the GLP-1 dosing comparison guide, which walks through how the semaglutide 2.4 mg, tirzepatide 5 to 15 mg, and retatrutide titration schedules compare on tolerability. The GLP-1 muscle loss evidence guide covers the lean-mass preservation considerations that matter when weight loss is rapid. For reconstitution math on research vials, our reconstitution calculator handles the dose-by-volume conversion at the common vial sizes.
The other side: GLP-1s as a misuse vector in ED populations
The Bartel et al. 2024 review in the International Journal of Eating Disorders is the most cited synthesis of the eating-disorder-population concerns (Bartel et al., Int J Eat Disord 2024, PMID 38135891). The argument is straightforward: GLP-1 receptor agonists produce sustained appetite suppression and weight loss, which is therapeutic in BED and obesity, and which can be co-opted by patients with restrictive or purging eating disorders to deepen pathological patterns.
Published case reports describe patients with prior anorexia or bulimia obtaining GLP-1 prescriptions through obesity-medicine or telehealth channels, then using them to reignite restrictive cycles. The pattern is not specific to GLP-1s. Lisdexamfetamine, topiramate, and bupropion-naltrexone have similar misuse vectors. What is specific to the GLP-1 wave is the scale of access. With telehealth prescribing, compounded versions, and global research-vial markets, the population that could in principle obtain a GLP-1 RA without an obesity diagnosis is much larger than the population that could obtain Vyvanse without a controlled-substance prescription.
The clinical implication is screening, not blanket avoidance. The 2025 Bartel framework recommends an eating-disorder history at every GLP-1 obesity intake, with particular attention to childhood anorexia history, current purging behavior, and rapid intentional weight loss as red flags. The Gong 2024 case report sits on the therapeutic side of this same coin: a patient with BED and type 1 diabetes on semaglutide whose binge symptoms resolved alongside body-weight normalization (Gong & Wentworth, Intern Med J 2024, PMID 39239945). The same compound can do both depending on patient profile, so the clinical art is matching the path to the person.
What the 2026 trials should clarify
A Phase 2 tirzepatide BED trial currently recruiting on ClinicalTrials.gov is the most consequential pending readout for this question. The reported design includes a three-arm comparison: tirzepatide versus placebo versus lisdexamfetamine, with guided self-help cognitive behavioral therapy in all arms, and binge episodes per week as the primary outcome. A direct head-to-head against the FDA-approved comparator is exactly what the field needs.
Separately, a semaglutide BED Phase 2 trial is also in development. Together those trials should answer four questions that the current literature cannot:
- Does a higher-potency GLP-1 RA (semaglutide 2.4 mg, tirzepatide 10 to 15 mg) clear the BED-specific symptom bar that liraglutide 3.0 mg did not in the Allison pilot?
- Does it clear it in a placebo-controlled randomized design where the placebo response is the main confounder?
- Does it clear it independent of weight loss, or does the BED benefit track 1-to-1 with the body weight effect?
- Does it match or exceed lisdexamfetamine on binge-day reduction in a direct comparison?
If the answer to all four is yes, the field will have a credible second-line BED indication and the practice patterns will catch up within two to three years. If the answers are mixed, GLP-1 RAs will remain off-label adjuncts in BED-with-obesity profiles, and lisdexamfetamine will keep its monopoly on first-line drug therapy. The third possibility, where the BED outcome moves but tracks tightly with weight, would point to satiety and reduced food intake as the proximate mechanism, with the mesolimbic dopamine story doing less explanatory work than the preclinical literature suggests.
For broader context on the GLP-1 evidence in neuropsychiatric outcomes, see the GLP-1 mental health evidence breakdown and the semaglutide alcohol cravings research review. For the structural comparison among current and next-generation GLP-1 RAs, the tirzepatide vs semaglutide SURMOUNT-5 head-to-head covers the underlying potency differences that will likely shape any BED-specific effect size.
How a careful researcher should read this in 2026
Pulling the pieces together, the honest position is:
- The strongest controlled trial in this space showed weight loss but not binge eating reduction beyond placebo. The headline framing that "GLP-1s treat BED" overstates what the controlled evidence has shown.
- The open-label cohort work and a 2025 meta-analysis suggest meaningful BES reductions on GLP-1 RAs, but the design quality is not yet at the lisdexamfetamine standard.
- Mechanistically, the mesolimbic GLP-1 receptor story is coherent and shared with the alcohol use disorder signal. The mechanism is not by itself a clinical claim.
- For obese patients with BED and cardiometabolic risk, a GLP-1 RA is a defensible off-label choice with the caveat that the BED-specific evidence is preliminary and the weight-loss benefit is the primary justification.
- For normal-weight BED patients, the controlled evidence still points to lisdexamfetamine. GLP-1 RAs do not have a clear case here, and the misuse risk in ED-history populations is real.
- The 2026 to 2027 Phase 2 tirzepatide and semaglutide BED trials are the key pending readouts. The current open-label literature should not be confused with the kind of evidence those trials will eventually produce.
Sourcing options for researchers
If you are pursuing GLP-1 research outside of standard prescribing channels and you need vendors with published certificates of analysis, Ascension Peptides covers semaglutide, tirzepatide, and retatrutide research vials with code ENHANCED for 50% off. Limitless Biotech covers the oral and nasal end of the peptide space with code ENHANCED. Neither path is a substitute for clinician supervision in patients with a binge eating diagnosis, and BED is not a research-vial protocol. Use these sources for the obesity, longevity, and metabolic protocols where they fit, and pursue BED-specific care through obesity-medicine and eating-disorder specialists.
For protocol design and reconstitution math on injectable GLP-1 research compounds, the tirzepatide reconstitution chart and the semaglutide 5mg reconstitution chart cover the common vial-size math. The glp-1 dosing comparison walks through how the current and next-generation doses line up across compounds.
This article is for educational and research purposes only and is not medical advice. Binge eating disorder is a clinical diagnosis that requires individualized assessment, and pharmacotherapy choices depend on comorbidities, prior eating disorder history, cardiometabolic risk, and patient goals. Lisdexamfetamine (Vyvanse) is the only FDA-approved medication for moderate to severe BED in adults. Semaglutide (Wegovy, Ozempic), liraglutide (Saxenda, Victoza), and tirzepatide (Zepbound, Mounjaro) do not carry BED indications and any use for binge eating symptoms is off-label. Off-label use, compounded versions, and self-directed dosing are outside the trial evidence reviewed here. Consult a qualified eating-disorder or obesity-medicine clinician before starting, switching, or stopping any medication for BED.