At a glance
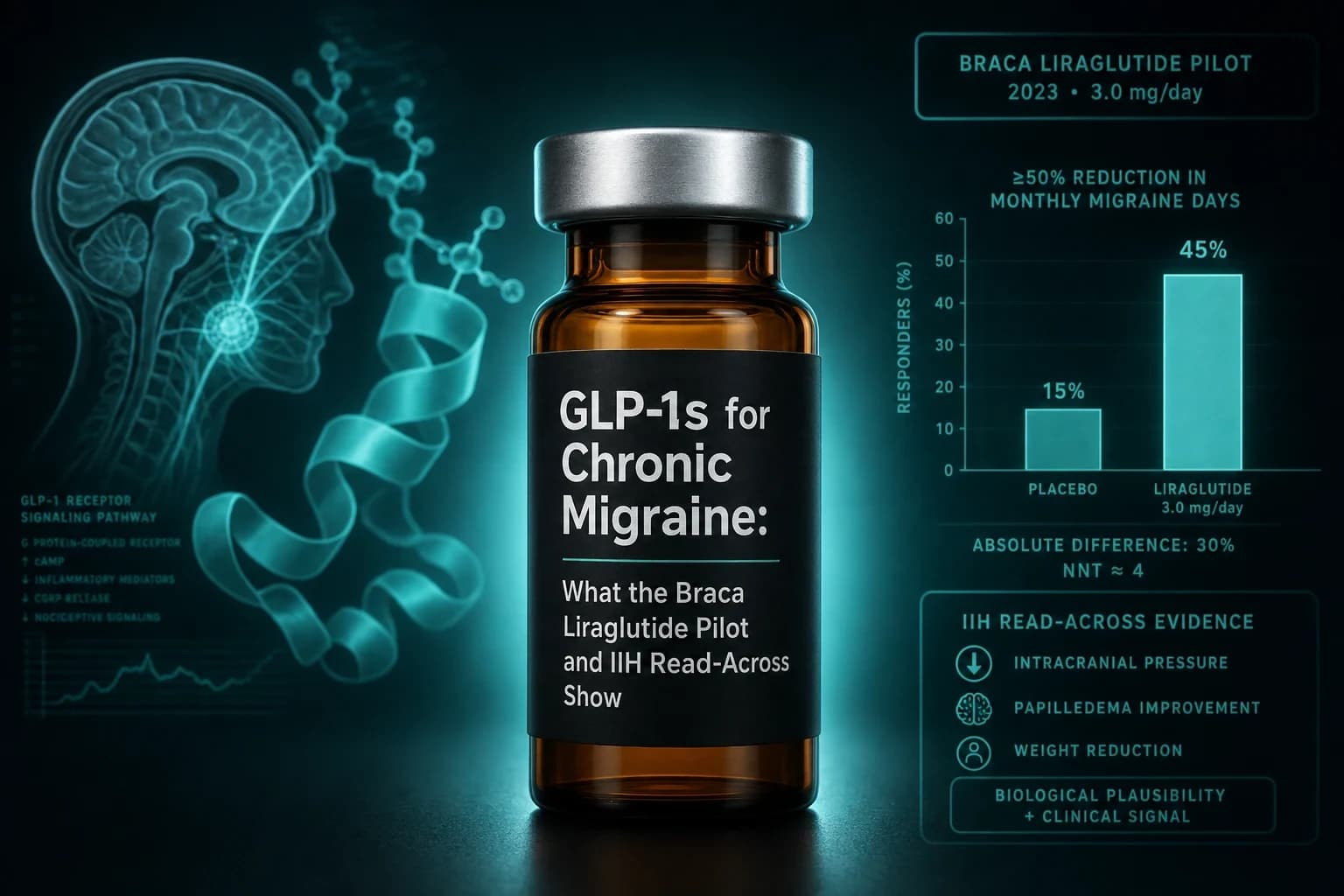
- Braca et al. 2025 (n=31, obesity plus refractory migraine, PMID 40525593): liraglutide 1.2 mg daily cut monthly headache days from 19.8 to 10.7 at week 12, p<0.001, Cohen's d 0.90
- About 45% of patients hit a 50% or greater reduction in monthly headache days; MIDAS disability scores dropped by more than half
- Weight loss during the 12 weeks was small and did not correlate with headache reduction, so the drug effect was not weight-mediated
- Jing et al. 2021 (PMID 34325647) mapped the mechanism: microglial GLP-1R activation in the trigeminal nucleus caudalis suppressed CGRP, c-fos, and PI3K/p-Akt in a nitroglycerin migraine model
- No GLP-1 receptor agonist is FDA-approved for migraine; this is one open-label pilot plus preclinical and IIH read-across, not proof of efficacy
Every migraine preventive that actually works either blocks CGRP directly or does something old and non-specific that the field kept because nothing better arrived. A 31-patient pilot out of the University of Naples put a diabetes drug into the same slot and cut monthly headache days almost in half. The compound was liraglutide, dosed at the type 2 diabetes strength of 1.2 mg. The result is small, open-label, and specific to patients with obesity. It is also the first prospective clinical signal that a GLP-1 receptor agonist may prevent migraine through a mechanism that has almost nothing to do with weight.
What the Braca pilot actually tested
The Braca group ran a single-center, prospective, open-label, interventional pilot (Braca et al. 2025, PMID 40525593) published in Headache. Enrollment ran January to July 2024. Eligibility was strict: adults with a body mass index of 30 or higher, high-frequency episodic or chronic migraine, and prior failure of at least two guideline-supported preventive treatments. All 31 participants (26 female, mean age 44.9) stayed on their prior preventive regimen. Liraglutide 1.2 mg subcutaneous daily was added on top for 12 weeks.
The primary endpoint was pre-specified as change in monthly headache days from a 4-week baseline diary to weeks 9 to 12. Secondary endpoints covered acute medication days, MIDAS disability score, HIT-6 impact score, and body weight. Tolerability and adverse events were tracked throughout.
Two design choices matter for interpretation. First, 1.2 mg is the type 2 diabetes dose, not the 3.0 mg obesity dose (Saxenda). It is a metabolic-strength daily dose, chosen because higher liraglutide doses produce more nausea during titration. Second, the trial had no placebo arm. The migraine field's known placebo response in preventive trials sits around 20% to 30% for the 50% responder endpoint, so a single-arm pilot cannot cleanly separate real drug effect from expectancy.
The 12-week results
| Metric | Baseline | Week 12 | Change | Statistical read |
|---|---|---|---|---|
| Mean monthly headache days | 19.8 | 10.7 | -9.1 days (95% CI 5.41 to 12.84) | p<0.001, Cohen's d 0.90 |
| 50% responder rate | not applicable | ~45% | not applicable | reported as the pre-specified secondary |
| MIDAS disability score | high | reduced by more than half | large drop | reported as significant |
| HIT-6 impact score | high | reduced | meaningful drop | reported as significant |
| Body weight | baseline | small mean decline | minor | not correlated with headache change |
Read that first row against the reference. A Cohen's d of 0.90 is a large effect size by any standard used in headache research. For context, the anti-CGRP monoclonal antibodies posted a -1.9 to -2.8 monthly migraine day advantage over placebo in their pivotal trials at similar 12-week reads. Braca's -9.1 day drop is a within-subject change, not a placebo-adjusted one, but the direction and magnitude are large enough that a chance finding is not the leading explanation.
The second row is the number the headache community actually looks at. Roughly 45% of patients achieved at least a 50% reduction in monthly headache days. That is the same responder threshold used to license erenumab, fremanezumab, galcanezumab, and eptinezumab. In a refractory population that had already failed two preventives, hitting 45% responder rate is the finding that made Nature run a news piece on the trial in July 2025.
The weight column is where the mechanism argument lives. Mean weight loss over 12 weeks was small, in line with what 1.2 mg liraglutide produces in non-diabetic adults. Correlation analyses in the paper did not find a relationship between kilograms lost and headache days dropped. That is not the same as proving weight loss is irrelevant, but it does rule out weight loss as the primary explanation for the effect within this window.
Bottom line: In 12 weeks, on a diabetes-strength daily dose, liraglutide cut monthly headache days almost in half in refractory migraine patients with obesity. The pilot is open-label and single-arm. The effect size is large, and it is not accounted for by weight change.
Why the mechanism matters
Modern migraine biology runs through calcitonin gene-related peptide (CGRP). The gepants (rimegepant, atogepant, ubrogepant) block the CGRP receptor. The monoclonal antibodies (erenumab, fremanezumab, galcanezumab, eptinezumab) neutralize the peptide or its receptor. Both classes work at or near the peripheral trigeminovascular system. Neither touches central sensitization mechanisms directly.
The preclinical case for GLP-1 receptor agonists working upstream of CGRP came from Jing and colleagues (Jing et al. 2021, PMID 34325647) in the Journal of Headache and Pain. They ran a repeated nitroglycerin injection model in mice, which is the standard preclinical chronic migraine model because nitroglycerin reliably induces central sensitization and CGRP release. Three findings:
- GLP-1R protein expression rose in the trigeminal nucleus caudalis after repeated nitroglycerin.
- Liraglutide administration reduced basal mechanical allodynia (a measurable proxy for central sensitization).
- Liraglutide suppressed CGRP, c-fos, and PI3K/p-Akt signaling in the trigeminal nucleus caudalis, and this suppression tracked microglial GLP-1R activation.
The translated read: GLP-1 activation in the central migraine circuit reduces CGRP release upstream of where the mAbs and gepants work. If the Braca signal replicates, that would be the first mechanistically distinct migraine preventive class since the CGRP era began. That is a big "if" and belongs in the "watch phase 3" column, not the "prescribe today" column.
Braca's paper anchored the mechanistic discussion on Jing and on the pressure-lowering data described next. The authors did not run their own CGRP or intracranial pressure sub-study, so the mechanism claim is one step removed from their patient-level data.
The IIH read-across
Idiopathic intracranial hypertension is not migraine. It is a distinct clinical entity: elevated intracranial pressure with papilledema and headache, mostly in women with obesity. But the headache phenotype in IIH overlaps clinically with migraine often enough that neurologists treat both conditions with several of the same drugs.
The IIH Pressure trial (Mitchell et al. 2023, PMID 36907221) in Brain was the first randomized, placebo-controlled test of a GLP-1 receptor agonist in IIH. Sixteen women received subcutaneous exenatide or placebo. Exenatide significantly lowered telemetrically measured intracranial pressure at 2.5 hours (-5.7 cmCSF, p=0.048), at 24 hours (-6.4 cmCSF, p=0.030), and at 12 weeks (-5.6 cmCSF). The headache secondary was also positive: exenatide arm patients had 7.7 fewer monthly headache days at 12 weeks; placebo arm patients had 1.5 fewer.
That trial matters for the migraine question in two ways. First, it establishes proof of concept that GLP-1 receptor engagement in a headache-relevant patient population reduces headache frequency by a clinically meaningful margin. Second, it identifies a plausible second mechanism: intracranial pressure lowering, which some migraine investigators have long argued could explain part of the migraine-obesity overlap.
Two phase 3 exenatide trials in IIH are enrolling. For the deeper IIH story, our GLP-1 IIH evidence review walks through the full 2026 dataset.
The systematic-review view
Halloum and colleagues (Halloum et al. 2024, PMID 38997662) published a systematic review in the Journal of Headache and Pain covering 42 studies of GLP-1 receptor agonists in headache and pain disorders. The review split findings into four buckets: inflammatory pain and osteoarthritis, headaches, neuropathic pain and diabetic neuropathy, and visceral pain and irritable bowel syndrome.
The headache bucket at that time (mid-2024) held IIH data and preclinical migraine work. The reviewers flagged primary migraine as the most methodologically compelling next indication for prospective trials. Braca 2025 arrived one year later and fit the prediction, which is what happens when a field moves in the direction its systematic reviews say it should.
The obesity-migraine confounder, honestly
Obesity is an independent risk factor for chronic migraine. A meta-analysis by Ornello et al. 2015 (PMID 25903159) in the Journal of Headache and Pain documented the association across 11 studies: obese subjects have a higher risk of chronic migraine than normal weight subjects, and pre-obese patients sit in between. Bigal and Lipton's earlier work established the dose-response with BMI.
Two implications for Braca. First, in the long run, losing enough weight might reduce migraine days independently of any direct central effect. Braca's 12-week window is too short and the weight change too small to see that pathway operate. Second, the fact that weight loss was small and did not correlate with headache change in Braca actively argues against the weight-mediated hypothesis for the pilot's specific results. A longer trial with meaningful weight loss would face the opposite problem: two overlapping mechanisms would be impossible to fully separate without a weight-matched control.
Where GLP-1s would sit if this replicates
| Class | Where it acts | Approved for migraine | Best evidence | Where GLP-1 sits |
|---|---|---|---|---|
| Anti-CGRP mAbs (erenumab, fremanezumab, galcanezumab, eptinezumab) | Peripheral CGRP peptide or receptor | Yes | Multiple phase 3 | GLP-1 would work upstream if Jing 2021 replicates |
| Gepants (rimegepant, atogepant, ubrogepant) | Peripheral CGRP receptor, oral | Yes | Multiple phase 3 | GLP-1 would work upstream of the same target |
| Topiramate, propranolol, amitriptyline | Various CNS mechanisms | Yes (topiramate, propranolol) | Older RCTs | GLP-1 has a cleaner mechanism story |
| OnabotulinumtoxinA (Botox) | Peripheral neurotransmitter release | Yes (chronic migraine only) | PREEMPT trials | Different anatomy, different indication overlap |
| GLP-1 receptor agonists | GLP-1R activation in trigeminal circuit and possibly ICP lowering | No | 1 open-label pilot, 1 IIH RCT, preclinical | Speculative fourth-line, class-effect unproven |
The comparison is not "GLP-1 vs the mAbs." The realistic slot, if any of this replicates in phase 3, is a fourth-line preventive for the subset of migraine patients who also have obesity and have failed two or more first-line preventives. That is exactly the Braca population.
Practical questions the pilot does not answer
Does semaglutide or tirzepatide work the same way? Braca used liraglutide specifically. Semaglutide and tirzepatide share GLP-1 receptor agonism but differ on half-life and, in the case of tirzepatide, on GIP receptor activity. No prospective migraine trial has tested them. A class effect is mechanistically plausible; that is not the same as evidence.
What dose applies? Braca used 1.2 mg subcutaneous daily. That is the diabetes dose, not the 3.0 mg obesity dose. If the mechanism is genuinely GLP-1R activation at the trigeminal nucleus caudalis, then the 3.0 mg obesity dose or the 2.4 mg semaglutide dose could plausibly do more. That question has not been tested. For a full mapping of liraglutide doses across indications, our liraglutide vs semaglutide comparison walks through Victoza vs Saxenda vs Wegovy.
Would microdosing work? Untested for migraine. Some research users are already tracking anecdotal headache changes on lower semaglutide and tirzepatide doses for weight loss; see the GLP-1 microdosing evidence for what the current data supports. Migraine microdosing has not been formally studied.
What about mood changes? GLP-1s have been separately studied for depression and suicidal ideation signals, and the mixed evidence is worth understanding before adding one to a migraine-plus-comorbidity picture. See the GLP-1 mental health review.
What about GI side effects during titration? The Braca pilot reported an adverse event profile in line with prior liraglutide safety data: mostly mild to moderate GI symptoms during titration, no serious safety signals. Patients starting liraglutide for migraine would face the same titration reality as patients starting it for diabetes. The GLP-1 dosing comparison covers titration schedules across the class.
What the pilot did not answer
Five gaps deserve to be named rather than glossed:
- No placebo arm. Migraine has a documented placebo effect for preventive endpoints. Without a control, the 45% responder rate cannot be cleanly attributed to drug effect versus expectancy plus regression to the mean.
- Twelve weeks is short. Anti-CGRP mAbs and gepants are licensed on 24-week to 52-week endpoints for durability reasons. Whether the Braca effect holds at 24 or 52 weeks is the next question.
- Single center, small n. Thirty-one patients in Naples. Replication in a different setting is a hard requirement before treating the effect as real.
- Refractory obesity phenotype only. The results may not generalize to normal-weight patients or first-line preventive use. Braca herself framed this population as the appropriate target for the follow-up.
- No mechanism sub-study. CSF pressure was not measured. Serum CGRP was not measured. Trigeminal ganglion imaging was not done. The mechanism argument is imported from Jing 2021 and from Mitchell 2023, both of which are separate patient or animal populations.
What to watch through 2028
- Phase 3 exenatide trials in IIH are enrolling and will read out in the next 2 to 3 years. Positive results would strengthen the pressure-lowering component of the migraine story.
- A placebo-controlled Braca successor has been signaled but not registered on clinicaltrials.gov as of mid-2026. That trial, if it enrolls, would be the first randomized read on GLP-1 for primary migraine.
- Semaglutide or tirzepatide migraine sub-studies. No manufacturer has announced one. Investigator-initiated retrospective cohorts from patients already on GLP-1s for weight loss will probably arrive first.
- CGRP measurement sub-studies. Direct measurement of plasma CGRP change on liraglutide would materially strengthen the mechanism claim beyond the Jing preclinical read.
Where to source research-grade GLP-1s
Braca dosed pharmaceutical liraglutide. For researchers tracking the class-effect question with reference-grade compounds, Ascension Peptides supplies research-grade semaglutide and tirzepatide with third-party lab COAs; code ENHANCED runs 50% off injectables. The reconstitution calculator handles the mg-to-IU math across every vial size these vendors ship, which matters more than most people expect once you drop from an obesity-strength dose to a diabetes-strength or microdose. None of that is a substitute for a licensed neurologist evaluating whether an off-label GLP-1 makes sense for a specific migraine case.
Tip: If you are already on a GLP-1 for weight loss and you also have migraine, keep a monthly headache diary starting the week you begin titration. That is how the retrospective cohorts of the next 24 months are going to be built, and your data will be more useful with a clean baseline.
The bottom line
The Braca 2025 pilot is the strongest single-trial signal to date that GLP-1 receptor engagement may reduce migraine days independently of weight. The pilot is open-label, single-arm, 12 weeks long, and limited to 31 patients with obesity and refractory migraine. The mechanism argument sits on solid preclinical work (Jing 2021) and on a well-designed but small IIH RCT (Mitchell 2023). The systematic review (Halloum 2024) predicted primary migraine as the next indication, and Braca fit that prediction.
None of that is proof. It is a strong hypothesis with three converging streams of evidence and no placebo-controlled clinical replication yet. The next 24 months will decide whether GLP-1s become a real fourth-line preventive for the migraine-plus-obesity phenotype or another intriguing pilot that failed to reproduce.
Research and educational purposes only. This article is not medical advice. No GLP-1 receptor agonist (liraglutide, semaglutide, tirzepatide, exenatide, or any next-generation candidate) is FDA-approved for migraine prevention. The Braca 2025 pilot is a single-center, open-label, uncontrolled study of 31 patients. The preclinical data is animal-model. The IIH data is from a separate clinical condition. GLP-1 receptor agonists carry class side effects including nausea, vomiting, delayed gastric emptying, pancreatitis signal, gallbladder events, and pre-procedural aspiration risk that are independent of any migraine question. Consult a neurologist or headache specialist before making decisions about migraine preventive therapy. Do not start, stop, or switch any GLP-1 receptor agonist on the basis of this article.