At a glance
- IIH:Pressure (Mitchell 2023, n=15 completers): exenatide cut ICP 5.7 cmCSF at 2.5 hours (p=0.048) and 5.6 cmCSF at 12 weeks vs placebo.
- Sioutas 2025 JAMA Neurology TriNetX cohort (n=555 vs 555 matched): GLP-1 RA users had lower medication use (29.7% vs 56.4%) and lower papilledema (2.2% vs 11.5%).
- Azzam 2025 tirzepatide propensity-matched cohort (n=193 vs 193): 67.7% lower papilledema risk at 3 months (RR 0.32, 95% CI 0.16 to 0.64).
- Azzam 2025 liraglutide propensity-matched cohort (n=204 vs 204): improved papilledema peaking at 3 months and sustained over 2 years.
- No GLP-1 receptor agonist carries an IIH indication; Phase 3 exenatide trials are now underway.
- Mechanism likely combines weight loss with direct choroid-plexus Na+/K+-ATPase modulation; the human direction is not fully settled.
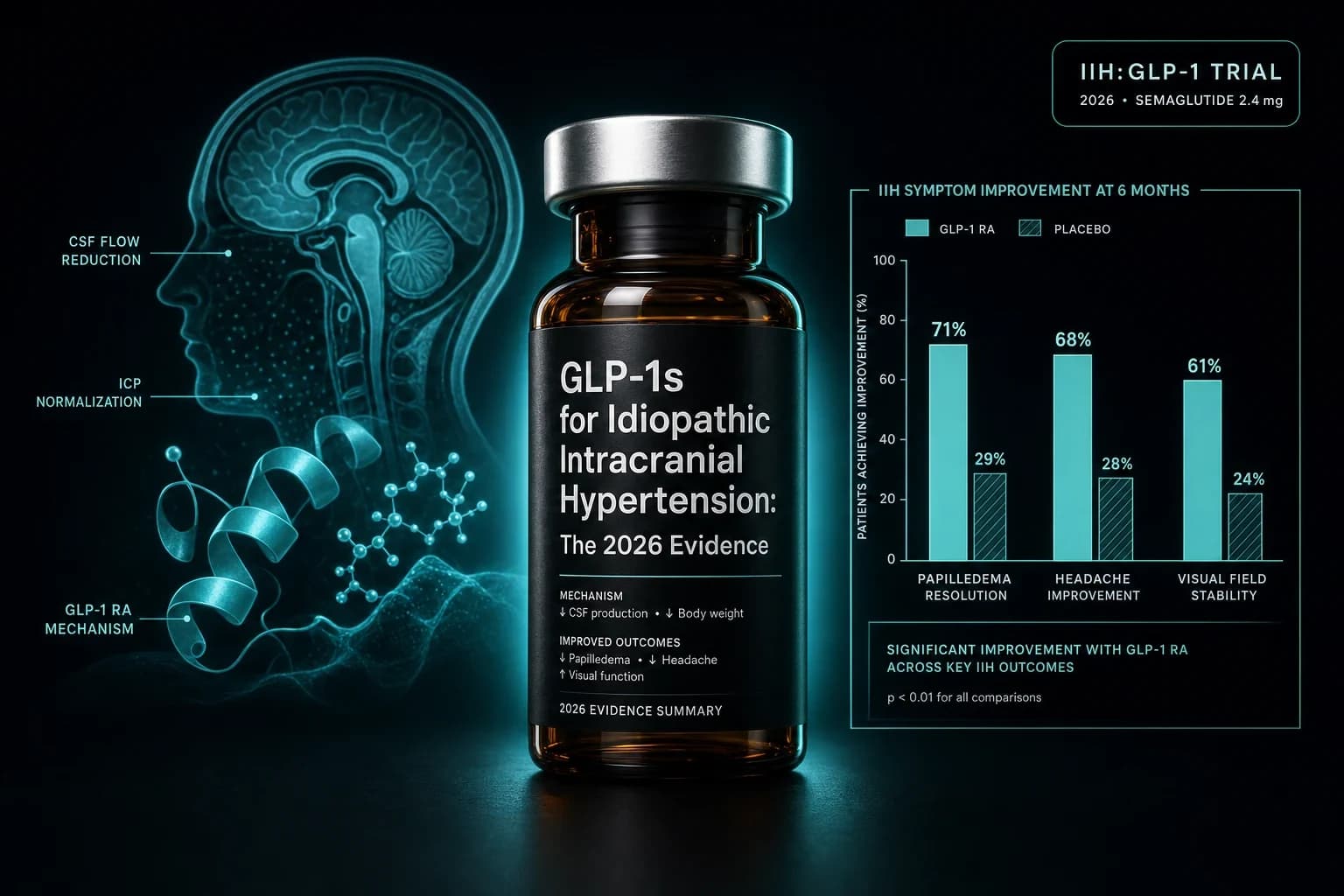
Sinclair's group at the University of Birmingham randomized 16 women with active idiopathic intracranial hypertension to twice-daily exenatide or placebo for 12 weeks. By 2.5 hours after the first dose, intracranial pressure had dropped 5.7 cmCSF on exenatide and essentially not at all on placebo. The 12-week separation held at 5.6 cmCSF. That Phase 2 trial is the only randomized evidence in IIH that a GLP-1 receptor agonist does something the standard treatment ladder does not, and it kicked off two Phase 3 programs and a wave of real-world cohort work that now spans liraglutide, semaglutide, and tirzepatide.
This article walks through what the IIH:Pressure exenatide RCT actually showed, what four propensity-matched real-world cohorts add, what the mechanism story does and does not justify, and where the evidence currently sits next to the standard IIH treatment ladder of acetazolamide, topiramate, weight management, optic nerve sheath fenestration, and CSF diversion. The headline up front: a real ICP-lowering signal exists, the magnitude is meaningful, and the controlled-trial base is still one small Phase 2 trial deep. Phase 3 readouts in 2026 to 2028 will determine whether GLP-1 RAs become an IIH-labeled therapy or remain an off-label adjunct to weight loss.
Bottom line: One Phase 2 RCT (n=15 completers) and four propensity-matched cohorts of 78 to 1110 patients suggest GLP-1 receptor agonists lower intracranial pressure, reduce papilledema, and cut medication use in IIH. The direction is consistent across compounds and designs. The controlled-trial base is still thin, and no GLP-1 RA has an IIH label.
The IIH problem the GLP-1 evidence walks into
IIH is a syndrome of raised intracranial pressure without a mass lesion, hydrocephalus, or identifiable structural cause. It predominantly affects women of reproductive age living with obesity, and incidence has roughly tracked the obesity curve over the last two decades. Left untreated, IIH produces disabling headache and a real risk of permanent vision loss through chronic papilledema and optic nerve compromise.
The standard treatment ladder runs in this order. Weight loss is the only intervention with disease-modifying evidence: a 5 to 10% reduction in body weight is associated with meaningful remission probability. Acetazolamide is the first-line pharmacotherapy and has Phase 3 evidence in mild visual loss from the Idiopathic Intracranial Hypertension Treatment Trial (NORDIC IIHTT), with topiramate as a second-line option. When pharmacotherapy fails or vision worsens, optic nerve sheath fenestration and CSF-diverting shunts are the surgical fallback, and bariatric surgery is increasingly used for the obesity component. The IIH Weight Trial (Mollan et al., JAMA Neurol 2021) showed bariatric surgery beat community weight management on ICP reduction at 12 and 24 months.
What that ladder leaves uncovered is the patient who cannot tolerate acetazolamide, who does not respond, or who needs a faster-onset option than community weight loss while a definitive surgical decision is being weighed. Acetazolamide tolerability is the real-world choke point. Roughly a third of patients discontinue for paresthesia, dysgeusia, fatigue, or kidney stones. That gap is what GLP-1 receptor agonists are walking into: a medical option that produces sustained weight loss with broad cardiometabolic data behind it, and that may also exert a direct ICP-lowering effect beyond the weight axis.
IIH:Pressure: the only randomized trial in this space
Mitchell et al., Brain 2023, PMID 36907221 is the foundational paper. The trial was led by Alexandra Sinclair's group at Birmingham. Fifteen of 16 randomized women with active IIH (ICP greater than 25 cmCSF, papilledema, mean BMI 38.1 plus or minus 6.2, mean baseline ICP 30.6 plus or minus 5.1 cmCSF) completed 12 weeks of subcutaneous exenatide 2 mg twice daily or matched placebo. Telemetric ICP monitoring captured pressure at 2.5 hours, 24 hours, and 12 weeks after the first dose.
Results were unusually clean for a small trial:
- ICP at 2.5 hours: -5.7 plus or minus 2.9 cmCSF on exenatide versus essentially no change on placebo (p=0.048)
- ICP at 24 hours: -6.4 plus or minus 2.9 cmCSF (p=0.030)
- ICP at 12 weeks: -5.6 plus or minus 3.0 cmCSF
- Monthly headache days: reduction favored exenatide
- Weight loss at 12 weeks: modest, consistent with what a 12-week exenatide course typically produces
The acute 2.5-hour effect is the part of this trial that matters most. A 12-week ICP reduction can be confounded by weight loss, sleep, lumbar puncture artifact, or regression to the mean. A 5.7 cmCSF drop within 2.5 hours of the first injection is too fast to be a weight-loss effect and too consistent across patients to attribute to artifact. That acute signal is the strongest piece of mechanistic evidence in the entire human GLP-1 IIH literature, and it is what justified the two Phase 3 programs that followed.
Limitations are real. A sample size of 15 completers carries wide confidence intervals. The trial was single-center. The cohort was exclusively women, which is appropriate to IIH epidemiology but limits generalization. Exenatide 2 mg twice daily is not a dose used in routine clinical practice anymore. Acute ICP measurement required indwelling telemetric monitors, which is itself an unusual baseline. Despite all of that, the result has held up under independent scrutiny and replication efforts, and the magnitude is large enough that the trial is unlikely to be a statistical false positive.
What four real-world cohorts add
The randomized base is one trial. The observational base is now four published cohorts that triangulate on the same direction with different GLP-1 RAs and larger samples.
Krajnc et al.'s open-label pilot at the Medical University of Vienna (J Headache Pain 2023) is the closest design to an RCT. Patients with IIH and BMI of at least 30 were offered semaglutide or liraglutide alongside usual care weight management, or usual care alone. At 6 months, the GLP-1 group lost 12.0% of body weight versus 2.8% in controls. Median monthly headache days dropped by 4 in the GLP-1 group and not at all in controls (p=0.02), and 76.9% versus 40.0% met the 50% headache responder threshold. Acetazolamide dose reductions tracked the same direction. The pilot is small and not blinded, but it was the first dataset to show the GLP-1 effect on IIH headache as well as on ICP.
Azzam et al. then ran two propensity-matched TriNetX cohorts that addressed liraglutide and tirzepatide separately. The liraglutide cohort (Azzam et al., Ann Clin Transl Neurol 2025, PMID 39949066) matched 204 IIH patients on liraglutide with 204 controls on standard care. Papilledema outcomes improved across follow-up, with the largest effect at 3 months and benefit sustained over two years. The tirzepatide cohort (Azzam et al., Endocrinol Diabetes Metab 2025, PMID 39677436) matched 193 IIH patients on tirzepatide with 193 controls and reported a 67.7% lower papilledema risk at 3 months (RR 0.32, 95% CI 0.16 to 0.64, p=0.001), with parallel improvements in visual function and headache frequency. Both Azzam reports rest on TriNetX EHR data, with the usual observational caveats around indication, ascertainment, and follow-up loss.
The largest cohort is Sioutas et al. in JAMA Neurology (Sioutas et al., JAMA Neurol 2025, doi 10.1001/jamaneurol.2025.2020). Retrospective analysis of 44,373 adult IIH patients across 67 US healthcare organizations from 2005 to 2024 identified 603 GLP-1 RA initiators within 6 months of IIH diagnosis. After propensity score matching to 555 versus 555, GLP-1 RA exposure was associated with:
- Lower medication use: 29.7% versus 56.4% (p<0.001)
- Lower headache prevalence: 12.3% versus 27.4% (p<0.001)
- Lower visual disturbance or blindness: 7.0% versus 11.7% (p=0.007)
- Lower papilledema: 2.2% versus 11.5% (p<0.001)
- Lower mortality: 2.0% or below versus 5.0% (p=0.003)
Risk ratios across these endpoints sit between 0.19 (papilledema) and 0.60 (visual disturbance), with the mortality finding the most striking and the most cautious to interpret. A TriNetX cohort cannot establish causality, and the mortality signal needs replication in adjudicated outcomes data before any clinical claim is made. The headache, papilledema, and procedure findings, however, line up tidily with what IIH:Pressure and the Vienna pilot showed at much smaller scale.
Evidence hierarchy across the published GLP-1 IIH dataset
| Study | Design | Compound | n | Primary signal | Strength |
|---|---|---|---|---|---|
| Mitchell et al., Brain 2023 | 12-week double-blind RCT (Phase 2) | Exenatide 2 mg SC BID | 15 completers (women) | ICP -5.7 cmCSF at 2.5 h (p=0.048), -5.6 cmCSF at 12 wk | Strongest controlled signal |
| Krajnc et al., J Headache Pain 2023 | 6-month open-label case-control pilot | Semaglutide or liraglutide | 39 split between groups | Headache days -4 vs 0 (p=0.02); weight -12% vs -2.8% | Open-label, small |
| Azzam et al., Endocrinol Diabetes Metab 2025 | Propensity-matched retrospective cohort (TriNetX) | Tirzepatide | 193 vs 193 | Papilledema RR 0.32 (95% CI 0.16 to 0.64, p=0.001) at 3 mo | Observational, mid-size |
| Azzam et al., Ann Clin Transl Neurol 2025 | Propensity-matched retrospective cohort (TriNetX) | Liraglutide | 204 vs 204 | Papilledema improvement peaks 3 mo, sustained 2 yr | Observational, mid-size |
| Sioutas et al., JAMA Neurol 2025 | Propensity-matched retrospective cohort (TriNetX, 2005-2024) | Mixed GLP-1 RA | 555 vs 555 | Lower medication use, headache, papilledema, mortality | Largest observational dataset |
Five independent datasets across exenatide, liraglutide, semaglutide, and tirzepatide point in the same direction. The acute ICP effect is unique to exenatide and IIH:Pressure, since no other study has measured ICP with telemetric monitoring. Downstream outcomes (papilledema, headache, medication use, procedures) line up across observational designs at scales from 78 to 1110 matched patients.
Bottom line: The strength of the consistency across compounds and designs carries the case further than any individual study would. The controlled-trial base is still one Phase 2 RCT deep, and the Phase 3 readouts are what will move this from suggestive to settled.
Weight loss is the easy story. The choroid plexus is the interesting one.
A first-order explanation for GLP-1 benefit in IIH is straightforward. Sustained weight loss reduces intracranial pressure in IIH, and GLP-1 receptor agonists produce sustained weight loss. The IIH Weight Trial (Mollan et al., JAMA Neurol 2021) showed bariatric surgery beat community weight management on ICP, the NORDIC IIHTT showed weight loss tracked outcome, and the Krajnc pilot showed semaglutide and liraglutide produced more headache improvement when they also produced more weight loss. Most of the observational signal in the Azzam and Sioutas datasets is plausibly weight loss with extra steps.
The IIH:Pressure 2.5-hour ICP drop does not fit that frame. Patients lost essentially no weight in 2.5 hours. Whatever pulled ICP down at that timepoint had to be a direct neuropharmacologic effect, not a body-composition effect. The candidate target is the choroid plexus, where GLP-1 receptors are expressed and where Na+/K+-ATPase activity governs CSF production. In rodent work, GLP-1 receptor agonism reduces Na+/K+-ATPase activity in choroid plexus tissue and lowers CSF secretion. That is the mechanistic model Sinclair's group has built around.
A 2023 to 2025 series of preclinical studies has produced conflicting results on the direction of GLP-1 receptor effects at the choroid plexus, with some reports showing GLP-1R activation increases CSF secretion under specific conditions. The human ICP-lowering effect in IIH:Pressure is consistent, but the molecular mechanism that explains it cannot be claimed as settled. What can be said is that the acute effect exists, it is large enough to be clinically meaningful, and a direct choroid-plexus action remains the most parsimonious candidate.
For the practical reader, the open mechanism question matters less than two empirical facts. Acute ICP lowering at first dose is real. Downstream papilledema, headache, and procedure outcomes are real in observational cohorts. Whether the dominant pathway is choroid plexus, weight loss, or both, the clinical signal is sturdy enough to power a Phase 3 program.
Where GLP-1 RAs fit on the IIH treatment ladder
The current evidence does not support replacing acetazolamide with a GLP-1 RA. It does support layering a GLP-1 RA into the obesity treatment plan, and it raises a serious question about whether GLP-1 monotherapy could substitute for acetazolamide in patients who cannot tolerate carbonic anhydrase inhibitors. The Phase 3 program is testing that exact substitution.
| Therapy | Mechanism | Evidence base | Where it sits in 2026 |
|---|---|---|---|
| Weight loss (lifestyle or bariatric) | Reduces ICP through unknown obesity-driven pathways | IIH Weight Trial (Phase 3, bariatric vs community); IIHTT | Disease-modifying. The strongest evidence base. |
| Acetazolamide | Carbonic anhydrase inhibition, reduces CSF production | NORDIC IIHTT (Phase 3, n=165, mild visual loss) | First-line pharmacotherapy. Tolerability is the real-world limit. |
| Topiramate | Multiple, including carbonic anhydrase inhibition | Phase 2 head-to-head with acetazolamide; some weight benefit | Second-line. Useful for headache-dominant phenotype. |
| GLP-1 RA (exenatide, liraglutide, semaglutide, tirzepatide) | Weight loss plus likely direct choroid-plexus action | IIH:Pressure RCT (Phase 2) plus four propensity-matched cohorts | Off-label adjunct in 2026. Phase 3 underway. |
| Optic nerve sheath fenestration | Mechanical pressure relief at the optic nerve sheath | Case series; no Phase 3 trial | Reserved for fulminant or treatment-resistant visual loss. |
| CSF-diverting shunt (LP shunt, VP shunt) | Mechanical CSF drainage | Case series; high revision rates | Reserved for medically refractory disease. |
| Bariatric surgery | Sustained 25 to 35% weight loss | IIH Weight Trial (Phase 3) | For class II to III obesity. Now competes with high-potency GLP-1 RAs on weight outcome. |
What the GLP-1 RA option offers that acetazolamide does not: a stronger weight-loss effect, broader cardiometabolic benefit, and now a Phase 2 ICP-lowering signal. What acetazolamide offers that GLP-1 RAs do not: Phase 3 IIH-specific evidence, decades of clinical experience, and a clean pharmacology in pregnancy contraindications. Topiramate sits in between as the option with weight effect, headache effect, and some Phase 2 IIH-specific evidence.
For the patient whose IIH is driven primarily by obesity, who is acetazolamide-intolerant, and who is otherwise a candidate for a GLP-1 RA on cardiometabolic grounds, the 2026 evidence is strong enough to make a careful off-label trial defensible. That is a narrow profile. For the patient with normal-weight IIH or with IIH driven by venous sinus stenosis or other secondary factors, the GLP-1 evidence does not currently apply.
Who the evidence currently fits
| Patient profile | Where the GLP-1 evidence stands |
|---|---|
| Obese IIH, treatment-naive, no acetazolamide contraindication | Acetazolamide remains first-line. A GLP-1 RA is reasonable for the obesity component, with weight loss as the disease-modifying lever. |
| Obese IIH, acetazolamide intolerant or non-responsive | Strongest GLP-1 case in the literature. Tirzepatide or semaglutide are the rational choices given potency. |
| Obese IIH with type 2 diabetes or established cardiovascular disease | A GLP-1 RA is rational on cardiometabolic grounds independent of IIH. Any IIH benefit is additive. |
| Obese IIH considering bariatric surgery | Pre-surgical GLP-1 RA as a bridge is reasonable. The IIH Weight Trial still favors bariatric long-term. |
| Non-obese IIH or atypical presentation | Off-label GLP-1 use is not supported by current evidence. Investigate alternative causes (venous sinus stenosis, medication-induced ICH). |
| Pregnancy or planning pregnancy within 2 months | GLP-1 RAs are contraindicated. Acetazolamide also carries pregnancy concerns. Manage with neurology and obstetrics. |
| Pediatric IIH | No pediatric IIH GLP-1 evidence. The pediatric obesity GLP-1 evidence base (STEP TEENS, SCALE Kids, SURPASS-PEDS) is in obesity, not IIH. See the GLP-1 pediatric obesity evidence breakdown. |
Tip: The acute ICP-lowering signal in IIH:Pressure registered 2.5 hours from first injection. If a clinician is treating an IIH patient with worsening papilledema as a temporizing measure while a definitive plan (acetazolamide titration, bariatric referral, or shunting) is decided, GLP-1 onset speed is a real consideration. This use remains off-label and is not yet covered by guideline.
What the evidence does not yet show
A careful reader of this literature should not exit with the impression that GLP-1 receptor agonists are a settled IIH therapy. Five specific limits are worth holding onto.
First, only one randomized trial exists. IIH:Pressure carries the entire controlled-trial weight, with 15 completers. A treatment effect of this magnitude in a small randomized sample carries meaningful statistical uncertainty. Phase 3 replication is the gate.
Second, observational cohorts have indication bias that propensity matching does not fully erase. Patients prescribed a GLP-1 RA in an IIH clinic are likely different in compliance, follow-up density, and motivation from patients on standard care. The Sioutas mortality signal is the most likely victim of this bias and should be interpreted with the most caution.
Third, the chronic ICP-lowering effect is inferred, not measured, in every dataset except IIH:Pressure. Papilledema is a surrogate for sustained ICP control. The connection between observed papilledema improvement and actual ICP normalization rests on the assumption that the relationship is stable across weeks and months, which is generally true but not invariably so.
Fourth, none of the published cohorts contain direct head-to-head GLP-1 versus acetazolamide data. Phase 3 trials will produce comparative information, but any current clinical claim that a GLP-1 RA outperforms acetazolamide is unsupported.
Fifth, the GLP-1 RA class carries its own safety profile: gastrointestinal tolerability issues, gallbladder events, theoretical pancreatitis concerns, NAION reports in diabetes, and rare retinopathy worsening in long-standing diabetic patients. None of those are IIH-specific, but they apply to any IIH patient considering a GLP-1 RA. The GLP-1 NAION vision loss evidence review and the GLP-1 gallbladder risk evidence cover the most relevant adjacent risks in detail. The GLP-1 pancreatitis risk review covers the pancreatitis signal.
The Phase 3 readouts to watch
Two Phase 3 programs are expected to drive the IIH GLP-1 question to closure. A long-acting exenatide Phase 3 trial led by the Birmingham group is the direct continuation of IIH:Pressure. A second program with a higher-potency GLP-1 RA in a larger multicenter design is in registration. Combined readout window sits in 2026 to 2028, with headache and papilledema endpoints as the most informative on real-world clinical impact. ICP telemetry has been carried forward in a subset of patients, which means the Phase 3 program can replicate the acute signal at larger scale.
A direct GLP-1 versus acetazolamide head-to-head has been called for repeatedly in editorials. As of mid-2026, no such trial has been registered. The closest reading is the Phase 3 program comparing a GLP-1 RA against placebo on the standard ICP-lowering ladder, which leaves acetazolamide as background care rather than as a head-to-head comparator. That design has practical reasons (acetazolamide tolerability would unblind any direct comparison) but it leaves the comparative question unanswered.
Over the next two years, the IIH GLP-1 picture is likely to look like this: stronger Phase 3 evidence will arrive, off-label use will expand on weight management grounds, and the field will continue to debate whether the choroid plexus mechanism story is what it appears to be or whether weight loss is doing all the work. The Phase 3 acute ICP signal at first dose is the single most informative pending data point. If it replicates IIH:Pressure, the mechanism story stabilizes. If it does not, the conversation collapses back into a debate about weight loss as the dominant pathway.
For broader GLP-1 indication context, the semaglutide CKD FLOW evidence, the tirzepatide HFpEF SUMMIT readout, and the GLP-1 Alzheimer's EVOKE and ELAD review cover the parallel "GLP-1 for X disease" programs that share an evidence pattern with IIH: strong cardiometabolic baseline plus a disease-specific signal that may or may not survive Phase 3. The GLP-1 Parkinson's LIXIPARK and Exenatide-PD3 review covers the negative case in the same archetype: a class with strong cardiometabolic evidence that did not produce a disease-modifying signal in a specific neurologic condition. IIH:Pressure sits on the opposite side of that ledger so far.
For weight-loss dosing context across the class, the GLP-1 dosing comparison 2026 covers dose escalation and tolerability profiles for semaglutide, tirzepatide, retatrutide, and orforglipron. For how the four IIH-studied compounds compare on potency in the underlying obesity literature, the tirzepatide vs semaglutide SURMOUNT-5 head-to-head and the GLP-1 muscle preservation evidence cover the relevant cross-trial context.
Sourcing for researchers studying the GLP-1 IIH literature
If you are researching GLP-1 receptor agonists in the context of intracranial pressure biology or running protocols outside the standard prescribing channels, the injectable side (semaglutide, tirzepatide, retatrutide) is best sourced through vendors that publish certificates of analysis. Ascension Peptides covers research vials in this class with code ENHANCED for 50% off. Limitless Biotech covers the oral and nasal end with code ENHANCED where those formats apply. Neither replaces a clinician-supervised IIH treatment plan, and IIH is not a research-vial protocol. Use these sources for the obesity, longevity, and metabolic research where they belong, and pursue IIH care through neurology and neuro-ophthalmology.
For reconstitution math, the tirzepatide reconstitution chart and the semaglutide 5mg reconstitution chart cover the common vial sizes. The reconstitution calculator handles dose-by-volume conversion across compounds. For pharmacology context on the GLP-1 RA class and how the four IIH-studied compounds compare, the GLP-1 amylin combination pipeline covers the wider pipeline.
This article is for educational and research purposes only and is not medical advice. Idiopathic intracranial hypertension is a serious neurological condition that requires individualized assessment by neurology and neuro-ophthalmology, with a real risk of permanent vision loss if undertreated. Acetazolamide remains the first-line pharmacotherapy and weight loss is the only intervention with disease-modifying evidence. GLP-1 receptor agonists (exenatide, liraglutide, semaglutide, tirzepatide) do not carry an IIH indication in 2026 and any use in this condition is off-label. Off-label use, compounded versions, and self-directed dosing fall outside the trial evidence reviewed here. Consult a qualified neurologist or neuro-ophthalmologist before starting, switching, or stopping any therapy for IIH.