At a glance
- Wang 2024 (PMID 38967919): in 1.65M T2D adults, GLP-1s vs insulin cut risk for 10 of 13 obesity-associated cancers, led by gallbladder (-65%) and pancreatic (-59%).
- Ko 2026 Annals systematic review (PMID 41359966): GLP-1s and dual agonists probably have little or no effect on thyroid, pancreatic, breast, or kidney cancer risk.
- Silverii 2025 50-trial RCT meta-analysis (PMID 40437949): overall cancer OR 1.05 (0.98-1.13); a uterine cancer reduction appeared only in obesity trials.
- Target-trial emulation in 85,015 adults (PMID 40450698): GLP-1 vs DPP-4i, HR 0.93 for obesity-related cancer over 3.9 years, with the strongest signal in colon and rectal cancer.
- ASCO 2026 real-world data (Orland, 12,112 patients) found GLP-1s linked to 38-50% lower stage IV progression in lung, breast, colorectal, and liver cancers vs DPP-4i.
The cancer question that will not go away
Every GLP-1 prescription comes with a question the prescriber rarely volunteers and the patient rarely asks out loud. If a drug remodels appetite, gut motility, insulin signalling, and adipose biology over years, what is it doing to cancer risk in tissues that respond to those same signals? The short version is that the rodent thyroid C-cell tumors that earned semaglutide and liraglutide their boxed warning have not translated into a clean human signal, and the more interesting story sitting underneath that finding is that the overall direction in the largest 2024 to 2026 cohorts points the other way.
Three things changed in the last 18 months. A 1.65 million-patient JAMA Network Open cohort tracked 13 obesity-associated cancers across 15 years of follow-up (Wang et al. 2024, PMID 38967919). A 50-trial randomized controlled trial meta-analysis was published in Diabetes, Obesity and Metabolism (Silverii et al. 2025, PMID 40437949). And the Annals of Internal Medicine ran a full systematic review of GLP-1 monoagonists and dual agonists in February 2026 (Ko et al. 2026, PMID 41359966). Pair those with the 85,015-patient target-trial emulation (PMID 40450698), the metformin-plus-GLP-1 synergy paper (Henney et al. 2026, DOI 10.1111/dom.70267), and the May 2026 ASCO real-world metastatic-progression abstract, and the evidence base for this question looks almost nothing like it did in 2023.
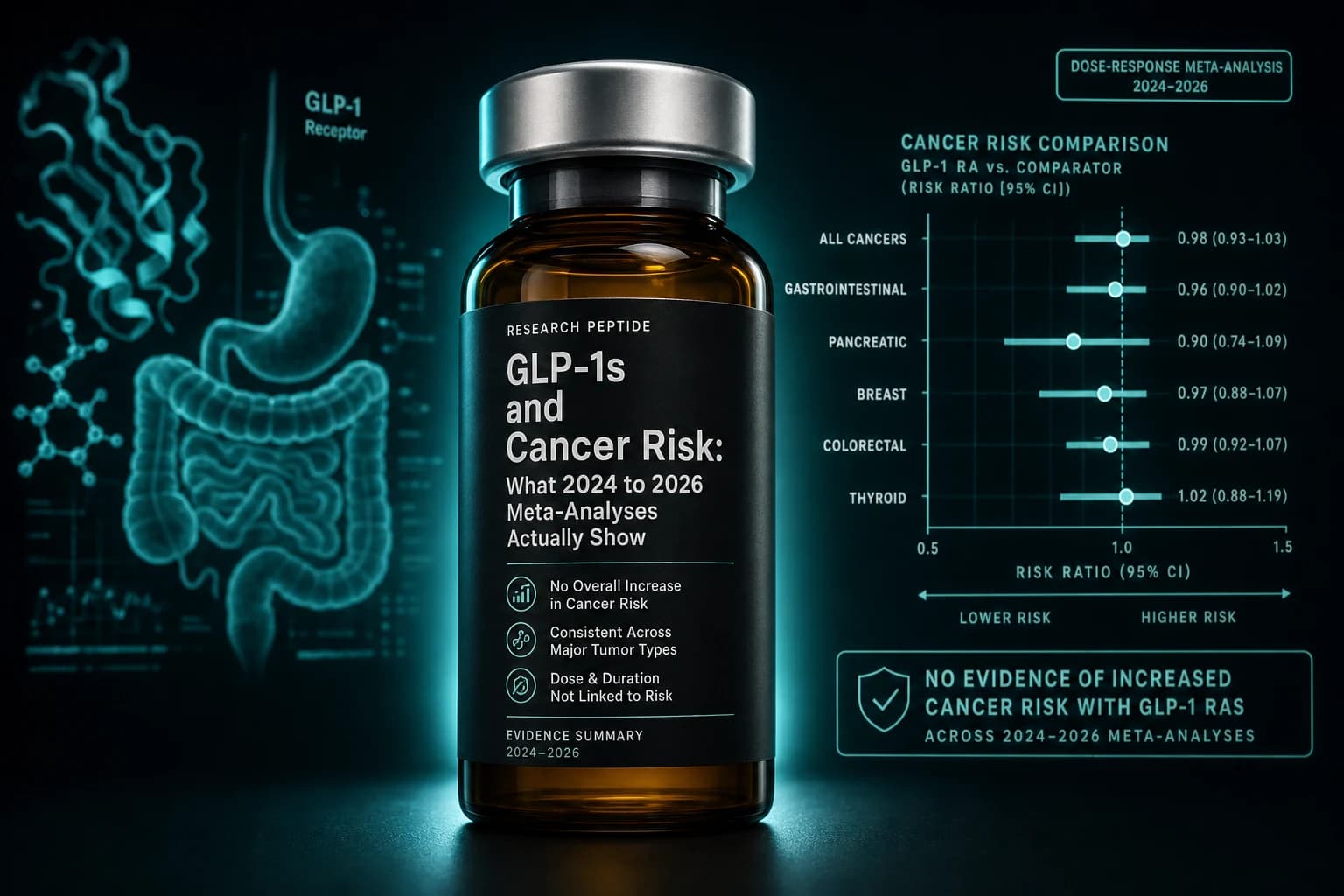
Bottom line: Across the largest 2024 to 2026 cohorts and meta-analyses, GLP-1 receptor agonists are not associated with an overall cancer signal. The strongest active-comparator studies point toward lower risk for several obesity-associated cancers, including colorectal, liver, pancreatic, and endometrial. The thyroid concern that lit up the early literature has not survived larger active-comparator analyses, and current best estimates put it at no detectable change.
Where the cancer worry actually came from
The boxed warning on semaglutide, liraglutide, dulaglutide, exenatide, and tirzepatide originated in rodents, not humans. Two-year rat carcinogenicity studies showed dose-dependent thyroid C-cell adenomas and carcinomas with GLP-1 receptor agonist exposure (Bjerre Knudsen 2010). Rats and mice express GLP-1 receptors on thyroid C-cells at higher density than humans, and the proposed mechanism, sustained calcitonin release driving C-cell proliferation, scales with that receptor density. The FDA accepted the rodent data as a signal worth a boxed warning while flagging the unclear translation to human medullary thyroid cancer.
That same setup produced a second class of concern around pancreatic cancer. Early case reports and adverse-event databases logged pancreatitis cases in GLP-1 users, and a hypothesized chronic pancreatitis to pancreatic adenocarcinoma sequence was reasonable enough to take seriously. The 2013 FDA and EMA reviews concluded that the available evidence did not support a causal link, but the question stayed open because every new pharmacovigilance dataset added more event counts. The third strand of concern, around medullary thyroid carcinoma in patients with MEN2 or a family history, is the one part of the rodent signal that translates cleanly into a clinical contraindication.
We covered the narrow thyroid question separately in our semaglutide thyroid cancer evidence review. The broader cancer landscape across all 13 obesity-associated tumor types is what the 2024 to 2026 cohorts actually let us see for the first time.
The Wang 2024 cohort that reset the conversation
The largest single dataset on this question is a TriNetX-based cohort study of 1,651,452 adults with type 2 diabetes prescribed GLP-1 receptor agonists, insulins, or metformin between March 2005 and November 2018 (Wang et al., JAMA Network Open 2024, PMID 38967919). Patients with prior diagnoses of any of 13 obesity-associated cancers were excluded at baseline. The follow-up window was 15 years. Outcomes were incident cancers across the obesity-associated set.
Compared with insulin, GLP-1 use was associated with significantly lower risk in 10 of the 13 tracked cancers. The reductions cluster in the gastrointestinal, hepatobiliary, and reproductive categories: gallbladder cancer fell 65 percent, meningioma 63 percent, pancreatic cancer 59 percent, and hepatocellular carcinoma 53 percent. Ovarian cancer dropped 48 percent, colorectal 46 percent, multiple myeloma 41 percent, esophageal 40 percent, endometrial 26 percent, and kidney cancer 24 percent. Thyroid, breast, and gastric cancers did not show statistically significant differences.
Two caveats matter. First, the comparator was insulin, and insulin itself carries an independent obesity-associated cancer association in the diabetes literature, which inflates the apparent benefit. Second, the GLP-1-versus-metformin comparison in the same dataset showed no consistent reduction. That second finding is the more honest read on what GLP-1s buy you on top of standard diabetes care: the Wang dataset is not saying GLP-1s cut cancer risk against the best background drug, only that they are clearly better than insulin in patients who could have been on something else.
The 2025 RCT meta-analysis: 50 trials, no overall signal
The randomized controlled trial evidence base was synthesized in 2025 by Silverii and colleagues at the University of Florence Diabetology Unit (Silverii et al., Diabetes Obesity and Metabolism 2025;27(8):4454-4468, PMID 40437949). The meta-analysis pulled 50 trials lasting at least 52 weeks that compared GLP-1 receptor agonists to any active or placebo comparator, in diabetes or obesity populations.
For overall cancer, the pooled odds ratio was 1.05 (95% CI 0.98 to 1.13). That confidence interval crosses one. The headline read is that across the cumulative trial-level evidence, there is no detectable difference in total cancer incidence on GLP-1 therapy compared with what those patients would have experienced on placebo or active comparators.
The site-specific findings inside that pooled non-result are where the texture lives. Thyroid cancer showed a non-significant numerical increase that became more pronounced in trials longer than 24 months, consistent with detection bias from thyroid imaging that often happens during trial follow-up. Colorectal cancer showed a small numerical increase that was significant only in shorter trials and disappeared in longer ones. Uterine cancer showed a significant reduction, but only in the obesity-trial subset, not the diabetes-trial subset.
Note: The Silverii pattern, where short-term and long-term subgroups disagree, is what detection bias usually looks like. When the screening intensity is highest at trial entry and the cancer-positive cases get pulled forward, you see a phantom increase early and a real null later. The same pattern showed up in the thyroid cancer evidence, where the Bezin 2023 French Insurance signal at one to three years did not survive longer active-comparator follow-up.
The 2025 target-trial emulation: GLP-1 vs DPP-4i, 85,015 patients
The cleanest active-comparator real-world signal comes from a target-trial emulation that compared GLP-1 initiators to DPP-4 inhibitor initiators in adults with type 2 diabetes and a body mass index of 30 or higher (target-trial emulation 2025, PMID 40450698). The cohort included 85,015 patients across 43 U.S. health systems between 2013 and 2023, with one-to-one propensity score matching on prescription year and baseline risk factors. The mean follow-up was 3.9 years.
The headline result was a hazard ratio of 0.93 (95% CI 0.88 to 0.98, p = 0.005) for obesity-related cancer incidence, and 0.92 (95% CI 0.87 to 0.97, p = 0.001) for all-cause mortality. The site-specific protective associations were strongest for colon and rectal cancers, consistent with both the Wang cohort and the Silverii subgroup findings. The DPP-4 inhibitor comparator is the right call methodologically. Both classes are second-line oral or injectable diabetes agents prescribed to similar patient profiles, which strips out the confounding-by-indication that distorts insulin comparisons.
The point estimate is small. A 7 percent relative reduction in obesity-related cancer over four years is real but modest. It is also exactly what you would expect from a class of drugs that produces 15 to 25 percent body weight reduction, given the established obesity-to-cancer dose-response.
The 2026 Annals systematic review: the most definitive read
The most rigorous single document on this question is the systematic review and meta-analysis published in Annals of Internal Medicine in February 2026 (Ko et al., Ann Intern Med 2026;179(2):216-229, PMID 41359966). The review pulled randomized placebo-controlled trials of GLP-1 monoagonists and dual agonists (GLP-1/GIP, GLP-1/glucagon, GLP-1/amylin) reporting cancer outcomes through August 2025. Predefined outcomes included thyroid, pancreatic, colorectal, gastric, esophageal, liver, gallbladder, breast, ovarian, endometrial, and kidney cancer, plus multiple myeloma and meningioma.
The review's conclusion is the cleanest summary statement currently in the literature: GLP-1 receptor agonists probably have little or no effect on the risk of thyroid, pancreatic, breast, or kidney cancer, and may have little or no effect on other obesity-related cancers, although certainty of evidence was low for most outcomes. The "probably" and "may" language is GRADE-system phrasing for confidence levels, not editorial hedging. Those are the strongest claims the evidence base currently supports.
The certainty-of-evidence ratings matter. Most outcomes were rated low or very low certainty because the trials were powered for metabolic endpoints, not cancer, and the event counts within any given trial are small. That is why the long-running cardiovascular outcome trials, which already enroll 10,000 to 18,000 patients for years, will give the next decisive read.
Cancer-by-cancer breakdown
| Cancer type | Wang 2024 (vs insulin) | Silverii 2025 (RCT meta) | Annals 2026 (GRADE) |
|---|---|---|---|
| Thyroid | No difference | No significant overall; ↑ in trials >24 months | Probably no effect (low certainty) |
| Pancreatic | -59% | No significant change | Probably no effect (low certainty) |
| Breast | No difference | No significant change | Probably no effect (low certainty) |
| Colorectal | -46% | Mixed (↑ short term, null long term) | May have no effect (very low certainty) |
| Liver (HCC) | -53% | No significant change | May have no effect (very low certainty) |
| Gallbladder | -65% | Not separately reported | Not separately reported |
| Endometrial | -26% | Not separately reported | May have no effect (very low certainty) |
| Ovarian | -48% | Not separately reported | May have no effect (very low certainty) |
| Kidney | -24% | No significant change | Probably no effect (low certainty) |
| Esophageal | -40% | No significant change | May have no effect (very low certainty) |
| Gastric | No difference | No significant change | May have no effect (very low certainty) |
| Uterine | Not separately reported | -42% (obesity trials only) | Not separately reported |
| Meningioma | -63% | Not separately reported | Not separately reported |
| Multiple myeloma | -41% | Not separately reported | Not separately reported |
Two patterns are worth flagging. First, the largest Wang cohort reductions cluster in the cancers most tightly coupled to obesity and chronic insulin resistance: gallbladder, pancreatic, liver, ovarian, endometrial. Second, the RCT meta-analysis is consistently more conservative than the observational cohorts, because RCTs by design have less follow-up time and smaller event counts.
The metformin synergy signal: Henney 2026
A separate question, also new, is whether combining a GLP-1 with metformin behaves differently from either alone. The Henney 2026 paper used TriNetX to compare three exposure groups (metformin alone, GLP-1 alone, and metformin plus GLP-1) against a DPP-4 inhibitor reference, with propensity score matching (Henney et al., Diabetes Obesity Metabolism 2026, DOI 10.1111/dom.70267). After matching, the cohort sizes were 88,786 (metformin), 112,735 (GLP-1), and 36,347 (dual).
Metformin alone showed a 4 percent reduction in adiposity-related cancer (HR 0.96, 95% CI 0.92 to 0.99) and a 22 percent reduction in mortality (HR 0.78, 95% CI 0.76 to 0.80). GLP-1 alone produced similar directional effects, and the dual exposure group showed the lowest cancer incidence of the three. The synergy claim is methodologically softer than the headline number, because dual users self-select into more aggressive treatment and tighter monitoring, but the directional consistency across all three exposures strengthens the underlying signal.
The clinical implication is the inverse of what most patients fear. Adding a GLP-1 to baseline metformin therapy does not appear to introduce an oncology risk that metformin was holding back. The combination, in this dataset, looked at least as good as either alone.
ASCO 2026: progression-stage data
The May 2026 ASCO Annual Meeting added a real-world abstract that addresses a different question: not whether GLP-1s prevent cancer, but whether patients already diagnosed at an earlier stage progress to metastatic disease at a lower rate on a GLP-1. Mark David Orland and colleagues at Cleveland Clinic's Taussig Cancer Institute pulled 12,112 TriNetX patients with stage I, II, or III breast, prostate, lung (NSCLC), colorectal, hepatocellular, renal cell, or pancreatic cancer, comparing GLP-1 users against DPP-4 users with propensity matching.
For four of the seven cancer types, patients on a GLP-1 were 38 to 50 percent less likely to develop stage IV disease than patients on a DPP-4 inhibitor: lung, breast, colorectal, and liver. Prostate, kidney, and pancreatic cancers did not show a statistically significant progression difference. The abstract is from a single database with the usual real-world confounders, and ASCO meeting abstracts have not gone through full peer review, so the appropriate read is "interesting signal worth replicating in active prospective work," not "confirmed metabolic-oncology benefit."
Tip: Real-world progression studies are useful exactly because clinical trials almost never enroll patients with existing untreated stage I to III cancer onto an obesity drug. If a class effect on metastatic progression exists, observational comparisons against another diabetes drug are likely to be the only feasible way to detect it for the next decade.
Where the evidence is genuinely weak
A few honest caveats. Most of the RCT trials run between 52 and 104 weeks. Solid tumor incidence is a long-tail outcome, and a four-year follow-up is short for cancers like prostate or breast that often take a decade to manifest. The observational cohorts have longer follow-up, but selection effects in who gets prescribed GLP-1s versus the comparator pull the estimates around in ways that propensity matching only partially corrects.
The dual and triple agonist evidence is thinner than the single agonist evidence. Tirzepatide (GLP-1/GIP), retatrutide (GLP-1/GIP/glucagon), and mazdutide (GLP-1/glucagon) all carry the same boxed thyroid warning, but the long-term oncology evidence for those molecules is a year or two behind semaglutide. The Annals 2026 review is the first to pull dual agonists into the same synthesis, and it explicitly notes lower certainty for that subset because the trial-level event counts are smaller.
The mechanism story is also genuinely incomplete. The cleanest mechanistic hypothesis is that GLP-1-driven weight loss reduces adipose-tissue-derived inflammatory drivers (IL-6, leptin, insulin) that promote cancer progression in obese tissue, with secondary contributions from improved glucose control and possibly direct GLP-1 receptor signaling on some tumor cells. The Tentolouris 2026 editorial in Diabetes Obesity Metabolism explicitly argues for dedicated randomized cancer-prevention trials in obesity, because the metabolic-oncology hypothesis is now strong enough that an "obesity intervention trial with cancer as primary endpoint" is finally a reasonable proposition.
What this changes for someone considering a GLP-1
If you are weighing semaglutide, tirzepatide, or one of the newer dual agonists against another option, the cancer landscape now looks closer to a small benefit than a meaningful harm. The exceptions are narrow but real:
- A personal or family history of medullary thyroid carcinoma or MEN2 is still a hard contraindication. The rodent C-cell mechanism is biologically conserved in those patients, and no human evidence has changed that calculus.
- Active gallbladder disease is worth flagging with the prescriber. The Wang cohort showed a gallbladder cancer reduction, but the same drug class also raises symptomatic gallstone events through rapid weight loss.
- Patients with prior pancreatic cancer or chronic pancreatitis are still excluded from most trials, and the existing safety data for that population is sparse.
For everyone else, the modern evidence does not support delaying or declining a GLP-1 on cancer-risk grounds. The bigger long-run questions are what happens to retatrutide and tirzepatide cancer outcomes once the cardiovascular outcome trials (TRIUMPH-CVOT, SURPASS-CVOT, SELECT) report decade-scale cancer outcomes as secondary endpoints. We covered the published SURPASS-CVOT results in our tirzepatide cardiovascular outcomes review and the SELECT MACE data in our semaglutide SELECT trial breakdown. The cancer secondary endpoints from those trials will be the next major shift.
The other practical context: the cancer discussion does not stand alone. The same patients are also weighing muscle and lean mass loss on GLP-1s, pre-surgery aspiration risk, vision-loss NAION reports, and mental health questions. The cancer literature is the part of the safety conversation that has shifted the most in the last 18 months, and the direction it shifted in was not the one the early signal suggested.
Bottom line: Across 1.6 million patients in cohort data, 50 RCTs in meta-analysis, an 85,000-patient active-comparator emulation, and a 2026 Annals systematic review, GLP-1 receptor agonists are not associated with overall cancer risk. The cleanest signals point toward modest reductions in obesity-associated gastrointestinal, hepatobiliary, and reproductive cancers. The thyroid C-cell rodent finding has not translated into a detectable human signal. Medullary thyroid cancer history remains the one hard contraindication.
Where to learn more
For deeper dives on the safety topics the cancer discussion touches, our semaglutide and thyroid cancer evidence audit covers the rodent-to-human translation argument in detail. The GLP-1 mental health 2024-2026 review covers a parallel "early signal that did not survive larger active-comparator analysis" story. Our semaglutide page, tirzepatide page, and retatrutide page carry the compound-specific safety summaries and dosing references.
For the broader pipeline context, the GLP-1 plus amylin combinations 2026 guide and the pemvidutide MASH Phase 2b evidence cover the next-generation molecules whose long-term safety, including cancer outcomes, the field is now actively setting up to track.
Researchers exploring GLP-1 protocols can source semaglutide and tirzepatide for research-only use from Ascension Peptides with 50% off using code ENHANCED.
Disclaimer
This article is for research and educational purposes only. It is not medical advice and is not a substitute for consultation with a qualified clinician. The studies cited are real and published, but the cancer evidence base for GLP-1 receptor agonists continues to evolve and the conclusions here may shift as the cardiovascular outcome trials and the next generation of long-term active-comparator cohorts report. Anyone with a personal or family history of medullary thyroid cancer, MEN2, or active malignancy should discuss GLP-1 therapy with their prescribing clinician before starting, switching, or stopping.