At a glance
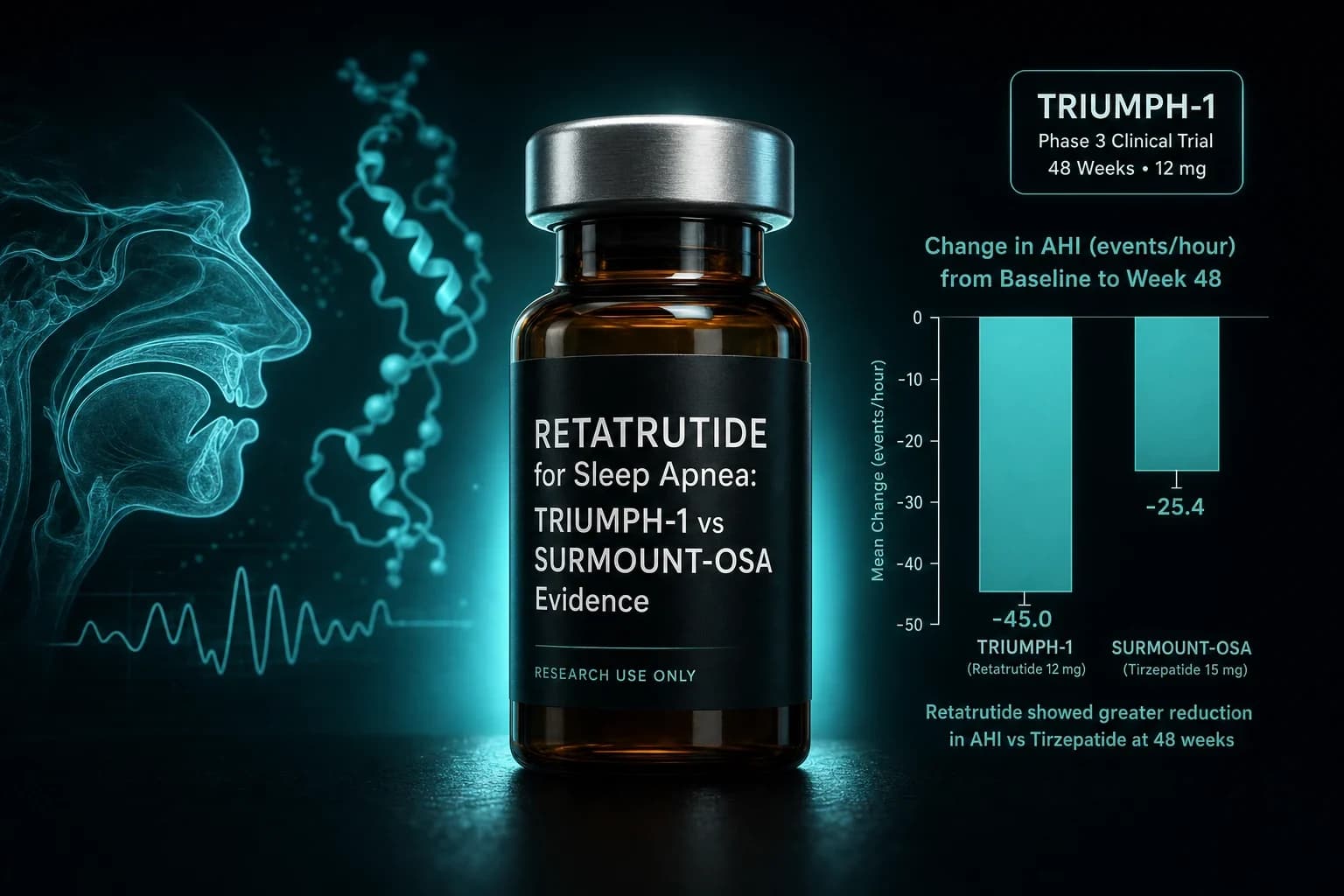
- TRIUMPH-1 OSA basket (n=243): retatrutide 12 mg cut AHI by up to 36.1 events/h (60.6%) from a 58.6 baseline at 80 weeks
- SURMOUNT-OSA Trial 1 (Malhotra et al. NEJM 2024, PMID 38912654): tirzepatide cut AHI by 25.3 events/h (55.0%) at 52 weeks
- Retatrutide's AHI reduction is the largest reported from any Phase 3 GLP-1 class agent to date, but the trial designs differ
- Retatrutide 12 mg drove 28.3% weight loss at 80 weeks in TRIUMPH-1 vs tirzepatide's 18 to 20% in SURMOUNT-OSA at 52 weeks
- TRIUMPH-5 will be the dedicated retatrutide OSA registrational trial and is required for a formal OSA label indication
Retatrutide's Phase 3 OSA subset just posted the largest apnea-hypopnea index reduction from any GLP-1 class agent, and the headline number is doing a lot of work. The triple agonist cut AHI by an average of 36.1 events per hour at the 12 mg dose, a 60.6% drop from a baseline near 58.6. Tirzepatide's SURMOUNT-OSA, the trial that produced the first FDA approval for a drug in obstructive sleep apnea, landed closer to 25 to 29 events per hour of AHI reduction in its two arms. On the surface retatrutide looks like a step change. Underneath the trial designs differ, the durations differ, and the OSA basket was nested inside an obesity trial rather than a dedicated sleep apnea registration study. This piece walks through what TRIUMPH-1 actually measured, where the retatrutide OSA numbers land against SURMOUNT-OSA on a like-for-like basis, and what the data does not yet prove.
What TRIUMPH-1's OSA basket actually was
TRIUMPH-1 is the pivotal Phase 3 obesity trial for retatrutide in adults with obesity or overweight without type 2 diabetes. Eli Lilly announced topline results on May 21, 2026, followed by an ADA Scientific Sessions presentation on June 22, 2026 that added the OSA basket detail (Eli Lilly investor press release, May 21, 2026; Eli Lilly ADA 2026 press release, June 22, 2026).
The design and rationale for TRIUMPH sit in Giblin et al. Diabetes Obes Metab 2026, PMID 41090431. Four Phase 3 trials share the retatrutide obesity dataset: TRIUMPH-1 in obesity with cardiometabolic complications, TRIUMPH-2 in obesity plus type 2 diabetes, TRIUMPH-3 in obesity with established cardiovascular disease, and TRIUMPH-4 in obesity plus knee osteoarthritis. TRIUMPH-1 enrolled 2,339 adults across the retatrutide 4 mg, 9 mg, 12 mg, and placebo arms with 80 weeks of treatment.
Within TRIUMPH-1, the OSA basket was a prespecified nested substudy of 243 participants who also had moderate-to-severe obstructive sleep apnea at baseline. Baseline mean AHI in the basket was 58.6 events per hour, which sits at the upper edge of severe OSA (the American Academy of Sleep Medicine defines severe as AHI 30 or higher). Participants were assessed by polysomnography at baseline and again during the 80 week visit.
Note: TRIUMPH-1's OSA basket is a nested prespecified subgroup within a Phase 3 obesity trial rather than a standalone OSA registration trial. The dedicated retatrutide OSA registration study is TRIUMPH-5, which is still enrolling. Peer-reviewed publication of TRIUMPH-1 primary results is expected later in 2026.
The TRIUMPH-1 OSA numbers
At 80 weeks in the OSA basket, retatrutide 12 mg reduced AHI by an average of 36.1 events per hour, a 60.6% drop from the 58.6 baseline. That leaves the average participant near 22 to 23 events per hour, which sits at the lower end of severe or upper end of moderate OSA depending on which cutoff you apply.
Weight reduction in the same OSA basket tracked the overall TRIUMPH-1 topline. Overall TRIUMPH-1 delivered mean weight loss of 28.3% at 12 mg (about 70.3 lbs) and 25.9% at 9 mg (about 64.4 lbs) at week 80, with 65.3% of 12 mg participants achieving BMI below 30 (Eli Lilly investor press release, May 21, 2026). The OSA subset weight numbers were consistent with the overall trial averages.
A useful comparison point: retatrutide's Phase 2 obesity trial (Jastreboff et al., NEJM 2023, PMID 37366315) hit 24.2% mean weight loss at 12 mg over 48 weeks. TRIUMPH-1 at 80 weeks extended the same curve by roughly four more percentage points, which is consistent with retatrutide's Phase 2 finding that weight loss had not plateaued at 48 weeks. Similarly, Rosenstock et al., Lancet 2023, PMID 37385275 reported dose-dependent glucose lowering in Phase 2 T2D that TRANSCEND-T2D-1 later confirmed at Phase 3 scale.
Retatrutide vs tirzepatide: TRIUMPH-1 vs SURMOUNT-OSA side by side
SURMOUNT-OSA is the correct comparator, but the two datasets are not perfectly matched. The comparison below is drawn from the Malhotra et al. NEJM 2024 SURMOUNT-OSA primary paper (PMID 38912654) and the TRIUMPH design paper (Giblin et al., Diabetes Obes Metab 2026, PMID 41090431) plus Lilly's TRIUMPH-1 topline releases.
| Parameter | TRIUMPH-1 OSA basket (retatrutide) | SURMOUNT-OSA Trial 1 (tirzepatide) | SURMOUNT-OSA Trial 2 (tirzepatide) |
|---|---|---|---|
| Compound | Retatrutide (GLP-1/GIP/glucagon triple) | Tirzepatide (GLP-1/GIP dual) | Tirzepatide (GLP-1/GIP dual) |
| Trial design | Nested OSA subgroup in Phase 3 obesity trial | Standalone Phase 3 OSA registration trial | Standalone Phase 3 OSA registration trial |
| PAP therapy | Mixed (not required) | Not on PAP at baseline | On PAP at baseline |
| N (arm sizes) | 243 total in OSA basket | 234 randomized | 235 randomized |
| Duration | 80 weeks | 52 weeks | 52 weeks |
| Baseline mean AHI | 58.6 events/h | 51.5 events/h | 49.5 events/h |
| Top dose | 12 mg weekly | 15 mg weekly (max tolerated) | 15 mg weekly (max tolerated) |
| AHI reduction (absolute) | 36.1 events/h | 25.3 events/h | 29.3 events/h |
| AHI reduction (% from baseline) | 60.6% | 55.0% | 62.8% |
| Placebo AHI reduction | Not yet disclosed | 5.3 events/h | 5.5 events/h |
| Mean weight loss | 28.3% | 18.1% | 20.1% |
A few takeaways worth flagging directly.
First, retatrutide's headline 60.6% AHI reduction is a percent-from-baseline number and sits in the same neighborhood as SURMOUNT-OSA Trial 2's 62.8%. The absolute AHI reduction of 36.1 events/h is meaningfully larger than tirzepatide's 25.3 to 29.3 range, and part of that is baseline: TRIUMPH-1's OSA basket started at a higher AHI. On a placebo-adjusted basis the retatrutide number will be smaller than the raw 36.1 (placebo groups in OSA trials typically show a few events/h of reduction, likely from weight change during trial life plus regression to the mean).
Second, treatment duration matters. SURMOUNT-OSA measured AHI at 52 weeks. TRIUMPH-1 measured at 80 weeks. Retatrutide had 28 extra weeks of dose exposure and weight loss to compound. The SURMOUNT-OSA time-course paper (PMID 41135142) shows AHI trends parallel weight trends across the year for tirzepatide, so an 80 week tirzepatide readout would almost certainly land higher than the 52 week number. Comparing 80 weeks of retatrutide against 52 weeks of tirzepatide is not a fair like-for-like on efficacy.
Third, SURMOUNT-OSA Trial 1 and Trial 2 are structured to isolate PAP dependency. Trial 1 enrolled participants unable or unwilling to use PAP. Trial 2 enrolled participants stable on PAP for at least three months at screening. TRIUMPH-1 did not stratify OSA participants by PAP status in the way SURMOUNT-OSA did, which limits how cleanly the datasets speak to "PAP-alternative" versus "PAP-adjunct" positioning.
Bottom line: The retatrutide 60.6% AHI reduction is real and impressive, but the trial design differences make a direct claim of superiority premature. TRIUMPH-5, the dedicated retatrutide OSA registration study, is the readout that will settle the head-to-head comparison against SURMOUNT-OSA.
What 60.6% AHI reduction means clinically
Percent reductions land differently at different starting AHIs. A 60% reduction from 30 events/h leaves a patient with mild OSA. A 60% reduction from 60 events/h leaves a patient with moderate OSA. Because TRIUMPH-1's OSA basket started high (58.6 baseline), a 60.6% cut still leaves participants above the mild threshold on average.
The clinically meaningful cutoffs, per the SURMOUNT-OSA secondary outcomes paper (PMID 41540105) and standard American Academy of Sleep Medicine definitions:
| AHI band | Severity | Interpretation |
|---|---|---|
| Under 5 events/h | Normal (no OSA) | Disease resolution |
| 5 to 14 events/h | Mild OSA | Symptomatic threshold; usually reserved for adjuncts |
| 15 to 29 events/h | Moderate OSA | Guideline threshold for active treatment |
| 30+ events/h | Severe OSA | PAP or surgical intervention typically first line |
In SURMOUNT-OSA, up to 51.5% of tirzepatide participants met a combined key secondary endpoint of AHI under 5 events/h or 5 to 14 events/h without symptoms or impairment at week 52. The TRIUMPH-1 OSA basket has not yet disclosed the equivalent responder-rate breakdown at a peer-reviewed level. Once that data lands (peer-reviewed publication expected late 2026 or early 2027), the responder-rate comparison will be more informative than the raw AHI percent-change number, because responder rates capture both the depth of AHI reduction and how many participants crossed clinically meaningful thresholds.
Weight loss is a strong candidate mediator of the effect. In SURMOUNT-OSA, mediation analysis in the secondary outcomes paper (PMID 41540105) suggested most of the AHI benefit was attributable to weight change, with a smaller residual effect that may reflect upper airway inflammation or fat depot redistribution. Retatrutide's larger weight effect makes weight-mediated AHI improvement the most parsimonious explanation for the larger observed reduction, but the mediation analysis specific to TRIUMPH-1 has not been published yet.
Where the retatrutide OSA data still falls short
Several gaps in the current TRIUMPH-1 OSA readout are worth naming plainly.
Peer-reviewed publication. As of July 2026, TRIUMPH-1 OSA basket data has been announced via ADA presentation and Lilly press release. The full manuscript, dose-by-dose breakdown, and safety profile in the OSA subgroup will land in a peer-reviewed publication later in 2026. Press releases tend to overstate efficacy and understate safety on average.
Dedicated OSA trial. TRIUMPH-1 measured OSA as a nested prespecified subgroup within an obesity trial. The dedicated retatrutide OSA registration trial is TRIUMPH-5, which is still enrolling per ClinicalTrials.gov (NCT06297603). SURMOUNT-OSA had two separate 234 and 235 participant trials designed from the start for OSA endpoints, PAP stratification, and secondary sleep-related patient-reported outcomes. TRIUMPH-5 will be needed for a formal OSA label indication with the FDA.
Hypoxic burden and sleep-related PROs. SURMOUNT-OSA published detailed secondary endpoints on hypoxic burden (an emerging predictor of cardiovascular events in OSA), Patient-Reported Outcomes Measurement Information System sleep-related impairment scales, hsCRP, and systolic blood pressure (Malhotra et al., NEJM 2024, PMID 38912654). TRIUMPH-1's OSA basket has not disclosed these endpoints yet. Without them, the AHI number alone does not paint the full picture of cardiometabolic OSA improvement.
Placebo-adjusted number. Percent-from-baseline reductions overstate treatment effects because placebo groups in OSA trials show some AHI decline. In SURMOUNT-OSA Trial 1, placebo cut AHI by 5.3 events/h; retatrutide's placebo comparator in TRIUMPH-1 OSA basket has not been publicly reported yet. The placebo-adjusted delta is what matters for regulators and payer coverage.
Head-to-head against tirzepatide. No trial has directly randomized OSA patients to retatrutide versus tirzepatide. A cross-trial numerical comparison is not the same as a controlled head-to-head, and TRIUMPH-1 versus SURMOUNT-OSA cross-comparison should be read as directional rather than definitive.
What TRIUMPH-5 needs to do
TRIUMPH-5 is the dedicated retatrutide OSA registrational trial, and it is the data readout that will actually determine whether retatrutide gets an OSA label. Design details from the TRIUMPH rationale paper (PMID 41090431) point to an enrollment target similar to SURMOUNT-OSA's parallel structure, with separate cohorts stratified by PAP dependency and endpoint measurement by polysomnography.
For an OSA label indication, TRIUMPH-5 will need to hit at least these bars:
- Statistically significant placebo-adjusted AHI reduction at the primary timepoint (likely 52 weeks to align with SURMOUNT-OSA and tirzepatide's Zepbound label)
- Responder-rate secondary endpoint (proportion under 5 or 5 to 14 events/h) to support the disease resolution or downgrade claim that Zepbound's label carries
- Hypoxic burden and sleep-related PRO improvements to support the broader cardiometabolic benefit story
- Safety profile in an OSA-plus-obesity population that does not add meaningful signals beyond the incretin class baseline (nausea, vomiting, diarrhea)
Retatrutide's Phase 2 obesity safety profile (Jastreboff et al., NEJM 2023, PMID 37366315) showed GI events accounted for most adverse events and were dose-dependent, consistent with the class. TRIUMPH-1's overall discontinuation and adverse event rates in the pivotal announcement did not flag anything outside class expectations, but the dose-by-dose and subgroup breakdown will land with the full publication.
Where retatrutide fits in current OSA treatment
FDA approval of Zepbound for moderate-to-severe OSA in adults with obesity landed on December 20, 2024 (FDA press announcement). That approval broke the OSA category open by demonstrating that an injectable metabolic agent could treat the underlying driver of OSA rather than the symptom.
Retatrutide's TRIUMPH-1 OSA data suggests the triple agonist can push further into the AHI-reduction space, and the peer-reviewed publication plus TRIUMPH-5 readout will decide whether that translates into a distinct OSA label. For context on tirzepatide's approved path and what SURMOUNT-OSA actually showed, see the tirzepatide sleep apnea SURMOUNT-OSA evidence guide. For the broader retatrutide picture, the retatrutide TRIUMPH-1 Phase 3 topline coverage covers the pivotal obesity readout, and the retatrutide vs tirzepatide vs semaglutide comparison puts the head-to-head weight numbers side by side. For readers newer to the compound, the retatrutide triple agonist explainer covers the receptor pharmacology.
Cost and access still favor tirzepatide by a wide margin. Zepbound has an approved OSA label, insurance coverage in some plans, and 503B compounded supply routes for research and cash-pay contexts. Retatrutide remains investigational and is not approved for any indication.
Practical framing for a research audience
Retatrutide is not clinically available. The compound sold on the research peptide market is unregulated, unverified, and not what a Phase 3 trial dispenses. TRIUMPH-1 dosed a specific pharmaceutical formulation of retatrutide with defined pharmacokinetics and quality control. Vendor-sourced retatrutide has none of those guarantees.
For readers who follow the class for personal research purposes, the more actionable comparison right now is tirzepatide (Zepbound) since it has the approved OSA label and stable supply. Semaglutide does not have an OSA label but sits adjacent to the class discussion. The retatrutide compound page tracks trial progress and dosing conventions but is framed strictly for research context, not clinical use.
Sleep apnea is a serious condition with dedicated diagnosis and treatment pathways. PAP therapy, positional therapy, oral appliances, and surgical options each have their own evidence base and clinician-directed protocols. GLP-1 class agents are additive to that clinical set, not a replacement for it.
Bottom line
Retatrutide's TRIUMPH-1 OSA basket delivered a 60.6% AHI reduction at 80 weeks, the largest number reported from any Phase 3 GLP-1 class agent to date. That headline should be read carefully. Trial design differences (80 versus 52 weeks, nested subgroup versus dedicated trial, mixed versus PAP-stratified populations) prevent a clean head-to-head against tirzepatide's SURMOUNT-OSA results. TRIUMPH-5, the dedicated retatrutide OSA registration trial, is where the direct comparison will actually get resolved. Until then, the retatrutide OSA data is a strong signal, not a settled question.
Related reading
- Tirzepatide sleep apnea SURMOUNT-OSA evidence guide
- Retatrutide TRIUMPH-1 Phase 3 topline coverage
- Retatrutide TRANSCEND-T2D-1 Phase 3 diabetes evidence
- Retatrutide vs tirzepatide vs semaglutide 2026
- Retatrutide explained: triple agonist pharmacology
- GLP-1 dosing comparison 2026
- Tirzepatide compound page
- Retatrutide compound page
- Reconstitution calculator
This article is for educational and research purposes only and is not medical advice. Retatrutide is an investigational compound not approved for human use in any indication in any jurisdiction as of July 2026. TRIUMPH-1 OSA basket data described here is drawn from Eli Lilly press releases and ADA 2026 conference presentations that have not yet been peer-reviewed; numbers and safety conclusions may change with publication. Cross-trial comparisons with SURMOUNT-OSA are directional and are not a substitute for a controlled head-to-head trial. Obstructive sleep apnea is a serious medical condition that requires clinician-directed diagnosis and treatment; nothing in this article is a recommendation to use any peptide or drug for OSA outside a supervised clinical context. Consult a licensed sleep physician for any decision about OSA diagnosis or management.