At a glance
- Rusfertide is a synthetic 9-amino-acid hepcidin mimetic that binds ferroportin, forcing its internalization and reducing iron export from macrophages and enterocytes.
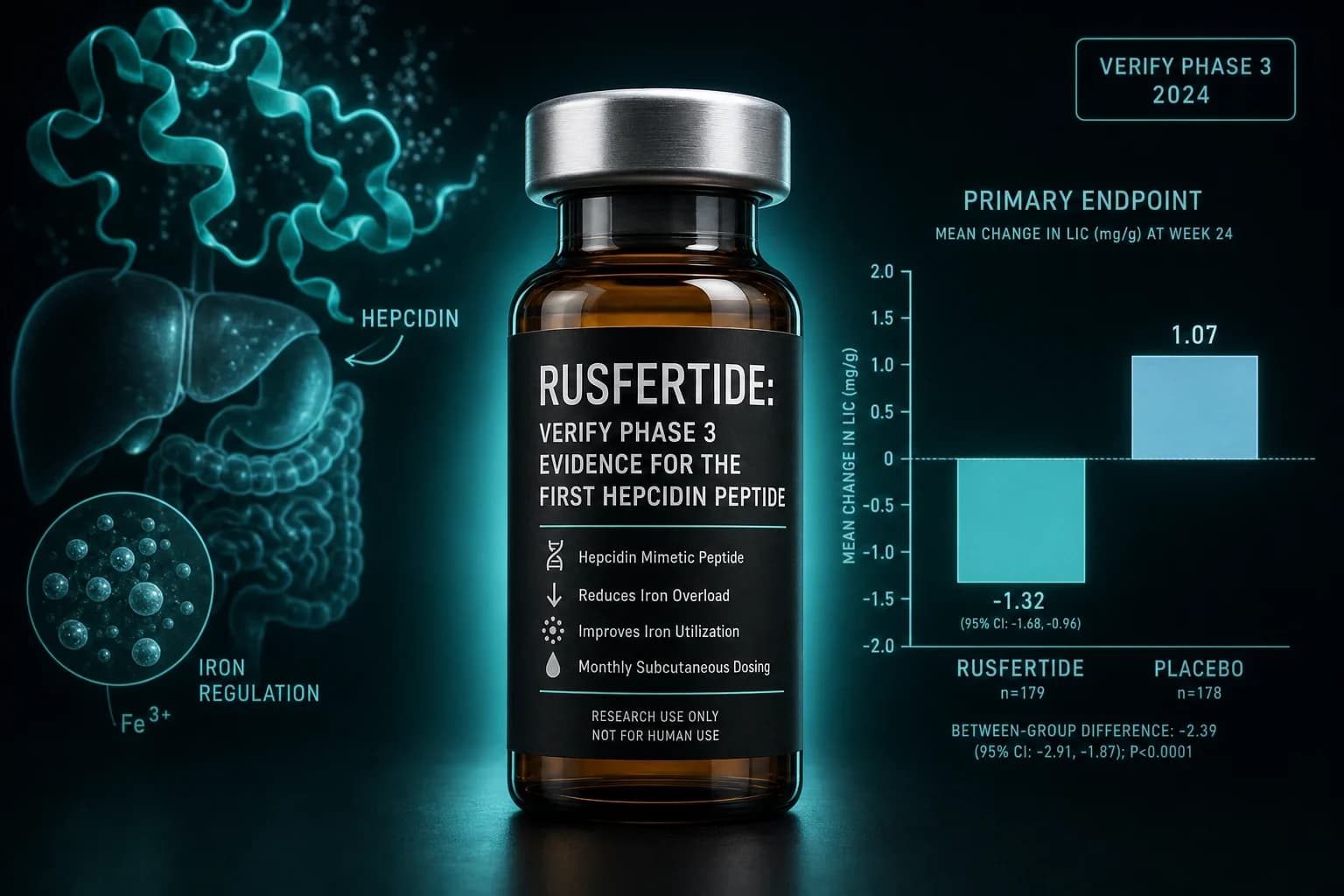
- VERIFY Phase 3 (n=293): 76.9% clinical response on rusfertide vs 32.9% placebo at weeks 20 to 32, with a mean 0.5 phlebotomies per patient vs 1.8 on standard of care.
- REVIVE Phase 2 ([Kremyanskaya et al., NEJM 2024, PMID 38381675](https://pubmed.ncbi.nlm.nih.gov/38381675/)) already showed 60% response vs 17% placebo in a 12-week randomized withdrawal.
- FDA accepted the NDA and granted Priority Review on 2 March 2026 with a PDUFA target in Q3 2026, on top of prior Breakthrough, Orphan Drug and Fast Track designations.
- Rusfertide does not replace hydroxyurea, ropeginterferon or ruxolitinib. It is an add-on for phlebotomy-dependent patients whose hematocrit is not controlled by current therapy.
The FDA is a few months from approving the first hepcidin peptide
Rusfertide (PTG-300) is a synthetic 9-amino-acid mimetic of hepcidin, the liver hormone that decides how much iron the bone marrow gets. Protagonist Therapeutics designed it, Takeda partnered on it, and on 2 March 2026 the FDA accepted the New Drug Application and granted Priority Review, with a Prescription Drug User Fee Act target date in the third quarter of 2026. If the review lands cleanly, rusfertide becomes the first therapeutic peptide that treats a myeloproliferative neoplasm by tuning iron flux instead of chemotherapy, cytokines, or JAK inhibition.
The clinical case rests on two trials. REVIVE, the Phase 2 randomized withdrawal published by Kremyanskaya et al. in the New England Journal of Medicine in 2024 (PMID 38381675), showed 60% response on rusfertide versus 17% on placebo. VERIFY, the Phase 3, hit 76.9% response versus 32.9% on standard of care alone, with a fraction of the phlebotomies. Both trials tested rusfertide as an add-on to existing therapy in phlebotomy-dependent polycythemia vera patients.
This walkthrough covers what rusfertide is at the molecular level, why polycythemia vera needs a hepcidin approach in the first place, what REVIVE and VERIFY actually measured, how the drug fits alongside hydroxyurea and ropeginterferon, and where the regulatory timeline stands.
What rusfertide actually is
Rusfertide is a chemically stabilized peptide analog of human hepcidin, retaining the ferroportin-binding pharmacophore of the native 25-amino-acid hormone while adding polyethylene glycol and D-amino acid substitutions to extend plasma half-life. It binds ferroportin at low nanomolar potency (EC50 approximately 5 nM in cell-based assays) and triggers the same conformational change that endogenous hepcidin induces, driving receptor internalization and lysosomal degradation. That is exactly the mechanism Nemeth et al. established in Science in 2004 for native hepcidin.
Once ferroportin is degraded, iron efflux from macrophages, hepatocytes, and duodenal enterocytes falls. Serum iron drops. Transferrin saturation drops. The bone marrow, which needs continuous iron delivery to make red blood cells, runs into a substrate ceiling. Erythropoiesis slows. In healthy iron biology this is a rheostat. In polycythemia vera, where hepcidin is inappropriately low, rusfertide takes over the rheostat and clamps it shut.
Route is a weekly subcutaneous self-injection. The Modi et al. 2024 first-in-human study in the European Journal of Haematology (DOI 10.1111/ejh.14243) showed dose-proportional exposure up to 80 mg, prompt reductions in serum iron and transferrin saturation within 24 hours, and a tolerability profile dominated by mild injection site reactions.
Note: Rusfertide is not a JAK2 inhibitor and does not target the driver mutation in polycythemia vera. It treats the phenotype (iron-driven erythrocytosis), not the clone. This matters for how you position it against ruxolitinib and interferon.
Why polycythemia vera needs a hepcidin approach
Polycythemia vera is a chronic clonal myeloproliferative neoplasm driven in more than 95% of cases by a JAK2 V617F mutation. The mutation constitutively activates JAK-STAT signaling in hematopoietic progenitors, producing autonomous red blood cell overproduction that is largely independent of erythropoietin. The clinical hazard is thrombosis. High hematocrit thickens blood, raises viscosity, and drives arterial and venous thrombotic events that account for the majority of PV mortality.
The evidence anchor is Marchioli et al., NEJM 2013 (PMID 23216616). The CYTO-PV trial randomized 365 PV patients to a hematocrit target below 45% versus 45 to 50%. The tighter target cut cardiovascular death or major thrombosis from 4.4 to 1.1 events per 100 person-years. That single number is why every subsequent PV guideline pins hematocrit at less than 45% for men and less than 42% for women.
The problem is that current tools for hitting that target are blunt. Standard of care is:
- Therapeutic phlebotomy: draw 500 mL of blood every few weeks to physically remove red cell mass.
- Cytoreduction: hydroxyurea or interferons (ropeginterferon alfa-2b, pegylated interferon alfa-2a) to suppress bone marrow proliferation.
- Ruxolitinib for hydroxyurea-resistant or intolerant patients.
- Low-dose aspirin for antithrombotic prophylaxis.
Phlebotomy works, but repeated blood draws deplete body iron stores, and iron deficiency in PV drives symptomatic fatigue, brain fog, and pica while paradoxically stimulating more erythropoiesis. Hydroxyurea works, but roughly a quarter of patients are resistant or intolerant, and long-term leukemogenic risk remains a point of ongoing debate. Interferons are disease-modifying but slow to work, poorly tolerated in a subset of patients, and expensive.
Hepcidin biology suggests a cleaner lever. In Ganz and Nemeth's Blood 2011 review (PMID 22160086), the hepcidin-ferroportin axis is described as the principal regulator of extracellular iron homeostasis, with hepcidin deficiency the shared upstream mechanism in hereditary hemochromatosis, thalassemia intermedia, and, as later work established, polycythemia vera. In PV, hepcidin is suppressed by both erythroferrone (secreted by expanded erythroid progenitors) and by JAK2-driven bone marrow demand. Adding back a hepcidin-mimicking peptide directly targets that suppressed axis.
REVIVE Phase 2: the proof of concept
REVIVE was an international three-part Phase 2 trial in phlebotomy-dependent PV patients. Part 1 was a 28-week open-label dose-finding run in 70 patients. Part 2 was a 12-week randomized withdrawal in 59 patients (30 rusfertide, 29 placebo). Part 3 was a long-term extension.
The primary endpoint in Part 2 was the proportion of patients who maintained response, defined as absence of therapeutic phlebotomy, hematocrit under 45%, and study completion. From the Kremyanskaya et al. NEJM 2024 paper (PMID 38381675):
- Response rate: 60% rusfertide vs 17% placebo (P < 0.001)
- Mean hematocrit maintained under 45% across the 28-week dose-finding period
- Iron indices normalized: ferritin rose from a mean below 20 ng/mL toward normal range
- Patient-reported symptoms (fatigue, pruritus, concentration) improved on rusfertide but not placebo
- Adverse events were dominated by grade 1 to 2 injection site reactions; no grade 4 or 5 events
That last point is important. Injection site reactions were common (roughly half of patients had at least one) but rarely severe and rarely led to discontinuation. No clinically significant laboratory toxicity emerged over the 28-week dosing window.
REVIVE was small and its randomized phase was short. But it established three things: rusfertide reliably clamps hematocrit under 45%, it reverses phlebotomy-induced iron deficiency without triggering rebound erythrocytosis, and it moves symptom scores in the same direction as the hematologic response. Those are the three variables Phase 3 had to reproduce at scale.
VERIFY Phase 3: scale confirmation
VERIFY (NCT05210790) is a global, randomized, double-blind, placebo-controlled Phase 3 trial. 293 patients with phlebotomy-dependent PV were randomized 1:1 to weekly subcutaneous rusfertide or placebo on top of their existing standard of care, which for most participants included ongoing cytoreduction with hydroxyurea, interferons, or ruxolitinib.
Topline was reported by Takeda on 27 March 2025. The full primary analysis was presented at the ASCO 2025 Annual Meeting as abstract LBA3 and updated at the ASH 2025 Annual Meeting.
The primary endpoint was clinical response between weeks 20 and 32, defined as no phlebotomy plus hematocrit control and study completion.
| Endpoint | Rusfertide + SOC | Placebo + SOC |
|---|---|---|
| Clinical response (weeks 20 to 32) | 76.9% | 32.9% |
| Mean phlebotomies per patient | 0.5 | 1.8 |
| Hematocrit control (< 45%) | Sustained | Not sustained |
| Symptom improvement (fatigue, pruritus, concentration) | Statistically significant | Not significant |
| Injection site reactions | 55.9% | 32.9% |
All four key secondary endpoints hit, including patient-reported symptom improvement on the myeloproliferative neoplasm symptom assessment form (MPN-SAF TSS). The safety profile mirrored REVIVE: mostly mild injection site reactions, no unexpected laboratory toxicity, and no new signal of thrombotic events at 32 weeks.
Bottom line: VERIFY did not just replicate REVIVE. It replicated it against active standard-of-care background therapy in a much larger population. The 44-percentage-point placebo-adjusted response and the near-elimination of phlebotomies are the strongest data any hepcidin-targeting therapeutic has generated in a myeloproliferative neoplasm.
REVIVE vs VERIFY at a glance
| Feature | REVIVE Phase 2 | VERIFY Phase 3 |
|---|---|---|
| Design | Three-part, open-label + randomized withdrawal | Global randomized, double-blind, placebo-controlled |
| N | 70 (Part 1) / 59 (Part 2) | 293 |
| Comparator | Placebo (Part 2) | Placebo on top of standard of care |
| Primary endpoint | Response at 12 weeks (post-withdrawal) | Response at weeks 20 to 32 |
| Response rate | 60% rusfertide vs 17% placebo | 76.9% rusfertide vs 32.9% SOC |
| Phlebotomy reduction | Yes, sustained under 45% Hct | Mean 0.5 vs 1.8 per patient |
| Symptom endpoint | Improved on rusfertide | MPN-SAF TSS improved on rusfertide |
| Safety | Grade 1 to 2 ISRs dominant | Same pattern, larger dataset |
| Publication | NEJM 2024 (PMID 38381675) | ASCO 2025 LBA3 + ASH 2025 |
Beyond polycythemia vera: hemochromatosis and beta-thalassemia
Rusfertide's mechanism is not disease-specific. Any condition driven by inappropriately low hepcidin or by iron overload is a candidate. Two directions have already produced clinical data.
Hereditary hemochromatosis is the mirror image of PV: HFE mutations impair hepcidin production, ferroportin stays open, and iron loads chronically into liver, heart, and endocrine tissues. Standard care is scheduled phlebotomy for life. Kowdley et al. published an open-label proof-of-concept Phase 2 trial in Lancet Gastroenterology and Hepatology in 2023 (PMID 37863080) in HFE-related hemochromatosis. Rusfertide maintained liver iron concentration in the absence of phlebotomy across the treatment period. This is a genuine unmet need indication because current care is a lifetime of scheduled blood draws with no pharmacologic alternative.
Beta-thalassemia intermedia is more speculative. In thalassemia, ineffective erythropoiesis suppresses hepcidin, iron loads without transfusion, and existing hepcidin mimetics have been proposed as adjunctive iron control. Rusfertide has moved into thalassemia dosing exploration but has not read out a pivotal trial.
The takeaway for rusfertide as a platform: the drug is a hepcidin agonist, and the same peptide has generated positive Phase 2 data in two mechanistically opposite diseases (iron overproduction from PV, iron overload from HFE). That is unusual outside of anti-inflammatories and speaks to how central the ferroportin lever is in mammalian iron biology.
Where rusfertide fits in the current PV treatment stack
Rusfertide is not a first-line replacement for hydroxyurea or ropeginterferon. It does not touch the JAK2 clone, does not reduce leukocyte or platelet counts, and does not carry disease-modifying claims. What it does is control the hematologic phenotype that drives thrombosis, in patients whose hematocrit is not adequately controlled by cytoreductive therapy alone.
| Therapy | Mechanism | Primary role | Iron impact | Practical caveat |
|---|---|---|---|---|
| Therapeutic phlebotomy | Physical red cell removal | Standard for all PV | Depletes stores | Symptomatic iron deficiency, fatigue, brain fog |
| Hydroxyurea | Ribonucleotide reductase inhibitor | First-line high-risk PV | Neutral | Roughly 25% resistant/intolerant; long-term safety debate |
| Ropeginterferon alfa-2b | Type I interferon | First-line low-risk PV, disease-modifying | Neutral | Slow onset, tolerability variable |
| Ruxolitinib | JAK1/JAK2 inhibitor | Second-line after hydroxyurea failure | Neutral | Anemia and infection risk |
| Rusfertide (pending) | Hepcidin mimetic, ferroportin degrader | Add-on for phlebotomy-dependent PV | Restores iron balance | Weekly subq, ISRs common |
The rational placement, based on VERIFY's design, is as add-on for patients who still need frequent phlebotomy despite adequate cytoreduction. Some of the strongest symptomatic gains in REVIVE came from reversing iron deficiency without allowing hematocrit to rebound.
Regulatory status and PDUFA target
The rusfertide clinical package carries an unusually stacked set of FDA designations:
- Breakthrough Therapy Designation
- Orphan Drug Designation
- Fast Track Designation
- Priority Review (granted 2 March 2026)
Takeda and Protagonist submitted the NDA on 30 January 2026. The FDA accepted it on 2 March 2026 with a Q3 2026 PDUFA target date. If approved, rusfertide would be the first hepcidin-pathway therapeutic in any indication, launching into a PV market that has not seen a new mechanism approved since ropeginterferon (BESREMi) in 2021 and ruxolitinib (Jakafi) for PV in 2014.
The commercial partnership is Takeda-led. Protagonist Therapeutics owns the discovery IP and shares economics; Takeda handles the NDA, launch, and commercial infrastructure.
Warning: Rusfertide is not FDA-approved as of July 2026. It is under regulatory review. Nothing in this article authorizes personal use. Peptide vendors selling rusfertide or PTG-300 as a research chemical are operating outside any clinical-use pathway, and the drug is not a maintenance therapy for anyone with polycythemia vera, hemochromatosis, or any iron disorder outside a supervised trial.
What this means for the peptide therapeutics field
Rusfertide is a data point in a slow but real trend: rationally designed peptide agonists of endogenous receptor systems are graduating from Phase 1 curiosities to Phase 3 assets and, increasingly, to approved drugs. Semaglutide and tirzepatide made the case in metabolism. Sotatercept made a related case for the activin pathway in pulmonary arterial hypertension. Rusfertide extends that pattern into hematology.
Three implications matter for how the field reads this.
First, first-in-class peptide receptor agonists can generate placebo-adjusted response gaps in the 40-percentage-point range when the underlying receptor biology is well characterized. Semaglutide vs placebo on cardiovascular outcomes, sotatercept vs placebo on PAH clinical worsening, and now rusfertide vs placebo on PV phlebotomy dependence all share that magnitude. That is a very different signal from small-molecule symptomatic drugs.
Second, chemically stabilized peptides can hit weekly or monthly dosing with acceptable tolerability. Rusfertide is weekly subcutaneous. Semaglutide is weekly subcutaneous or oral daily. Long-acting cagrilintide is weekly. The dosing frequency ceiling for peptide therapeutics has moved.
Third, therapeutic peptides tend to have much cleaner off-target profiles than small molecules, at the cost of injectable delivery. Rusfertide's REVIVE and VERIFY safety readouts are dominated by injection site reactions. That is the trade-off pattern seen across thymosin alpha-1 clinical evidence, SS-31 (elamipretide) mitochondrial data, and the incretin class. Injectable peptides are generally well tolerated because they act at the receptor they were designed for and little else, and most stay out of the CNS unless engineered to cross the blood-brain barrier. Route context lives in the injectable vs oral peptide bioavailability guide.
What rusfertide is not
Rusfertide does not cure polycythemia vera. It does not eradicate the JAK2 clone, does not reduce transformation risk to myelofibrosis or acute leukemia, and does not replace the disease-modifying claim that ropeginterferon holds. It also does not reduce leukocyte or platelet counts, so patients with thrombocytosis-driven risk still need cytoreduction.
It also does not have oral bioavailability. It does not have a data package in essential thrombocythemia, primary myelofibrosis, or any non-clonal cause of secondary erythrocytosis. Sleep apnea, high-altitude erythrocytosis, and testosterone-induced polycythemia are all mechanistically distinct and not covered by any current rusfertide trial.
The takeaway
Rusfertide is on the verge of becoming the first approved hepcidin-mimetic peptide, and the VERIFY Phase 3 data support that trajectory. In a population where the driver mutation is JAK2 but the killer is hematocrit-driven thrombosis, a drug that controls hematocrit through iron restriction rather than bone marrow suppression opens a distinct treatment lane. The FDA decision is expected within Q3 2026, and prescribing patterns will need to answer a specific question: which phlebotomy-dependent PV patients benefit most from adding a weekly peptide injection to their existing regimen.
For anyone reading this as an early-stage indicator of where peptide therapeutics are heading, rusfertide is the second-clearest example in the past year (after retatrutide) that a well-characterized endogenous receptor is a fair place to place drug development risk. Regulatory context for other peptide-adjacent decisions this year lives in the FDA July 2026 peptide compounding review. The broader question of where injectable peptides stand versus oral formulations is covered in the injectable vs oral peptides guide. For a comparison compound with a similarly narrow but high-conviction dataset, see the SS-31 (elamipretide) FDA approval writeup.
Related coverage
- Thymosin alpha-1 clinical evidence
- SS-31 (elamipretide) FDA approval breakdown
- FDA July 2026 peptide compounding review
- Injectable vs oral peptide bioavailability guide
- FDA peptide reclassification February 2026
- Thymosin alpha-1 compound page
- Reconstitution calculator
This article is for educational and research purposes only and is not medical advice. Rusfertide is an investigational peptide therapeutic. As of July 2026 it is under FDA Priority Review with a Q3 2026 PDUFA target and is not approved for polycythemia vera, hereditary hemochromatosis, beta-thalassemia, or any other indication. All clinical data described above are from Phase 2 REVIVE, Phase 3 VERIFY (topline and conference presentations), a Phase 2 hemochromatosis proof-of-concept trial, and a Phase 1 first-in-human study in healthy volunteers. Do not interpret the placebo-adjusted response numbers above as generalizable to non-phlebotomy-dependent polycythemia vera, secondary erythrocytosis, athletic hematocrit management, or any off-label use. Rusfertide is a prescription-track drug candidate; peptide vendors offering rusfertide or PTG-300 as a research chemical are operating outside any clinical-use pathway, and the safety profile characterized in trials assumed medically supervised weekly subcutaneous dosing with hematologist follow-up. Polycythemia vera is a myeloproliferative neoplasm with disease-specific thrombotic and transformation risks that require ongoing hematology care regardless of any single drug. Consult a licensed clinician before making any change to diagnosis, monitoring, or treatment of an iron or myeloproliferative disorder.