At a glance
- IMPACT Phase 2b (Noureddin et al., Lancet 2025, PMID 41237796) hit MASH resolution at 24 weeks: 58% on 1.2 mg and 52% on 1.8 mg vs 20% placebo (P<0.0001)
- Fibrosis improvement without MASH worsening did not separate from placebo at 24 weeks, but 48-week ELF dropped 0.49 and 0.58 vs +0.16 placebo (P<0.0001)
- Weight loss extended from 4.8% and 5.8% at 24 weeks to 4.5% and 7.5% at 48 weeks with no plateau on the 1.8 mg dose
- Discontinuation due to adverse events was lower on pemvidutide (0 to 1%) than placebo (2%), even without dose titration
- Pemvidutide is investigational; PERFORMA Phase 3 starts H2 2026; the molecule holds FDA Breakthrough Therapy designation in MASH
A dual agonist that just earned a Lancet publication and a Best of EASL nod
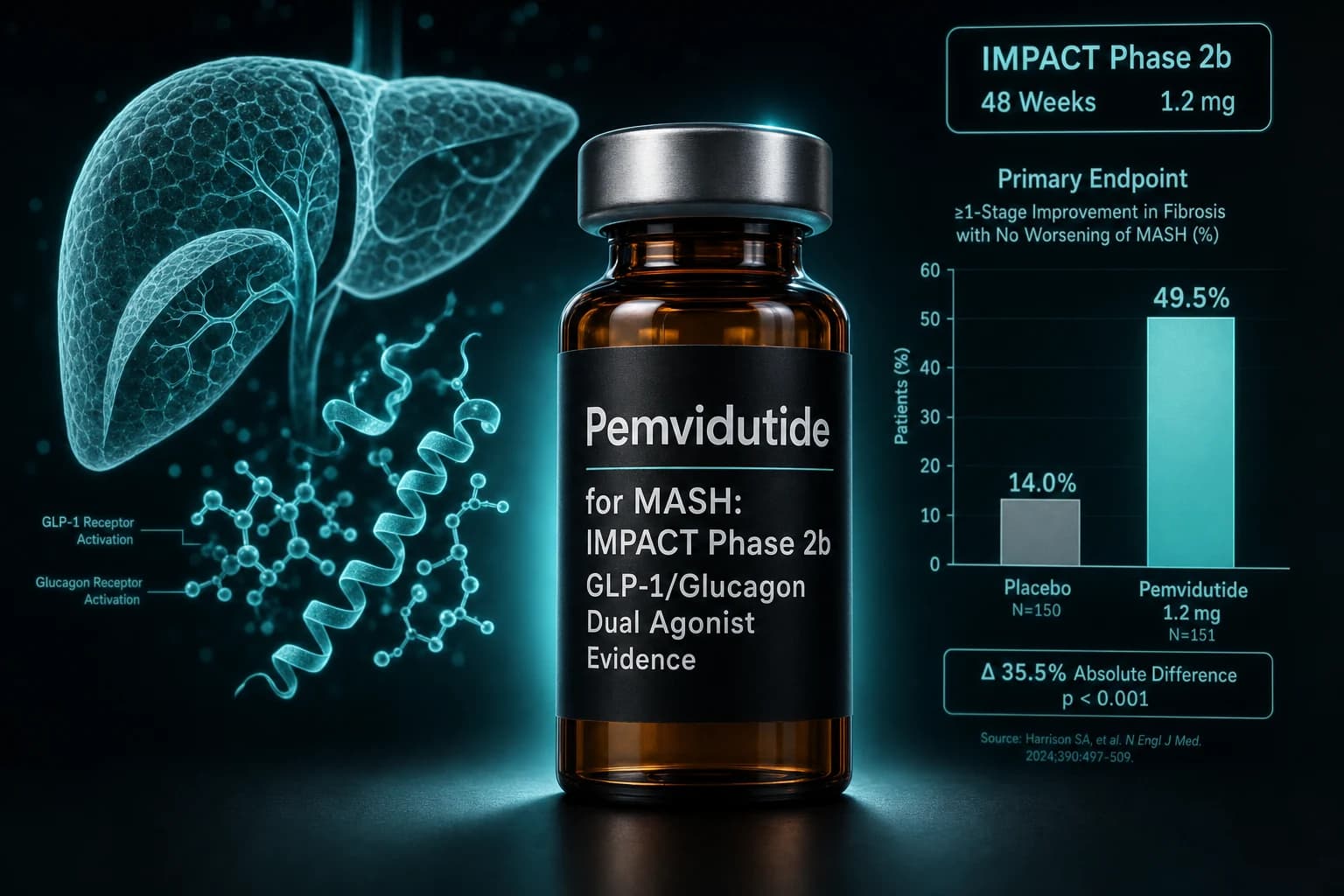
Pemvidutide is the second GLP-1 plus glucagon dual receptor agonist to read out a positive Phase 2b in metabolic dysfunction-associated steatohepatitis, and the first to do so in a Lancet publication. The 24-week IMPACT trial hit one of two co-primary endpoints. The 48-week topline announced in December 2025 extended weight loss without a plateau and pushed the antifibrotic non-invasive markers further apart from placebo. The EASL Congress 2026 late-breaking poster on May 27 added quantitative digital pathology evidence of fibrosis regression on biopsy. None of that earns the molecule an FDA approval yet, but it does pull pemvidutide into the same conversation as semaglutide and resmetirom in a way that did not exist a year ago.
The headline data, in one line: 58 percent of patients on pemvidutide 1.2 mg achieved MASH resolution without worsening of fibrosis at 24 weeks, versus 20 percent on placebo, in 212 biopsy-confirmed F2 to F3 patients across 83 US and Australian sites (Noureddin et al., Lancet 2025, PMID 41237796).
Bottom line: Pemvidutide is the first GLP-1/glucagon dual agonist with a Lancet-published Phase 2b MASH resolution result, but the fibrosis improvement endpoint missed at 24 weeks and only separated from placebo on non-invasive measures at 48 weeks. Phase 3 PERFORMA, planned for the second half of 2026, has to prove the biopsy story holds.
What pemvidutide actually is
Pemvidutide, also known as ALT-801, is a once-weekly subcutaneous 29 amino acid peptide developed by Altimmune. Structurally it is a unimolecular dual agonist engineered for 1:1 potency at the glucagon-like peptide-1 receptor (GLP-1R) and the glucagon receptor (GCGR). The molecule carries a EuPort glycolipid surfactant conjugation that slows entry into the bloodstream, reduces peak plasma concentrations, and extends effective duration of action enough to support weekly dosing without titration.
The receptor logic is what makes the MASH story plausible. GLP-1 receptor activation drives appetite suppression and weight loss, the indirect lever that pulls liver fat down. Glucagon receptor activation acts directly on hepatocytes: it increases hepatic fatty acid oxidation, suppresses de novo lipogenesis, and reduces VLDL secretion. The hypothesis behind dual agonism in MASH is that you can stack the indirect weight-loss benefit of GLP-1 with a direct liver-fat lowering effect from glucagon agonism, and the 1:1 balance is the bet that glucagon-mediated catabolism does not generate clinically meaningful hyperglycemia in the population pemvidutide is targeting.
Compared to the rest of the class:
- Semaglutide is a pure GLP-1 mono-agonist
- Tirzepatide is GLP-1 plus GIP
- Survodutide is GLP-1 plus glucagon, titrated to higher doses
- Mazdutide is GLP-1 plus glucagon with GLP-1-dominant ratios
- Retatrutide adds glucagon and GIP to GLP-1 for triple agonism
The closest mechanistic neighbor in the published clinical literature is survodutide, which we covered in the survodutide GCG/GLP-1 dual agonist trial evidence guide. The closest tonal neighbor for the GLP-1/glucagon framing is mazdutide, covered in the mazdutide IBI362 Phase 3 evidence article. Pemvidutide sits between those two on dose magnitude and has gone furthest in MASH-specific Phase 2 data so far.
The IMPACT Phase 2b trial that hit half its co-primary endpoints
IMPACT (NCT05989711) is an ongoing 48-week, international, randomized, double-blind, placebo-controlled Phase 2b trial. The 24-week results are what got published in The Lancet in November 2025.
Trial design specifics from the Lancet paper:
- 1,557 patients screened from July 27, 2023 to April 29, 2025
- 212 patients randomized at 83 sites in the US and Australia
- Biopsy-confirmed MASH with fibrosis stage F2 or F3 at baseline
- Randomization 1:2:2 to placebo (n=86), pemvidutide 1.2 mg (n=41), or pemvidutide 1.8 mg (n=85)
- Once-weekly subcutaneous injection, no dose titration
- Dual co-primary endpoints at 24 weeks: MASH resolution without worsening of fibrosis, and fibrosis improvement by at least one stage without worsening of MASH
The 24-week MASH resolution result:
| Group | MASH resolution without fibrosis worsening | vs placebo |
|---|---|---|
| Placebo (n=86) | 18/86 (20%) | reference |
| Pemvidutide 1.2 mg (n=41) | 24/41 (58%) | P<0.0001 |
| Pemvidutide 1.8 mg (n=85) | 45/85 (52%) | P<0.0001 |
The 24-week fibrosis improvement result is the part that did not separate cleanly. Fibrosis improvement by at least one stage without worsening of MASH was 30/85 (36%) on pemvidutide 1.8 mg, but the confidence interval crossed zero and the comparison did not reach statistical significance at 24 weeks. Pemvidutide met the MASH resolution endpoint and missed the fibrosis improvement endpoint at this timepoint.
Weight loss at 24 weeks:
| Group | Mean body weight change | vs placebo |
|---|---|---|
| Placebo | -0.5% | reference |
| Pemvidutide 1.2 mg | -4.8% | P<0.001 |
| Pemvidutide 1.8 mg | -5.8% | P<0.001 |
Discontinuations due to adverse events were lower on both pemvidutide arms than on placebo: 0% on 1.2 mg, 1% on 1.8 mg, 2% on placebo. That result held without using dose titration, which matters because the rest of the class typically requires titration to manage GI adverse events.
What the 48-week and EASL 2026 readouts added
Altimmune announced 48-week IMPACT topline results on December 19, 2025. The Phase 2b is still ongoing for additional analyses, but the published 48-week data give a cleaner picture of where pemvidutide is heading.
The 48-week fibrosis non-invasive test (NIT) results moved further apart from placebo than at 24 weeks:
- Enhanced Liver Fibrosis (ELF) score change from baseline: -0.49 (1.2 mg) and -0.58 (1.8 mg) versus +0.16 (placebo), P<0.0001 both doses
- Liver stiffness measurement (LSM) by FibroScan: mean reductions of 3.04 and 3.97 kPa on 1.2 mg and 1.8 mg
- Liver fat content drops of 45.2% and 54.7% versus 8.2% on placebo
- ALT reductions of roughly 38 IU/L versus 10.3 IU/L on placebo
Weight loss at 48 weeks did not plateau on the higher dose:
| Group | 24-week weight loss | 48-week weight loss |
|---|---|---|
| Placebo | -0.5% | -0.2% |
| Pemvidutide 1.2 mg | -4.8% | -4.5% |
| Pemvidutide 1.8 mg | -5.8% | -7.5% |
The 1.8 mg dose was still losing weight between weeks 24 and 48, which is the curve shape Altimmune needs to make a Phase 3 case in MASH where weight loss is a known mediator of histologic improvement.
The EASL Congress 2026 update on May 27, 2026 was selected as Best of EASL 2026. The headline addition was qFibrosis, a HistoIndex AI-based digital pathology measurement applied to the IMPACT biopsies. The 24-week qFibrosis data showed significant improvements in fibrosis stage on quantitative digital pathology even though the conventional pathologist-read biopsy fibrosis endpoint had missed statistical significance at 24 weeks. That is the kind of result that gets debated in hepatology: the pathologist read is the regulatory standard, and a digital pathology supportive signal does not change that, but it does shape the prior on whether the 48-week biopsy results in Phase 3 are likely to land.
The EASL poster also reported concurrent improvements across multiple non-invasive tests. 37.8% of pemvidutide 1.2 mg patients and 22.7% of pemvidutide 1.8 mg patients achieved at least a 30% LSM reduction concurrent with other NIT improvements, versus 8.3% on placebo.
How pemvidutide compares to semaglutide, survodutide, and resmetirom
The MASH field in 2026 has one approved drug class and three published Phase 2 or Phase 3 trials in the same patient population. Direct head-to-head trials do not exist, and trial populations and biopsy reading conventions differ enough that cross-trial comparison is interpretation, not arithmetic. With that caveat:
| Drug | Class | Trial (PMID) | N | Duration | MASH resolution (best dose vs placebo) | Fibrosis improvement (best dose vs placebo) | Weight loss (best dose) | Status |
|---|---|---|---|---|---|---|---|---|
| Resmetirom | THRβ agonist, oral | MAESTRO-NASH (Harrison et al., NEJM 2024, PMID 38324483) | 966 | 52 wks | 29.9% vs 9.7% (100 mg) | 25.9% vs 14.2% (100 mg) | ~3% | FDA accelerated approval Mar 2024 |
| Semaglutide 2.4 mg | GLP-1 mono-agonist, SC weekly | ESSENCE (Sanyal et al., NEJM 2025, PMID 40305708) | 1,197 | 72 wks | 62.9% vs 34.3% | 36.8% vs 22.4% | ~10% | FDA accelerated approval Aug 2025 |
| Survodutide | GLP-1/glucagon dual, SC weekly | Phase 2 (Sanyal et al., NEJM 2024, PMID 38847460) | 295 | 48 wks | not the primary endpoint | MASH improvement no fibrosis worsening 62% vs 14% (4.8 mg) | ~10 to 15% | Phase 3 LIVERAGE recruiting |
| Pemvidutide | GLP-1/glucagon dual, SC weekly | IMPACT (Noureddin et al., Lancet 2025, PMID 41237796) | 212 | 24 wks (48 wks topline) | 58% vs 20% (1.2 mg) | 36% vs ~22%, NS at 24 wks; NITs significant at 48 wks | 7.5% at 48 wks (1.8 mg) | Phase 2b; PERFORMA Phase 3 H2 2026 |
A few honest reads of that table:
- The MASH resolution numbers for semaglutide in ESSENCE and pemvidutide in IMPACT look similar at first glance, but ESSENCE is a 72-week biopsy comparison and IMPACT is 24-week. Time is doing real work here.
- Resmetirom has the only positive fibrosis-improvement primary endpoint in an FDA-approved product so far. Pemvidutide has not cleared that bar on biopsy.
- Weight loss in IMPACT at 48 weeks sits closer to semaglutide territory than to resmetirom territory, which is exactly the mechanistic claim a dual agonist needs to make: glucagon-mediated catabolism plus GLP-1 appetite suppression.
- The IMPACT population is enriched for F2 to F3 fibrosis, similar to MAESTRO-NASH and ESSENCE, which makes the comparison less unfair than it would be if the trials enrolled different stages.
For broader class context, see the ESSENCE Phase 3 semaglutide MASH evidence review and the tirzepatide MASH Phase 2 evidence article. For the oral angle on the rest of the class, see the orforglipron Phase 3 review.
The MASLD and obesity efficacy backstory
The Phase 2b in MASH did not come out of nowhere. Pemvidutide has two earlier Phase 1b MASLD readouts and a Phase 2 obesity readout, all peer-reviewed.
The Phase 1b MASLD 12-week trial (Harrison et al., J Hepatol 2024, PMID 39002641) randomized patients 1:1:1:1 to pemvidutide 1.2, 1.8, or 2.4 mg or placebo. At 12 weeks, relative reductions in liver fat content were 46.6%, 68.5%, and 57.1% versus 4.4% on placebo (P<0.001), with 94.4% of patients on 1.8 mg achieving at least a 30% liver fat reduction. Peak weight loss in that trial was 4.3% on the 1.8 mg dose at 12 weeks. ALT dropped 13.8 IU/L on 1.8 mg.
The 24-week extension (JHEP Reports 2025, PMID 41113119) of the same MASLD trial pushed the liver fat reductions to 56.3%, 75.2%, and 76.4% on the three doses respectively versus 14.0% placebo, with 53.8% of patients on 1.8 mg achieving liver fat normalization (≤5%). Body weight dropped 6.2% on 1.8 mg over 24 weeks.
The MOMENTUM Phase 2 obesity trial enrolled 391 adults with obesity or overweight plus at least one comorbidity, no diabetes, mean BMI 37 kg/m², 75% female, mean age 50. Randomization was to pemvidutide 1.2, 1.8, or 2.4 mg or placebo for 48 weeks. Weight loss at 48 weeks was 10.3%, 11.2%, 15.6%, and 2.2% across the four arms. The body composition piece is the part that drew attention: MRI-based analysis put lean mass loss at roughly 21.9% of total weight lost and fat mass at 78.1%, which Altimmune positioned as class-leading lean mass preservation. That ratio sits in the same neighborhood as natural caloric restriction and below most GLP-1 mono-agonists in published lean mass data. The GLP-1 muscle loss research review puts that context in numbers if the lean mass question is relevant to your read.
Note: The MOMENTUM weight loss and body composition numbers come from oral presentations and press releases, not a primary journal publication, so they sit a tier below the IMPACT and MASLD numbers in evidence strength. Read them as supportive context for the obesity arm of the development program, not as confirmatory efficacy data.
Safety, tolerability, and what to actually watch
Across pemvidutide trials, the safety profile is dominated by GI adverse events that are characteristic of the GLP-1 class: nausea, diarrhea, and vomiting, mostly mild to moderate, peaking in the early weeks of treatment. The notable feature in IMPACT was that pemvidutide was given without dose titration and discontinuation due to adverse events still came in below placebo on both doses (0% and 1% versus 2%). That is unusual in the class. Whether it survives Phase 3 in a larger and more heterogeneous population is the open question.
The glucagon side of the receptor profile has historically raised three specific concerns:
- Hyperglycemia from glucagon-mediated hepatic glucose output
- Increased heart rate
- Increased blood pressure
In MOMENTUM and IMPACT, pemvidutide did not cause meaningful HbA1c worsening in non-diabetic patients, but the trials were not powered to find subtle long-term metabolic effects, and the populations excluded patients with poorly controlled diabetes. Heart rate increases on the order of 4 to 6 bpm have been reported across the dual-agonist class. None of that is disqualifying for an investigational MASH drug, but it is the part of the safety profile that Phase 3 PERFORMA will need to track at scale.
Warning: Pemvidutide is not FDA-approved. It is an investigational compound undergoing Phase 3 development. Any peptide marketed as research-use pemvidutide should be treated with the same skepticism applied to any other unapproved peptide. Until PERFORMA reads out, there is no benchmark for purity, formulation, or human dosing safety outside the controlled trial environment.
Where pemvidutide sits in the 2026 MASH field
The big picture for MASH treatment in mid-2026 has shifted faster than most other liver disease areas. One year ago, resmetirom was the only approved MASH drug. Today, semaglutide 2.4 mg has accelerated FDA approval for biopsy-confirmed MASH with F2 to F3 fibrosis (granted August 2025, contingent on ESSENCE extension data), and the pipeline behind those two is dense: survodutide is in Phase 3 LIVERAGE, retatrutide is moving toward MASH evaluation, tirzepatide has Phase 2 SYNERGY-NASH data, and pemvidutide just earned Breakthrough Therapy designation and is heading into PERFORMA Phase 3 in the second half of 2026.
The differentiation pemvidutide is trying to claim has three parts:
- Dual-mechanism advantage on direct liver fat reduction and weight loss, more like survodutide than like semaglutide
- Lean mass preservation, more favorable than mono-agonist GLP-1 if the MOMENTUM numbers hold up in larger trials
- Tolerability without titration, which would simplify clinical use if confirmed in Phase 3
The points that work against pemvidutide are equally clear. The fibrosis improvement endpoint missed at 24 weeks. The IMPACT sample size was small for the 1.2 mg arm (n=41). Pemvidutide is behind semaglutide in time-to-approval, behind survodutide in glucagon-dose magnitude, and behind resmetirom in mechanism-validated regulatory pathway. The Phase 3 read on biopsy fibrosis is the gating fact.
For researchers building MASH context broader than the dual-agonist story, the ESSENCE Phase 3 semaglutide MASH evidence covers the GLP-1 mono-agonist read, the tirzepatide SYNERGY-NASH Phase 2 article covers the GLP-1/GIP angle, and the survodutide trial evidence covers the closest mechanistic neighbor. For the triple-agonist alternative, the retatrutide TRIUMPH-1 Phase 3 article covers the highest-magnitude weight loss data in the class.
What researchers should watch next
The three datapoints that matter most for pemvidutide over the next 12 months:
- PERFORMA Phase 3 trial initiation and design specifics in the second half of 2026. The endpoint structure (biopsy at what week, MASH resolution and fibrosis improvement as separate or composite endpoints) will tell you what Altimmune learned from IMPACT.
- RECLAIM Phase 2 readout in alcohol use disorder with obesity (NCT06987513), which is the second major indication for pemvidutide. Pemvidutide holds FDA Fast Track designation for AUD in addition to MASH.
- Any direct head-to-head against semaglutide or resmetirom. None is currently scheduled, but the field is competitive enough that one would reshape the prescribing conversation if it happened.
The cleanest read for now: pemvidutide cleared the MASH resolution bar in a Lancet-published Phase 2b, missed the fibrosis biopsy bar at 24 weeks but separated clearly on non-invasive markers at 48 weeks (with digital-pathology supportive evidence at 24 weeks), and is heading into Phase 3 with a tolerability profile that the rest of the class has not matched without titration. Treat the 2026 readouts as encouraging rather than confirmatory until PERFORMA closes the biopsy story.
Researchers studying GLP-1 mechanism in MASH-adjacent biology can source FDA-approved semaglutide (the only GLP-1 currently approved for MASH) through Ascension Peptides with 50% off using code ENHANCED. The COA matters more than the price, and the relevant comparator for any pemvidutide-class research question is the approved benchmark, not a research-grade copy of an investigational molecule that has not finished Phase 3.
This article is for educational and research purposes only. It summarizes published Phase 1b, Phase 2, and Phase 2b trial data, press-release topline announcements, and conference abstracts. Pemvidutide is an investigational compound and is not FDA-approved for any indication. Trial data on the comparator drugs (semaglutide, tirzepatide, survodutide, resmetirom) are abstracted from the cited primary publications and have not been independently re-analyzed. This is not medical advice. Do not start, stop, or change any medication based on this article. Investigational and research-use peptides are not intended for human use.