At a glance
- Semax is a synthetic ACTH(4-10) analog used in Russian neurology for stroke and cognitive disorders; it is not FDA-approved.
- A single 50 mcg/kg dose raised hippocampal BDNF protein 1.4-fold and exon III BDNF mRNA 3-fold in rats (Dolotov et al. 2006).
- Radiolabeled Semax binds brain tissue specifically and reversibly (KD 2.4 nM) and lifts basal forebrain BDNF within 3 hours (Dolotov et al. 2006).
- Human evidence is limited and almost entirely Russian: a 1997 acute-stroke study (30 treated vs 80 controls) reported faster motor recovery.
- No independent Western double-blind RCT has confirmed the cognitive or stroke findings, so treat human efficacy as unproven.
Semax has been used in Russian neurology clinics for almost thirty years. It has close to zero independent trials outside Russia. Both statements are true, and the distance between them is the entire reason this peptide is hard to evaluate.
Most vendor pages skip that tension. They cite the BDNF numbers, mention stroke recovery, and stop there. What follows is the actual published record: which claims have real data behind them, which rest on a single Russian study, and which have no human evidence at all.
Bottom line: The preclinical case that Semax engages the brain's BDNF system is genuinely solid. The case that it reliably improves cognition or stroke recovery in people rests on small, mostly Russian studies that no Western group has replicated under double-blind conditions.
What Semax actually is
Semax is a synthetic heptapeptide with the sequence Met-Glu-His-Phe-Pro-Gly-Pro. The first residues copy a fragment of adrenocorticotropic hormone (ACTH); the trailing Pro-Gly-Pro tail was added to slow enzymatic breakdown so the molecule survives long enough to act. It was developed at the Institute of Molecular Genetics of the Russian Academy of Sciences by Nikolay Myasoedov's group.
Stripping ACTH down to that fragment removes the hormonal (corticotropic) activity while keeping the neurotropic effects, so Semax does not raise cortisol the way full-length ACTH would. In Russia it is registered for ischemic stroke and a range of cognitive and neurological indications, and it appears on the country's list of vital and essential medicines. It is delivered intranasally, which sidesteps the gut and gives the peptide a short route toward the brain.
Outside Russia the regulatory status is simpler: there is none. Semax is not approved by the FDA or EMA, and in Western markets it is sold for laboratory research only. The peptide profile for Semax covers the structural details; this article is about the evidence.
Note: Two stabilized variants circulate in research markets, N-acetyl Semax and N-acetyl Semax amidate. The acetylation and amidation slow degradation further and are marketed as longer-acting. The human data discussed below were generated with plain Semax, so do not assume the modified versions behave identically.
The BDNF mechanism: what the rat data show
The most reproducible finding about Semax is that it raises brain-derived neurotrophic factor (BDNF), the growth factor most tied to synaptic plasticity and neuronal survival.
In rat hippocampus, a single 50 mcg/kg dose of Semax produced a 1.4-fold rise in BDNF protein, a 3-fold rise in exon III BDNF mRNA, and a 1.6-fold increase in phosphorylation of the TrkB receptor that BDNF signals through (Dolotov et al., Brain Research 2006, PMID 16996037). The mRNA jump matters because it points to Semax driving new BDNF transcription rather than only releasing an existing pool.
A companion paper from the same year went looking for a binding site. Using tritium-labeled Semax, the group found specific, reversible, calcium-dependent binding in rat basal forebrain with a dissociation constant of 2.4 nM, and showed that intranasal doses of 50 and 250 mcg/kg raised basal forebrain BDNF within three hours while the cerebellum did not respond (Dolotov et al., Journal of Neurochemistry 2006, PMID 16635254). A nanomolar dissociation constant and a region-specific response are what you would expect from a real receptor interaction rather than a nonspecific effect.
Ischemia models extend the picture. In rats with permanent middle cerebral artery occlusion, Semax increased transcription of Bdnf, TrkC, and TrkA three hours after the occlusion and of NT-3 and NGF at 24 hours; the C-terminal Pro-Gly-Pro fragment alone produced mostly nonspecific changes, which suggests the intact peptide is doing the selective work (Medvedeva et al., Cellular and Molecular Neurobiology 2010, PMID 19633950). A later genome-wide analysis in the same model found that the gene programs Semax shifted most were immune response and vascular system genes, including chemokines and factors tied to blood vessel formation (Medvedeva et al., BMC Genomics 2014, PMID 24661604).
Read together, four animal studies converge on a consistent mechanism: Semax engages the neurotrophin system and tilts the post-ischemic environment toward repair. Every one of those studies is in rats.
How strong is the evidence, really?
Not all Semax claims carry the same weight. Sorting them by the strongest available source makes the gaps obvious.
| Claim | Strongest evidence | Evidence tier |
|---|---|---|
| Raises BDNF and related neurotrophins in brain tissue | Dolotov 2006 (two studies), Medvedeva 2010 | Strong preclinical (animal) |
| Binds a specific brain site (KD 2.4 nM) | Dolotov 2006, J Neurochem | Moderate preclinical (animal) |
| Shifts immune and vascular gene programs after ischemia | Medvedeva 2014, genome-wide | Strong preclinical (animal) |
| Speeds neurological recovery after ischemic stroke | Skvortsova and Gusev 1997 clinical study | Weak to moderate human (non-RCT) |
| Improves attention and memory in healthy adults | Kaplan et al. 1996 | Weak human (small, not PubMed-indexed) |
| Approved or proven in a Western RCT | none | No evidence |
The pattern is clear. The mechanism sits on solid animal work. The human claims that draw people to Semax sit on a much thinner base.
The human evidence: stroke and cognition
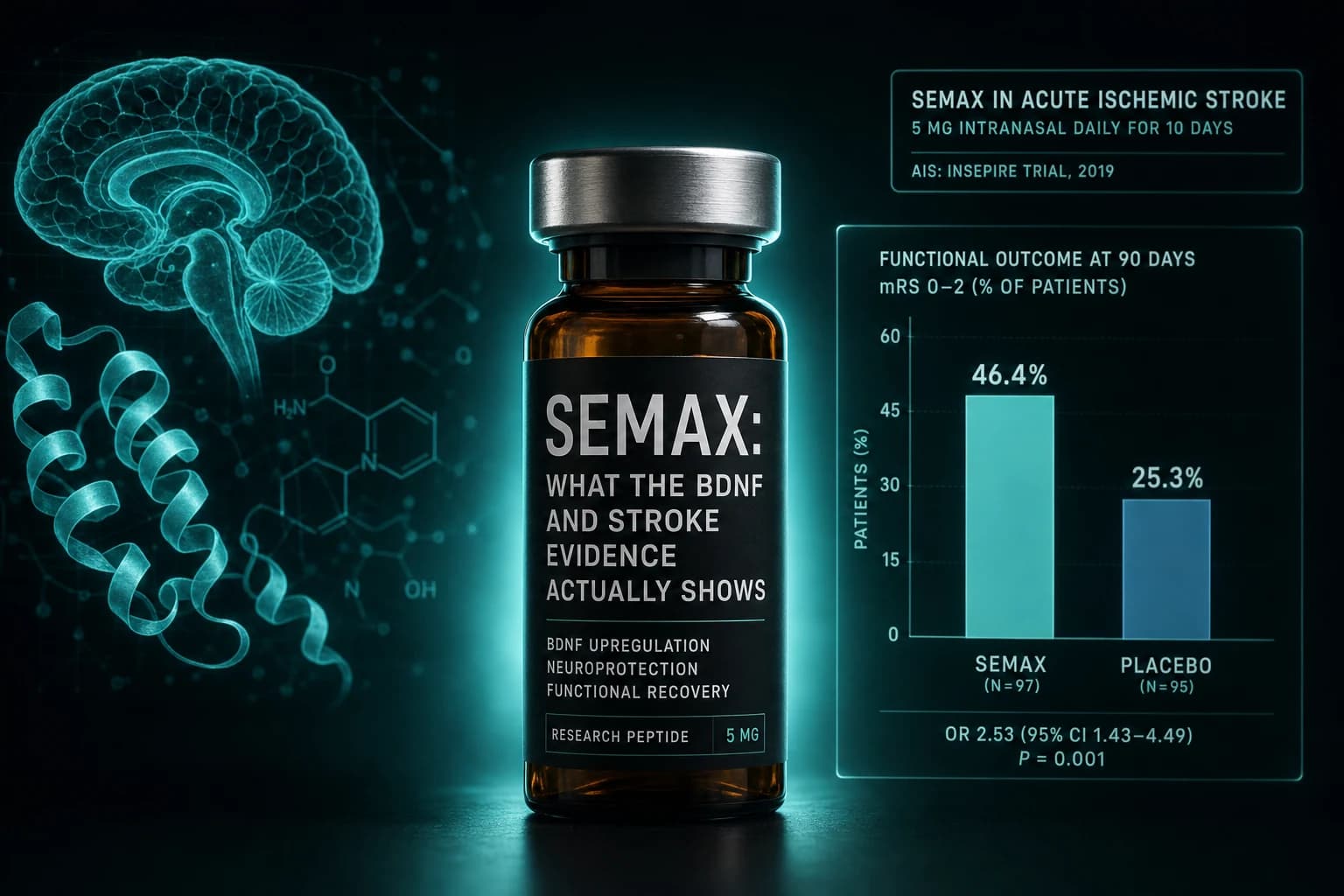
Stroke is the indication with the most human support, and it is still modest. A controlled clinical study added Semax to standard care for 30 patients in the acute phase of hemispheric ischemic stroke and compared them with 80 patients on conventional therapy alone, reporting faster regression of motor deficits and supportive electrophysiological changes (Skvortsova, Gusev et al., Zhurnal Nevrologii i Psikhiatrii 1997, PMID 11517472). That is a real clinical signal, but the design was not double-blind, the groups were not randomized one to one, the sample was small, and the literature exists almost entirely in Russian. None of that makes the finding wrong. It does mean it has never cleared the bar that Western stroke neurology requires.
Cognition is thinner still. The most cited human nootropic report gave healthy volunteers intranasal Semax at roughly 16 mcg/kg and recorded improved attention and short-term memory along with EEG changes resembling those of established nootropic drugs (Kaplan et al., Neuroscience Research Communications 1996). That study is small, comes from the same Moscow research lineage that developed the peptide, and is not clearly indexed in PubMed, so read it as preliminary rather than confirmatory.
Warning: No large, independent, double-blind, placebo-controlled trial of Semax has been published in a major international journal for any indication. Decades of Russian clinical use is real-world experience. That is different from replicated trial evidence. Anyone telling you Semax is "proven" for memory or stroke is overstating the record.
Semax vs Selank vs dihexa
The three peptides nootropics researchers most often compare share a problem: strong mechanistic stories, weak human trials. They differ in what they target.
| Compound | Origin and class | Proposed main mechanism | Best-supported endpoint | Independent human RCT | Usual route |
|---|---|---|---|---|---|
| Semax | ACTH(4-10) analog (Russia) | BDNF and NGF upregulation, dopaminergic tone | Neuroprotection and attention (animal-led) | None | Intranasal |
| Selank | Tuftsin analog (Russia) | GABA and serotonin modulation, anxiolytic | Anxiety reduction | Limited, Russian | Intranasal |
| Dihexa | Angiotensin IV analog (US) | HGF and c-Met driven synaptogenesis | New synapse formation (animal) | None | Oral or transdermal |
Semax and Selank are siblings from the same Russian neuropeptide program and are frequently paired, which is why several vendors sell them as a single nasal blend. If anxiety is the target, the Selank dosing and route comparison is the more relevant read. If the interest is raw synaptogenesis, the dihexa evidence audit walks through why its preclinical numbers look dramatic and why that has not translated to people yet. For neurorestorative protocols with more human data behind them, cerebrolysin is the better-studied option.
Dosing as it appears in the research literature
This section describes what published studies and registered Russian formulations used. It is not a protocol, and none of it is validated for human use outside Russia.
The animal mechanism work used 50 to 250 mcg/kg intranasally (Dolotov 2006). The healthy-volunteer cognitive report used roughly 16 mcg/kg intranasally, which lands near 1 mg for a 60 kg adult (Kaplan 1996). Russia's registered products are nasal solutions standardized by concentration: a lower-strength formulation for cognitive and neurological use and a higher-strength one reserved for acute stroke. The N-acetyl and amidated variants sold in research markets are pitched as longer-acting, but the human data above were not generated with them.
If a research peptide arrives lyophilized, it has to be reconstituted before any accurate volume can be drawn. Our reconstitution calculator handles the math so a stated microgram dose maps to an actual draw volume.
Tip: Intranasal peptides are sensitive to volume. A nasal cavity holds only a small liquid load before the excess drains down the throat and is wasted, so research protocols favor higher concentrations in smaller drops rather than large volumes.
Safety and the honest unknowns
Short Russian studies describe Semax as well tolerated, with no corticotropic side effects and few reported adverse events at the doses used. That is reassuring as far as it goes, and it does not go far. There is no long-term controlled safety data, no large pharmacovigilance system tracking it the way approved drugs are tracked, and meaningful batch-to-batch variability across research-grade peptide supply. Animal tolerability over days or weeks says little about chronic human use across months.
Where Semax fits
The honest summary is narrow. Semax has a credible, repeatedly demonstrated effect on the BDNF and neurotrophin system in rodents, a plausible neuroprotective profile in ischemia models, and a long Russian clinical history that points in a hopeful direction without ever proving it. The people who research it tend to want attention, mental stamina, or recovery support, and they accept that they are working ahead of the trial evidence.
Pairing with Selank is the most common configuration, which is why the Calm and Clarity cognitive stack groups these neuropeptides rather than treating them in isolation. The intranasal Semax and Selank formats sold for research are carried by Limitless Biotech, including a combined N-acetyl Semax and N-acetyl Selank nasal spray; their nasal spray catalog takes code ENHANCED at checkout. Treat anything you source as a research material, not a supplement.
Frequently asked questions
Is Semax FDA-approved? No. It is approved and used in Russia for stroke and cognitive indications and appears on Russia's essential medicines list, but it has no FDA or EMA approval and is sold elsewhere for research only.
Does Semax actually raise BDNF? In rats, yes, repeatedly and measurably (Dolotov 2006). Whether intranasal dosing produces a meaningful BDNF change in healthy humans has not been shown directly in a controlled trial.
Is Semax or Selank better for focus? They target different problems. Semax is studied more for attention and neuroprotection, Selank more for anxiety. Neither has independent Western RCT support for cognitive enhancement.
This article is for educational and research purposes only. Semax is approved in Russia for stroke and cognitive indications but is not approved by the FDA or EMA, and outside Russia it is sold for laboratory research use only. The human studies discussed are small, largely Russian-language, and have not been replicated in independent double-blind trials, so none of the findings establish clinical efficacy or safety. Nothing here is medical advice. Consult a qualified clinician before making any decision related to cognition, stroke risk, or peptide use.