At a glance
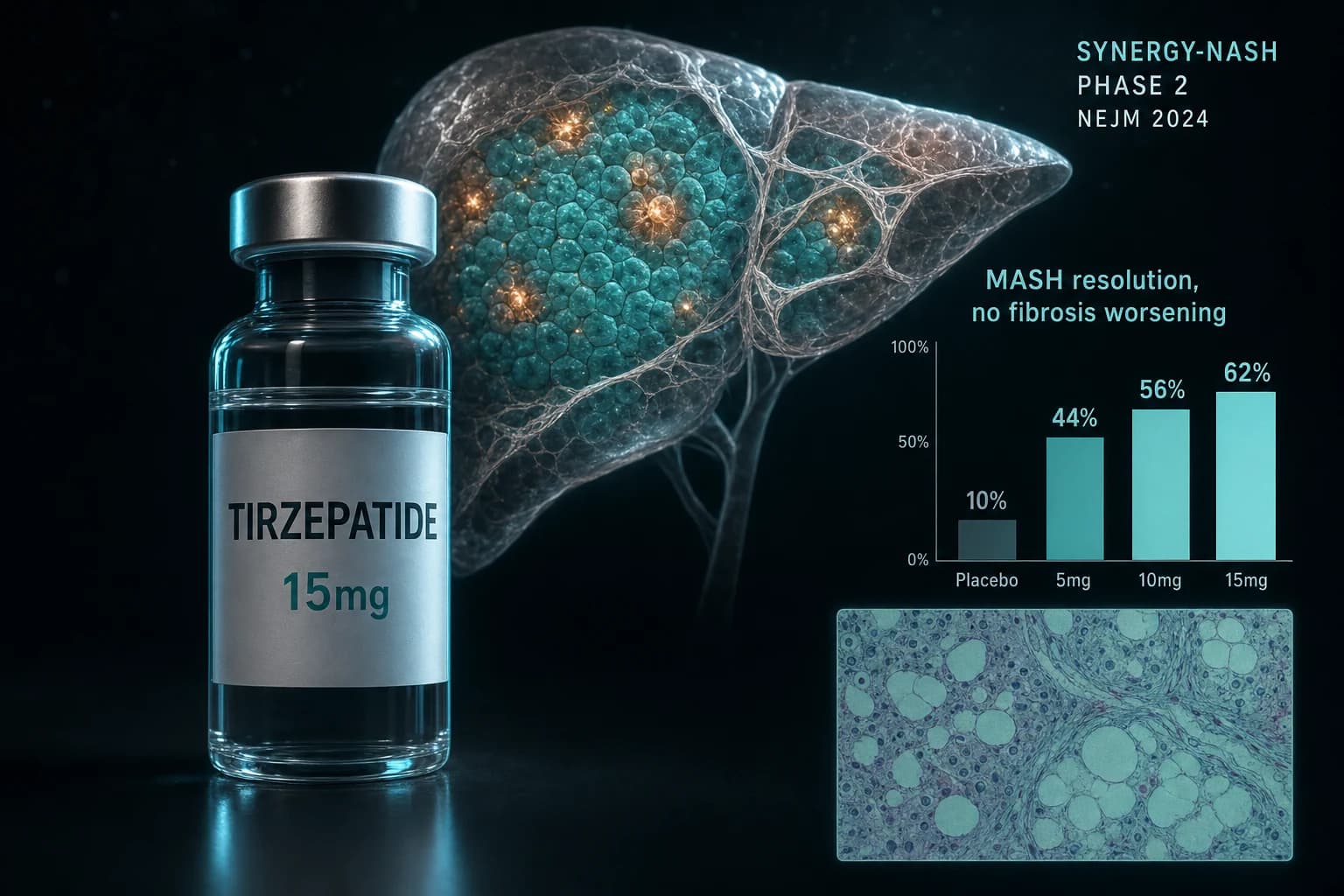
- SYNERGY-NASH Phase 2 (Loomba et al. NEJM 2024, PMID 38856224): MASH resolution without fibrosis worsening hit 62% on 15 mg tirzepatide vs 10% on placebo at 52 weeks
- Fibrosis improvement by at least 1 stage without MASH worsening landed at 51-55% across the three tirzepatide doses vs 30% on placebo, with no clear dose response
- n = 190 biopsy-confirmed F2-F3 MASH adults, 59% with type 2 diabetes, 130 sites in 10 countries; the trial was designed for Phase 2 dose-finding, not regulatory approval
- SURPASS-3 MRI substudy (Gastaldelli et al. Lancet Diabetes Endocrinol 2022, PMID 35468325): pooled tirzepatide 10/15 mg cut MRI-PDFF liver fat by 8.09% absolute vs 3.38% on insulin degludec
- Phase 3 SYNERGY-NASH-2 is enrolling under FDA breakthrough therapy designation; resmetirom remains the only oral with an FDA MASH label
TL;DR: tirzepatide hit MASH resolution endpoints no other peptide has matched
In the 190-patient SYNERGY-NASH Phase 2 trial, 15 mg tirzepatide resolved MASH without worsening fibrosis in 62% of biopsy-confirmed F2/F3 adults at 52 weeks. Placebo hit 10%. Fibrosis improvement by at least one stage without MASH worsening landed at 51% on 15 mg vs 30% on placebo (Loomba et al. NEJM 2024, PMID 38856224).
Those numbers came out of a Phase 2 trial. They will compress in Phase 3, as Phase 2 numbers in MASH almost always do. Even compressed, they remain the strongest published incretin signal in liver biopsy MASH trials to date, which is why Lilly's Phase 3 SYNERGY-NASH-2 is enrolling under an FDA breakthrough therapy designation.
This article walks through what the trial measured, what the data actually show, how tirzepatide compares to the only oral MASH drug currently approved by the FDA (resmetirom), and where the GIP/GLP-1 mechanism may or may not be doing useful work in the liver itself.
What MASH is and why most peptides do nothing for it
Metabolic dysfunction-associated steatohepatitis (MASH, formerly NASH) sits at the inflammatory end of fatty liver disease. The pathology requires three components on biopsy: steatosis (fat), hepatocyte ballooning (cell injury), and lobular inflammation. Once fibrosis stages reach F2 or F3, mortality risk climbs sharply.
Among adults with type 2 diabetes, pooled global NAFLD prevalence is roughly 65%, with 40-66% of biopsied patients showing MASH and around 15% showing advanced fibrosis (Younossi et al. Clin Gastroenterol Hepatol 2024, PMID 38521116). MASH is the fastest-growing cause of liver transplant in the United States.
Until March 2024, no drug was FDA approved for MASH. Resmetirom (Rezdiffra), a thyroid hormone receptor beta agonist, broke that barrier under accelerated approval (Harrison et al. NEJM 2024, PMID 38324483). The Phase 3 bar it set: 26-30% MASH resolution at 80-100 mg vs 10% on placebo at 52 weeks. Tirzepatide's Phase 2 number at 15 mg is roughly double that.
Bottom line: the existing approved option (resmetirom) hits about 1 in 4 patients with MASH resolution. SYNERGY-NASH put tirzepatide 15 mg at 6 in 10. Phase 2 numbers shrink in Phase 3, so the question is not whether tirzepatide helps MASH but by how much.
SYNERGY-NASH: the trial design
SYNERGY-NASH was a multicenter, randomized, double-blind, placebo-controlled Phase 2b trial in 190 adults with biopsy-confirmed MASH and stage F2 or F3 fibrosis across 130 sites in 10 countries (Hartman et al. Aliment Pharmacol Ther 2024, PMID 38768298). Participants were randomized 1:1:1:1 to placebo or once-weekly subcutaneous tirzepatide at 5 mg, 10 mg, or 15 mg for 52 weeks. Baseline characteristics: 59% had type 2 diabetes, mean BMI was 35.7 kg/m², and the cohort was enriched for stage F2 and F3 fibrosis.
The two co-primary endpoints were the FDA-recognized histologic endpoints for MASH trials:
- Resolution of MASH without worsening of fibrosis
- Improvement of fibrosis by at least one stage without worsening of MASH
Both endpoints require central pathologist review of paired pre- and post-treatment biopsies. Of 190 randomized participants, 157 had evaluable week-52 biopsies.
The headline endpoint numbers
The primary endpoint result was clean.
| Group | MASH resolution, no fibrosis worsening | Fibrosis ≥1 stage improvement, no MASH worsening |
|---|---|---|
| Placebo (n=47) | 10% | 30% |
| Tirzepatide 5 mg (n=47) | 44% | 55% |
| Tirzepatide 10 mg (n=48) | 56% | 51% |
| Tirzepatide 15 mg (n=48) | 62% | 51% |
All three tirzepatide doses beat placebo on MASH resolution at P<0.001. The fibrosis endpoint, while numerically higher across all tirzepatide doses, did not show a dose response across 5-15 mg.
The "treatment-policy estimand" numbers shown above include participants who discontinued treatment. Under the "efficacy estimand" (excluding intercurrent events like treatment discontinuation), the 15 mg MASH resolution rate climbs to roughly 73%. Neither version is a clinical claim. Both should compress in a Phase 3 trial with a longer placebo arm and a broader fibrosis distribution.
Note: Phase 2 trials almost always overstate effect size. Placebo response in MASH biopsy trials runs from 5% to 25% across studies, partly because biopsy interpretation has inter-rater variability and partly because lifestyle intervention is baked into every study protocol.
What happened to weight, MRI-PDFF, and biomarkers
Histologic effect tracked weight loss closely. Mean body weight changes were minus 11.6% (5 mg), minus 16.7% (10 mg), and minus 16.4% (15 mg) vs minus 1.8% on placebo over 52 weeks. Liver fat by MRI-PDFF dropped substantially across all tirzepatide arms, with the 10 mg and 15 mg arms approaching a steatosis-resolution rate (MRI-PDFF below 5%) in the majority of treated participants.
A participant-level exploratory analysis published a year later showed that biomarker improvements (fasting adiponectin rise, ALT decline, MRI-PDFF reduction) were significantly larger in histologic responders than nonresponders, both within and outside the T2D subgroup (SYNERGY-NASH exploratory analysis, Diabetes Care 2025, PMID 41066427). Adiponectin gain in responders with T2D was 44.2% vs 22.5% in nonresponders (P = 0.025).
This is the open scientific question. Does tirzepatide help MASH because of weight loss, because of direct hepatic effects, or both?
Mechanism: GIP plus GLP-1 in a liver context
The textbook view is that hepatocytes do not express GLP-1 receptors or GIP receptors meaningfully. Glucagon receptors are abundantly expressed in the liver. So most of the apparent liver effect of incretin agonists has been attributed to systemic mechanics: weight loss, improved insulin sensitivity, lower visceral fat, reduced delivery of free fatty acids to the liver.
Newer preclinical work complicates that view. A 2025 study in MASLD mice reported that tirzepatide reduced hepatic expression of CD36 and OBP2A, two proteins involved in fatty-acid uptake into hepatocytes (Chen et al. Heliyon 2025, PMID 40837406). Whether that mechanism is truly direct on hepatocytes or indirect (via Kupffer cells, hepatic stellate cells, or adipose tissue crosstalk) is unsettled.
The earlier SURPASS-3 MRI substudy in adults with type 2 diabetes gave a clean liver-fat signal: pooled tirzepatide 10 mg and 15 mg cut absolute MRI-PDFF by 8.09% vs 3.38% on insulin degludec from a baseline mean of 15.71% (Gastaldelli et al. Lancet Diabetes Endocrinol 2022, PMID 35468325). At week 52, 41.3% of pooled tirzepatide participants had MRI-PDFF below 5% (the steatosis cutoff) vs 9.6% on insulin degludec.
For an entry point on why dual GIP/GLP-1 agonism behaves differently from pure GLP-1 monotherapy, our MariTide GIP antagonism mechanism deep dive covers GIP biology in more detail and lays out the case for why even GIP antagonism produces similar metabolic effects to GIP agonism on a long enough timescale.
Tirzepatide vs semaglutide vs resmetirom for MASH
The three drugs with biopsy-grade MASH evidence are all different mechanisms. Trial designs differ, follow-up windows differ, and the underlying populations differ. The numbers below are not perfectly comparable; they are reference values from each pivotal trial.
| Drug | Trial | Phase | n | Duration | MASH resolution, no fibrosis worsening | Fibrosis ≥1 stage improvement |
|---|---|---|---|---|---|---|
| Resmetirom 100 mg oral daily | MAESTRO-NASH | 3 | 966 | 52 wk | 29.9% (vs 9.7% placebo) | 25.9% (vs 14.2% placebo) |
| Semaglutide 2.4 mg SC weekly | ESSENCE (72-wk interim) | 3 | 1,197 | 72 wk | 32.7% combined endpoint | 36.8% (vs 22.4% placebo) |
| Tirzepatide 15 mg SC weekly | SYNERGY-NASH | 2 | 190 | 52 wk | 62% (vs 10% placebo) | 51% (vs 30% placebo) |
Resmetirom is the only drug here with FDA approval for MASH (Harrison et al. NEJM 2024, PMID 38324483). Semaglutide cleared its Phase 3 ESSENCE interim primary endpoints on fibrosis improvement and MASH resolution; we cover the trial in detail in our semaglutide ESSENCE MASH article. Tirzepatide's Phase 3 program is still enrolling.
A direct head-to-head between tirzepatide and either competitor in MASH does not exist. The 62% vs 30% spread looks dominant on paper, but the SYNERGY-NASH cohort was smaller, had higher baseline diabetes prevalence, and produced markedly larger weight loss than the ESSENCE or MAESTRO-NASH cohorts. Weight loss alone may explain most of the histologic gap.
Bottom line: if the field cares about absolute weight-adjusted hepatic effect, tirzepatide and semaglutide are likely closer than the raw numbers suggest. If the field cares about overall MASH response across an unselected population, tirzepatide's signal is the strongest published incretin number to date, by a clear margin.
The fibrosis question Phase 2 could not answer
Note the gap between primary and secondary endpoint behavior in SYNERGY-NASH. MASH resolution scaled cleanly with dose (44% on 5 mg, 56% on 10 mg, 62% on 15 mg). Fibrosis improvement did not (55%, 51%, 51%). All three doses beat placebo on fibrosis (30%), but there was no dose response.
Two reasonable interpretations exist. One: fibrosis is downstream of inflammation, so once MASH resolves the fibrosis benefit plateaus regardless of dose. Two: 52 weeks is too short for collagen turnover, and a longer trial would surface the true fibrosis dose response. Both are speculation. The Phase 3 SYNERGY-NASH-2 trial has a longer follow-up window and is powered for fibrosis as a primary endpoint.
Until that readout, claims that tirzepatide "reverses liver fibrosis" run ahead of what the Phase 2 data actually showed. The honest statement: fibrosis improved by at least one stage in roughly half of treated participants vs 30% on placebo, with no clear dose dependence, in a 52-week Phase 2 trial.
Practical implications for tirzepatide users with fatty liver
Tirzepatide is approved as Mounjaro for type 2 diabetes, as Zepbound for chronic weight management, and as Zepbound for moderate-to-severe obstructive sleep apnea in adults with obesity. It is not approved for MASH. Off-label use is occurring, but no current label supports the indication.
For research-context users of injectable tirzepatide (compounded supply remains a moving regulatory target, covered in our compounded tirzepatide 2026 access guide), the SYNERGY-NASH dose range was 5-15 mg subcutaneously once weekly. The standard titration used in the trial mirrored SURPASS and SURMOUNT: 2.5 mg for 4 weeks, then 5 mg for 4 weeks, then escalation every 4 weeks to the assigned target dose.
The reconstitution calculator handles US-unit conversion on the standard 10 mg and 15 mg vial volumes. Weekly mg targets across the GLP-1 class sit in our GLP-1 dosing comparison 2026 piece.
Three things to know before assuming the SYNERGY-NASH numbers apply to a single individual:
- SYNERGY-NASH excluded cirrhotic patients. Anyone with F4 fibrosis or compensated cirrhosis was not enrolled. The drug has not been tested at this stage in MASH.
- The trial required biopsy-confirmed F2/F3 disease. MRI-PDFF and FIB-4 alone do not identify the same population, and elastography varies. Without a tissue diagnosis, the trial response rates are not directly transferable.
- Hepatic effect tracked tightly with weight loss. Tirzepatide responders who do not lose weight (a minority) had smaller histologic improvements. This is the "weight-mediated vs direct effect" question that Phase 3 is designed to disentangle.
Tirzepatide for injectable research use is available from Ascension Peptides at 50% off with code ENHANCED.
Safety in the SYNERGY-NASH window
The adverse event profile in SYNERGY-NASH matched the SURPASS and SURMOUNT data: gastrointestinal events were the main signal, most mild to moderate, with the highest incidence on 15 mg. Discontinuation due to adverse events ran 6-7% across the three tirzepatide arms vs 2% on placebo. No new hepatic safety signal emerged in the 52-week window. ALT and AST trended down across tirzepatide arms, consistent with reduced liver injury.
One important caveat carries over from the broader obesity literature. Tirzepatide reduces lean mass alongside fat mass. Whether that lean mass loss matters for MASH outcomes specifically is unclear; the exploratory data show responders had larger fat mass loss than nonresponders but did not separate cleanly on lean mass change. We cover the lean mass preservation question separately in our GLP-1 muscle loss research review.
What is next: SYNERGY-NASH-2 and the Phase 3 design
Lilly initiated the Phase 3 program for tirzepatide in MASH following the SYNERGY-NASH readout. The Phase 3 trial uses biopsy-confirmed MASH with F2/F3 fibrosis, a longer treatment window than 52 weeks, and dual primary histologic endpoints (MASH resolution and fibrosis improvement). It is expected to include compensated cirrhosis (F4) substudies that the Phase 2 trial excluded.
The FDA granted tirzepatide breakthrough therapy designation for MASH. That status accelerates review timelines but does not change the evidentiary bar. Phase 3 must replicate the Phase 2 signal on a larger, more diverse population over a longer window before any approval moves forward.
For now, the practical takeaway is narrow. Tirzepatide's Phase 2 MASH numbers are the strongest published incretin signal in this disease. Phase 3 confirmation is not yet here, and Phase 2 results in MASH have over-promised relative to Phase 3 outcomes more than once before (obeticholic acid, selonsertib, simtuzumab, cenicriviroc).
Bottom line: tirzepatide is a strong Phase 2 candidate for MASH with FDA breakthrough designation. It is not approved for MASH. Resmetirom remains the only oral with an FDA MASH label. Semaglutide's Phase 3 ESSENCE data carry more regulatory weight in absolute terms because they come from a larger, longer trial.
Quick reference and related reading
- Tirzepatide compound profile, mechanism, and approved indications: tirzepatide peptide page
- Semaglutide MASH parallel trial: semaglutide ESSENCE Phase 3 MASH evidence
- Tirzepatide cardiac evidence: tirzepatide HFpEF SUMMIT trial article
- Broader semaglutide compound profile: semaglutide peptide page
References
- Loomba R, Hartman ML, Lawitz EJ, et al. Tirzepatide for Metabolic Dysfunction-Associated Steatohepatitis with Liver Fibrosis. N Engl J Med. 2024;391(4):299-310. PMID 38856224
- Hartman ML, Sanyal AJ, Loomba R, et al. Design of the SYNERGY-NASH phase 2b trial to evaluate tirzepatide as a treatment for metabolic dysfunction-associated steatohepatitis and modification of screening strategy to reduce screen failures. Aliment Pharmacol Ther. 2024. PMID 38768298
- Gastaldelli A, Cusi K, Fernández Landó L, et al. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI). Lancet Diabetes Endocrinol. 2022;10(6):393-406. PMID 35468325
- Harrison SA, Bedossa P, Guy CD, et al. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis. N Engl J Med. 2024;390(6):497-509. PMID 38324483
- Younossi ZM, Golabi P, Paik JM, et al. The Global Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis Among Patients With Type 2 Diabetes. Clin Gastroenterol Hepatol. 2024. PMID 38521116
- SYNERGY-NASH Investigators. Relationship Between Metabolic and Histological Responses in People With Metabolic Dysfunction-Associated Steatohepatitis With and Without Type 2 Diabetes: Participant-Level Exploratory Analysis of the SYNERGY-NASH Trial With Tirzepatide. Diabetes Care. 2025. PMID 41066427
- Chen et al. Tirzepatide, a dual GIP/GLP-1 receptor agonist, alleviates metabolic dysfunction-associated steatotic liver disease by reducing the expression of CD36 and OBP2A. Heliyon. 2025. PMID 40837406
This article is for educational and research purposes only. None of the content above constitutes medical advice. Tirzepatide is FDA approved as Mounjaro for type 2 diabetes and as Zepbound for chronic weight management and for moderate-to-severe obstructive sleep apnea in adults with obesity; it is not approved for MASH. The histologic, biomarker, and dosing numbers above describe what published trials measured under controlled conditions; they do not establish efficacy or safety for any specific individual and they are not protocols. Decisions about fatty liver evaluation and pharmacotherapy belong with the patient and a qualified hepatologist.