At a glance
- No peptide has energy as a validated clinical endpoint yet.
- MOTS-c and 5-Amino-1MQ evidence is mostly mouse data, not human trials.
- NMN raised muscle insulin sensitivity in prediabetic women (Yoshino 2021).
- Elamipretide (SS-31) missed its primary endpoints in the MMPOWER-3 trial.
- MK-677 boosts slow-wave sleep ~50%, an indirect route to daytime energy.
Search "best peptide for energy" and you get a ranked list with zero caveats. That list is almost always wrong, because "energy" was never the endpoint any of these compounds was measured against.
What researchers actually study is narrower and more useful: mitochondrial ATP output, NAD+ availability, insulin sensitivity, and sleep architecture. Fix one of those and subjective energy often follows. So the honest question is not "which peptide gives energy" but "which mechanism is broken, and what has real data behind targeting it."
This is a research-first map of the compounds people file under energy peptides, what each one does at the cellular level, and how strong the evidence actually is. Spoiler: most of it is preclinical or indirect, and two of the six are not even peptides.
Why "energy" is a slippery endpoint
Fatigue is subjective. Trials rarely measure "energy" as a number; they measure walk distance, VO2, glucose disposal, or validated fatigue scales. A compound can raise a mitochondrial marker in a dish and still do nothing you can feel. That gap between mechanism and outcome is where most peptide energy claims quietly fall apart.
Keep two questions in mind for every compound below. First, is the evidence human or animal? Second, did anyone measure something a person would recognize as energy, or just a surrogate marker upstream of it?
The compounds at a glance
| Compound | Mechanism relevant to energy | Evidence level | Format |
|---|---|---|---|
| MOTS-c | Mitochondrial-derived peptide, activates AMPK, exercise-mimetic in animals | Preclinical (mouse); no human energy trial | Injectable (SC) |
| 5-Amino-1MQ | NNMT inhibitor, spares nicotinamide to preserve the NAD+ pool | Preclinical (mouse) only | Oral capsule |
| NAD+ / NMN | Coenzyme for ATP production; NMN precursor raises NAD+ | Early human RCT (metabolic markers, mixed) | Oral (NMN) or IV/injectable (NAD+) |
| SS-31 (elamipretide) | Binds cardiolipin, stabilizes cristae, improves ATP output | Human RCTs; MMPOWER-3 missed primary endpoints | Injectable (SC) |
| CJC-1295 + Ipamorelin | Larger GH/IGF-1 pulse, better sleep and recovery | Human PK data; energy inferred, not measured | Injectable (SC) |
| MK-677 | Oral ghrelin mimetic, raises GH/IGF-1, deepens sleep | Human sleep data; energy indirect | Oral capsule |
MOTS-c: the exercise-mimicking mitochondrial peptide
MOTS-c is a 16-amino-acid peptide encoded inside mitochondrial DNA rather than the nucleus. That detail matters: it is one of a small set of true mitochondrial-derived peptides, and its role is metabolic signaling. In mice, MOTS-c activates the AMPK pathway, improves insulin sensitivity, and protects against both diet-induced and age-related insulin resistance (Lee et al. (2015)).
The energy hook comes from a later study showing MOTS-c behaves like an exercise mimetic. Injected MOTS-c improved running capacity and physical performance in young, middle-aged, and old mice, and endogenous levels rose after exercise in both mice and humans (Reynolds et al. (2021)).
Here is the catch. Both landmark papers are animal work. No published human trial has measured MOTS-c against fatigue, VO2 max, or perceived energy. The mechanism is real and well-characterized; the human efficacy data is not there yet. Researchers typically run 5 to 10 mg subcutaneously a few times per week, and the MOTS-c dosing chart covers the reconstitution math.
5-Amino-1MQ: protecting your NAD+ pool
First honesty check: 5-Amino-1MQ is not a peptide. It is a small-molecule inhibitor of NNMT (nicotinamide N-methyltransferase), the enzyme that chews through nicotinamide, a direct NAD+ precursor. Block NNMT and, in theory, you spare raw material for NAD+ production while nudging cellular energy metabolism.
The data is entirely preclinical. In diet-induced obese mice, NNMT inhibitors reduced body weight and white fat mass and improved metabolic markers without changing food intake (Neelakantan et al. (2018)). No human trial has tested 5-Amino-1MQ for energy, fat loss, or NAD+ status.
It is sold as an oral capsule, usually around 50 mg daily in research settings. Treat the metabolic and NAD+ story as a promising mouse hypothesis, not a proven human effect.
NAD+ and NMN: the cofactor everyone talks about
NAD+ is the coenzyme every mitochondrion needs to turn food into ATP. Levels decline with age, which is why NAD+ and its precursor NMN dominate longevity forums. Raising NAD+ directly is hard because the molecule is large and unstable, so most research uses precursors like NMN or NR, or intravenous NAD+.
The strongest human signal comes from a 2021 randomized, placebo-controlled trial: 10 weeks of oral NMN increased skeletal-muscle insulin sensitivity in prediabetic, overweight or obese women (Yoshino et al. (2021)). That is a metabolic endpoint, not an energy one, and several other markers did not move. NMN raises NAD+ metabolites reliably; whether that translates into how you feel is still unsettled.
Injectable and IV NAD+ are popular in clinics but carry almost no controlled data behind the energy and "brain fog" claims attached to them. The precursor route (oral NMN) has better human evidence than the injectable route.
SS-31 (elamipretide): stabilizing the ATP machinery
SS-31, also called elamipretide, is the most clinically advanced compound here. It binds cardiolipin, a phospholipid unique to the inner mitochondrial membrane, and helps preserve cristae structure and electron-transport efficiency under stress (Birk et al. (2013)). In plain terms, it is designed to help damaged mitochondria make ATP more cleanly.
If any compound should improve energy, it is this one. And it is where the honesty rule bites hardest. MMPOWER-3, the Phase 3 trial in primary mitochondrial myopathy, did not meet its primary endpoints: elamipretide failed to beat placebo on the 6-minute walk distance and on the total fatigue score (Karaa et al. (2023)).
That is a genuinely negative result in the exact population you would expect to benefit. Later analyses and other elamipretide programs (Barth syndrome, dry AMD) have shown mixed and sometimes more encouraging signals, but the flagship fatigue trial missed. Researchers dose it 5 to 40 mg subcutaneously daily; the SS-31 dosing chart handles the reconstitution.
CJC-1295 + Ipamorelin: energy through better sleep and recovery
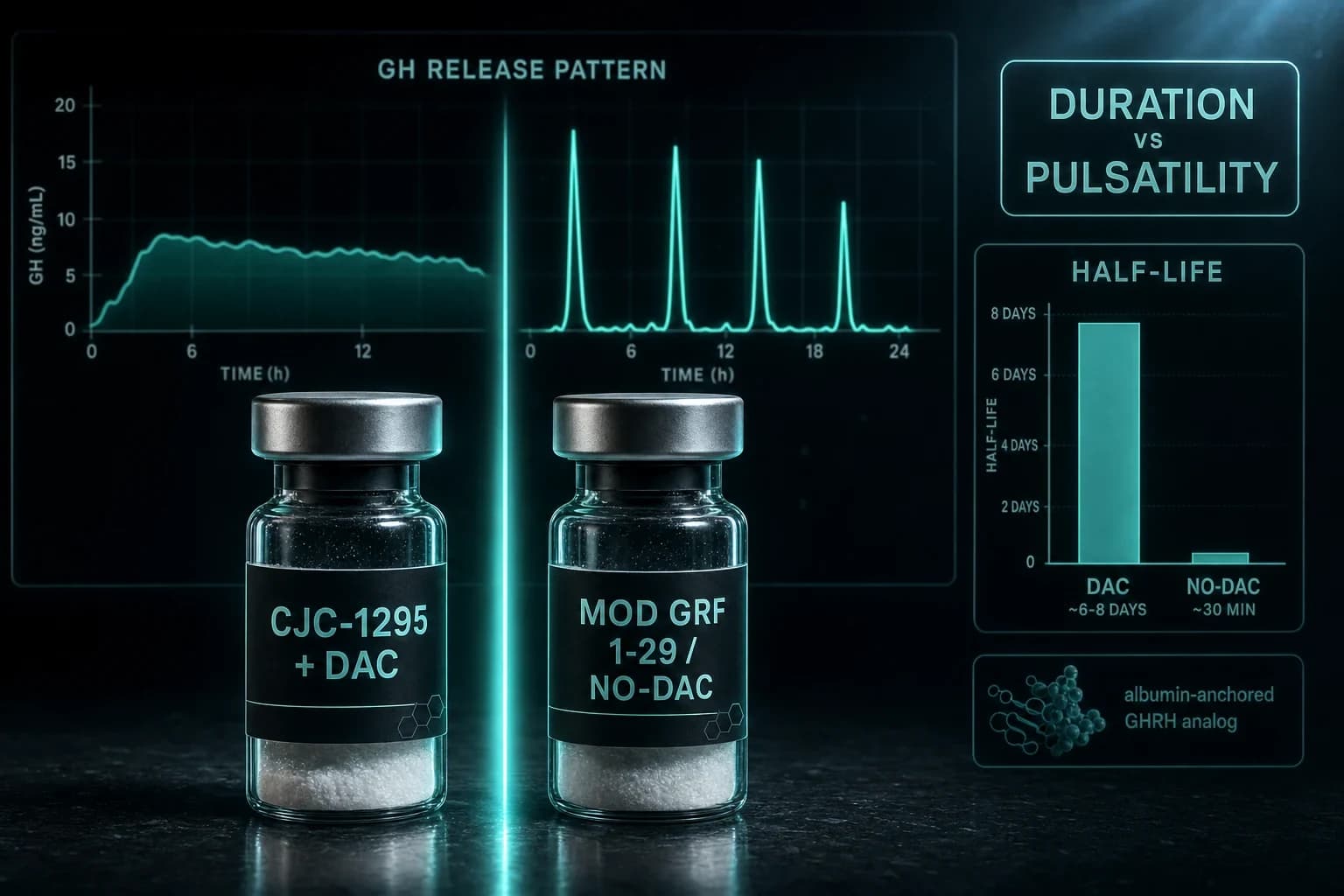
This pairing does not touch mitochondria directly. CJC-1295 is a long-acting GHRH analog and Ipamorelin is a selective ghrelin-receptor agonist; together they push a larger, cleaner pulse of growth hormone. CJC-1295 alone raised mean GH 2- to 10-fold and elevated IGF-1 for up to 11 days after a single dose in healthy adults (Teichman et al. (2006)).
The energy logic is indirect: better GH pulsatility can deepen sleep and speed recovery, and people who sleep and recover better report more daytime energy. That is a reasonable chain, but no trial has measured this stack against a fatigue score. The GH and IGF-1 numbers are human and solid; the energy claim is inference plus anecdote.
Worth flagging: chronically elevated IGF-1 is a growth signal for all tissue, which is a real consideration for anyone with a personal or family cancer history.
MK-677: the oral sleep lever
MK-677 (ibutamoren) is an orally active ghrelin mimetic that raises GH and IGF-1 without an injection, which is most of its appeal. Like the injectable secretagogues, it is not a peptide, and its energy case runs through sleep.
The best evidence is old and still cited for a reason: oral MK-677 increased stage IV (slow-wave) sleep by roughly 50% and REM sleep by more than 20% in healthy young men (Copinschi et al. (1997)). Deeper sleep is one of the more plausible routes to feeling more energetic, so the indirect logic is stronger here than for most of the list.
The trade-offs are real. MK-677 commonly increases appetite, can cause water retention, and raises fasting glucose in some users. Research protocols run it around 10 to 25 mg once daily.
So which peptides for energy actually earn the spot?
Rank by evidence instead of marketing and the picture inverts the typical listicle:
- Best human data, indirect route: MK-677 and the CJC-1295 + Ipamorelin stack, both working through sleep and recovery rather than mitochondria.
- Best human data, direct metabolic route: oral NMN for insulin sensitivity, though not for subjective energy.
- Best mechanism, weakest human proof: MOTS-c and 5-Amino-1MQ, striking in mice, untested in people for energy.
- Most studied, most sobering: SS-31, which missed its flagship fatigue endpoint despite an elegant mechanism.
If you are chasing an energy fix, the least glamorous answer wins: whatever repairs your sleep and metabolic health will out-perform any vial. These compounds are levers on specific pathways, not batteries.
Bottom line: There is no proven "best peptide for energy." The strongest human evidence sits with sleep-improving GH secretagogues (MK-677, CJC-1295 + Ipamorelin) and metabolic NMN, while the flashier mitochondrial names (MOTS-c, SS-31, 5-Amino-1MQ) are either preclinical or missed their key trials.
Warning: None of these compounds is FDA-approved for energy or fatigue. Most are sold for laboratory research only, human safety data is thin to absent, and elevated IGF-1 or glucose carries real trade-offs. Third-party testing is not optional.
Sourcing these compounds
Purity decides whether any protocol means anything. The injectables here (MOTS-c, SS-31, and the CJC-1295 + Ipamorelin pairing) are available from Ascension Peptides with 50% off using code ENHANCED, shipped with per-batch certificates of analysis. The oral options, 5-Amino-1MQ and MK-677 capsules, are handled through Limitless Biotech with code ENHANCED. You can compare the full lineup in the peptide directory.
For research use only. Verify purity, handle reconstitution correctly, and never treat a research vial as a prescribed medicine.
This article is for research and educational purposes only. It is not medical advice, and nothing here is a recommendation to use any compound in humans. The peptides discussed are not approved to treat fatigue or any energy-related condition. Consult a qualified healthcare professional before making any health decision.